
Subscribe to RSS
DOI: 10.1055/a-2001-5289
Intravascular Treatment Techniques for Locoregional Therapies of Lung Tumors
Article in several languages: English | deutsch
Abstract
Background Lung cancer incidence has greatly increased over the past century. Moreover, the lung is the most common site of metastatic involvement. Despite improvements in the diagnosis and treatment of lung malignancies, patient prognosis is still unsatisfactory. Locoregional chemotherapeutic techniques for the treatment of lung malignancies are the current focus of research. The aim of this review article is to present different locoregional intravascular techniques and their treatment principles and to assess the pros and cons of each of them as a palliative and neoadjuvant treatment method in the treatment of lung malignancy.
Method The different methods for the treatment of malignant lung lesions such as isolated lung perfusion (ILP), selective pulmonary artery perfusion (SPAP), transpulmonary chemoembolization (TPCE), bronchial artery infusion (BAI), bronchioarterial chemoembolization (BACE), and intraarteriel chemoperfusion (IACP) are evaluated comparatively.
Results Locoregional intravascular chemotherapy procedures are proving to be promising treatment options in the management of malignant lung tumors. In order to achieve optimal results, the locoregional technique should be used to achieve the highest possible uptake of the chemotherapeutic agent into the target tissue with rapid systemic clearance.
Conclusion Among the various treatment options for lung malignancies, TPCE is the best evaluated treatment concept. However, further studies are necessary to define the optimal treatment concept with the best clinical outcomes.
Key Points
-
There are various intravascular chemotherapy methods for the treatment of lung malignancies.
-
Transpulmonary chemoembolization (TPCE) is currently the most extensively evaluated treatment method for lung malignancies.
-
Thermoablation after neoadjuvant chemoperfusion is a promising therapy for treating lung malignancies.
Citation Format
-
Vogl TJ, Mekkawy A, Thabet DB. Intravascular Treatment Techniques for Locoregional Therapies of Lung Tumors. Fortschr Röntgenstr 2023; 195: 579 – 585
#
Key words
chemoembolization - interventional procedures - pulmonary metastases - lung cancer - locoregional techniquesIntroduction
Lung cancer continues to be the most commonly diagnosed malignant solid tumor. In spite of the numerous treatment options, it is still one of the main causes of cancer-related death. Despite the numerous treatment options, lung cancer was the second most commonly diagnosed cancer (11.4 %) and the most common cause of cancer-related death (20 %) in the year 2020 [1]. Among men, it is the most common cause of cancer-related morbidity and mortality while it is the third most common cancer in women after breast cancer and colon cancer and is the second most common cause of cancer-related mortality after breast cancer. Moreover, with the exception of the lymph nodes, the lung is the most common site of metastatic involvement in all invasive malignant diseases with an estimated cumulative incidence of 20–50 % for non-pulmonary malignancies. In the case of sarcomas, the lung is often even the only organ with metastases, with isolated pulmonary metastases occurring in up to 20 % of patients with sarcoma over the course of their disease [2]. In patients with metastatic melanoma, isolated pulmonary metastases are seen in 2–11 % of patients. In renal cell carcinoma, the lung is involved either as the only organ or as part of multiple metastases in 75 % of cases. Isolated metastases in the lung are common. However, singular metastases are seen in only 1–4 % of cases [3]. The 5-year survival rate of patients with bronchogenic carcinoma (approximately 18 %) is highly dependent on factors like disease stage and treatment modality and ranges from 4 % to 28 %. Therefore, for example, the median survival time is 31.4 months for stage IIIB patients who underwent surgical resection vs. 12.9 months in patients who did not undergo surgery [4].
In spite of improved diagnosis and treatment methods, the prognosis of patients is still unsatisfactory [5] since every treatment option has limitations. Although surgical resection is still the best treatment option for patients with early-stage non-small cell lung cancer and for patients with a limited number of pulmonary metastases of extrathoracic origin, it is only indicated for a minority of patients due to either comorbidities or an advanced disease stage (in approx. 70 % of patients) [5]. The ability to perform simultaneous biopsies for further molecular analyses and tumor verification is a further advantage of resection and ablation. This is in contrast to transarterial and transvenous embolization and radiation. The disadvantages of resection are stress on the patient due to general anesthesia, postoperative pain syndrome particularly in extensive metastasis resection, and reduction of functional lung parenchyma. Prior treatments like radiation also affect the lung parenchyma.
