
Subscribe to RSS
DOI: 10.1055/a-1067-4271
Needle-knife deroofing of a symptomatic type III choledochal cyst
Publication History
Publication Date:
09 December 2019 (online)


An 11-year-old patient was referred to our endoscopy unit following two bouts of acute pancreatitis of unclear cause. Because autoimmune or toxic causes were ruled out and mutation analysis for cystic fibrosis transmembrane regulator and serine protease inhibitors, Kazal type 1, was unrevealing, cross-sectional imaging by magnetic resonance imaging (MRI) ([Fig. 1]) and a subsequent endoscopic ultrasound (EUS) were performed, both showing a cystic structure at the distal common bile duct (CBD) ([Fig. 2], arrow). It was stipulated that local compression of a choledochal cyst could be directly causing the recurrent episodes of acute pancreatitis. The patient therefore consented to undergo endoscopic retrograde cholangiopancreatograpy (ERCP) with sphincterotomy. ERCP revealed a cystic, pre-papillary contrast opacification, findings compatible with a Todani type III choledochocele ([Fig. 3]). Following sphincterotomy, insufficient drainage was achieved because the cystic juxtapapillary lesion remained unchanged ([Fig. 4]). Subsequently, a needle-knife-assisted technique was used (NeedleCut3V, Olympus Medical Systems, Tokyo, Japan), which achieved a successful cystotomy and complete drainage of the choledochal cyst ([Video 1]) [1]. One month later at endoscopic follow-up, resolution of the choledochocele was seen ([Fig. 5]).



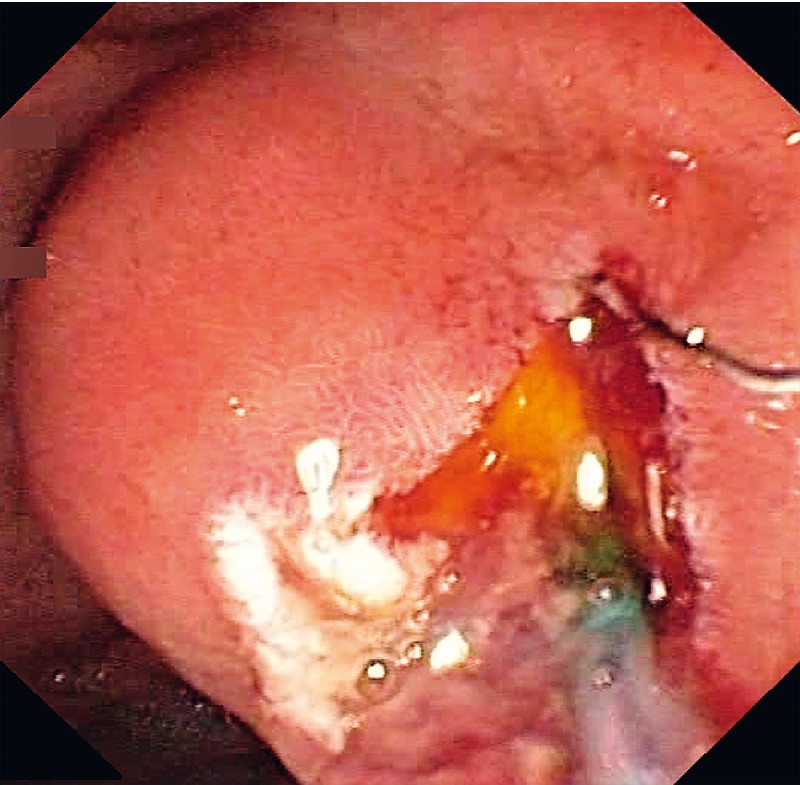
Video 1 Endoscopic treatment of a Todani type III choledochal cyst by needle-knife-assisted deroofing.
Quality:

Described for the first time in 1977, the Todani classification is used for describing the various configurations of choledochal cysts, varying from simple segmental bile duct dilatation (type I) to overt Caroliʼs disease (type V) [2]. Type III choledochal cysts are characterized by a cystic malformation of the distal CBD, typically extending into the duodenal wall, with simultaneous drainage of the CBD and pancreatic duct into the cyst. This increases intralesional pressure, which may give rise to cholangitis and pancreatitis by inducing reflux of pancreatobiliary fluids [3]. Unique to type III cysts, treatment typically consists of a simple sphincterotomy. However, our case illustrates that when sphincterotomy fails, needle-knife-assisted cystotomy can provide sufficient drainage in patients with type III choledochal cysts. After 3 years of follow-up, the patient has remained asymptomatic.
Endoscopy_UCTN_Code_TTT_1AR_2AK
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
-
References
- 1 Mangiavillano B, Parodi A, Conio M. Endoscopic ultrasound-guided ERCP in the treatment of a Todani type-III cyst causing acute necrotizing pancreatitis. Endoscopy 2016; 48 (Suppl. 01) E44
- 2 Todani T, Watanabe Y, Narusue M. et al. Congenital bile duct cysts: classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg 1977; 134: 263-269
- 3 Jablónska B. Biliary cysts: etiology, diagnosis and management. World J Gastroenterol 2012; 18: 4801-4810