Systemic chemotherapy also offers only a limited treatment option for patients with advanced bronchogenic carcinoma [6] or pulmonary metastases due to the minimal improvement in survival rate [7] and the relatively high rate of side effects, resulting in an increased demand for new treatment strategies [8] [9] and support for the development of locoregional chemotherapy techniques. The main goal of regional techniques is to achieve higher drug concentrations in target tumors while reducing side effects [6]. In combination with biopsy and local ablation, tumor verification and molecular analysis can be subsequently performed. Based on a review of the literature, the most important locoregional chemotherapy techniques for treating malignant pulmonary diseases are isolated lung perfusion (ILP), selective pulmonary artery perfusion (SPAP), transpulmonary chemoembolization (TPCE), bronchial artery infusion (BAI), bronchial artery chemoembolization (BACE), intraarterial chemoperfusion (IACP), and thermoablation [10] [11] [12]. Radiation, metastases resection, and ablation are competing methods.
The individual locoregional techniques in the treatment of pulmonary malignancies ([Table 1]) are evaluated in this review article and compared to one another.
1. Isolated lung perfusion (ILP)
Starting in the 1950 s, isolated lung perfusion (ILP) was developed for the treatment of lung tumors to improve the survival of patients with lung metastases. ILP is based on the concept of injecting a high dose of the chemotherapy drug with the lowest systemic toxicity into the lung by cannulation of the pulmonary arteries and veins [13]. The pulmonary artery is surgically exposed and perfused by means of cannulas. An essential element of this approach is extracorporeal circulation, which allows a closed perfusion circuit [14]. In ILP, the local injection of chemotherapeutics into the lung together with local hyperthermia was able to improve absorption and increase the cytotoxic effect of the applied medications [15]. Muller et al. reported that the concentration of chemotherapeutics at the tumor site is double the amount in systemic chemotherapy [16]. Numerous animal studies were able to confirm these promising results [17]. However, ILP has not become clinically established since it is not reproducible. Moreover, the technique which requires either a thoracotomy or other less invasive surgical techniques is very complex [18]. A further complication of ILP is the systemic inflammatory response that often occurs as a result of the secretion and/or release of cytokines [19].
#
2. Selective pulmonary artery perfusion (SPAP)
The goal of this technique in the treatment of lung cancer was to compare the uptake of gemcitabine and carboplatin during selective pulmonary artery perfusion (SPAP) and intravenous infusion (IV). SPAP is performed by means of venous puncture of the femoral vein, insertion of a selective catheter into the pulmonary artery, and further perfusion of chemotherapy drugs. To delay the washout of chemotherapeutic agents out of the lung, the circulation is occluded for approximately 30 minutes so that blood flow ceases. In a study by van Putte et al. [20], SPAP with carboplatin and/or gemcitabine had better uptake of cytostatics into the lung and mediastinal lymph nodes compared to intravenous infusion. However, the systemic absorption for both techniques was the same. In a further animal study by Den Hengst et al. [21], the authors concluded that the survival rate after the treatment of lung metastases of sarcomas with the SPAP technique using melphalan is just as effective as ILP but is significantly better than systemic intravenous injection of melphalan.
#
3. Transpulmonary chemoembolization (TPCE)
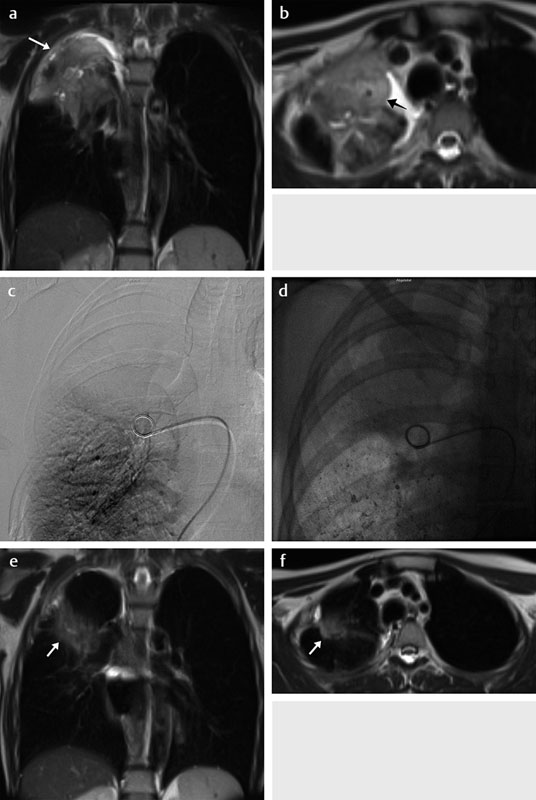
A further alternative is transpulmonary chemoembolization (TPCE) ([Fig. 1]). This is a reproducible percutaneous method that makes invasive methods superfluous [17] [22]. In this technique transfemoral placement of an endovascular 5F sheath and a 5F headhunter catheter is performed under fluoroscopy guidance and these are advanced until the pulmonary artery and then the tumor-supplying segment of the pulmonary branch are reached. For better results, a balloon catheter (diameter up to 7 mm) is optionally placed [23]. This selective pulmonary artery catheterization results in blocking of the arterial supply of the tumor tissue resulting in regional ischemic necrosis in the target tumor tissues while decreasing damage to the surrounding normal lung parenchyma. Chemotherapeutic agents are then administered in combination with injection of lipiodol and microspheres [23]. This extends the time that the injected cytostatics remain in the tumors [24] and reduces outflow into the circulatory system [10] [23]. Consequently, the frequency and severity of systemic effects are limited [25]. Other occlusion materials include coils, polyvinyl alcohol, degradable starch microspheres, and gelatin sponges. Initial results showed similar effectiveness to that of ILP and the same superiority compared to systemic chemotherapy [26]. The principle of this treatment technique is similar to that of transarterial chemoembolization (TACE) of liver tumors, which is an established and successful palliative method for treating primary and secondary liver tumors [24]. The transfer of this successful technique from the liver to the lung as a less invasive technique is currently being evaluated with promising initial results [27]. This can be attributed to the dual blood supply of the lungs and the perfusion of lung tumors by microvessels both from the bronchial and the pulmonary blood supply [24] [28] [29]. In TPCE, a high dose of a cytostatic agent is administered directly into the lung with tumor involvement. A systemic load is prevented by the simultaneous embolization of the vessels so that the medication remains exclusively in the target organ ([Fig. 2, ] [Fig. 3]).



Newer approaches using drug-eluting beads for controlled release of the therapeutic agent are still being examined [30]. The present data indicates that TPCE is well tolerated [25]. Initial results showed that the local control and the survival of patients with lung metastases can be improved. Better results were also achieved in combination with ablative therapy as a neoadjuvant treatment [25]. However, randomized controlled studies are still needed.
#
4. Bronchial artery infusion (BAI) and bronchial artery chemoembolization (BACE)
Numerous studies on bronchial artery infusion (BAI) for the treatment of primary lung cancer alone or in an adjuvant or neoadjuvant context can be found in the literature [11] [25] [31] [32] [33]. BAI is also used in combination with radiation therapy and pulmonary artery perfusion. BAI was also used in a very limited scope for the treatment of lung metastases in colorectal cancer [31]. In 1965, the BAI technique was described for the first time by Kahn et al. [32]. It is a reproducible technique that is performed under angiographic guidance with a 5F catheter. The catheter is inserted using a transfemoral approach and advanced to the bronchial artery. Better results were reported in organs with a dual blood supply, particularly when the tumor has a different perfusion source than the primary organ [33]. Superselective catheterization can be performed using a coaxial microcatheter with subsequent injection of mono or combined chemotherapeutic agents.
Sheng et al. reported that BAI is used in the local administration of immunotherapy in lung metastases of hepatocellular carcinoma (HCC) [34]. Kaseda et al. reported that BAI is used in combination with systemic chemotherapy and radiation therapy for the treatment of recurrent thymic large cell carcinoma [35]. In spite of the low reported complication rate of BAI [36], there are some rare but severe complications like spinal cord complications, bronchial or esophageal ulcerations, and the formation of bronchoesophageal fistulas [19].
In bronchial artery chemoembolization (BACE), a combination of cytostatics and embolic agents like lipiodol and EmboCept is injected [11].
#
5. Intraarterial chemoperfusion (IACP)
Intraarterial chemoperfusion (IACP) is a long-established method for the treatment of lung tumors. In the beginning, it was mainly used in a palliative context to improve performance and to reduce complications by applying chemotherapeutic agents as close as possible to the target tumor [37]. IACP was used not only for the treatment of lung tumors but also for other types of tumors [38].
In 1984, Collins [39] reported a theoretical advantage of intraarterial chemotherapy compared to systemic chemotherapy. He determined that the advantage of intraarterial chemotherapy could be maximized by infusing medications with high total body clearance into the vessels that supply the tumor with a low flow rate. Other animal experiments showed that infusion of medications with higher infusion rates resulted in a greater concentration of the medication and sufficient distribution of the medication in the tumor tissue resulting in better clinical results [40].
In numerous other studies, IACP was evaluated in the treatment of various tumor types. In 2013, Vogl et al. [41] examined 39 patients with inoperable or recurrent pleural mesothelioma and treated them with nonselective IACP using mitomycin C, cisplatin, and gemcitabine in a palliative context. The infusion catheter was placed in the aorta at the level of the origin of the tumor-supplying vessel and the chemotherapeutics were injected manually with maximum pressure. A good response rate was achieved with 36 % partial remission (PR), 49 % stabilization (SD), and an average survival time of 14.2 months (range: 2.1–33.1) from the start of treatment. The average time to progression was 2.6 months. They also reported a lower rate of side effects ([Fig. 4]). A relatively good objective and subjective response rate was achieved with IACP. However, data showing the advantage of IACP compared to systemic intravenous chemotherapy regarding the pharmacokinetics of the injected medications and the concentration of the medications in the tumor tissue is still missing.
In the case of pleural mesothelioma, other methods like pleural resection, intensity-modulated radiation, and hyperthermic intrathoracic chemotherapy (HITHOC) can also be considered.
#
6. Thermoablation in lung malignancies as neoadjuvant therapy
In recent years, the treatment of lung cancers with local interventional therapies has increased exponentially [42]. Thermoablation is considered the optimal treatment option for suitable patients, can be performed on an outpatient basis, and is associated with low morbidity and mortality. Thermoablation like laser-induced thermotherapy (LITT), microwave ablation (MWA), radiofrequency ablation (RFA), and cryoablation is based on the destruction of tumor tissue by means of targeted thermal therapy. However, the most important limiting factors are the size of the target tumor (< 3 cm) and the number of lesions per lung (n ≤ 3) [12]. Moreover, the inhomogeneity of the tumor tissue and the lower heat conductivity of the air-filled lung could limit ablation at the tumor margins [43]. Therefore, locoregional chemotherapy is usually needed prior to thermoablation to ensure that it can be safely performed. Stereotactic ablative radiotherapy can also be used here as a competing method [44].
Numerous animal studies examined various periprocedural techniques to improve the efficiency of thermoablation. These include local injection of various medications, e. g. DDMC-p53 gene therapy or lipiodol [45], that attempt to change the tumor microenvironment with the infusion of an NaCl solution in order to reduce the tissue impedance [46] or to close the bronchial or pulmonary artery to reduce heat loss caused by ventilation and perfusion [47]. In 2005, in a retrospective study in patients with lung metastases in colorectal cancer, treatment with chemotherapy was compared to multimodal treatment (including modified pharmacokinetic-modulating chemotherapy, radiation, and radiofrequency ablation (RFA)). The patients treated with multimodal therapy had a significantly higher survival rate. The three-year survival rate was 87.5 % vs. 33.3 % in the chemotherapy group [48]. In other studies, an attempt was made to combine thermoablation with other treatment options like radiation therapy or systemic, liposomal, or regional chemotherapy [10] [29] [49].
In another study, Gadaleta et al. [29] reported that the treatment of non-resectable lung tumors with RFA 48 hours after transpulmonary chemoembolization (TPCE) with drug-eluting beads is technically feasible and well tolerated and has an advantage over RFA alone. Zeng et al. reported that the combination of BACE and drug-eluting beads achieved good results in the treatment of advanced lung cancer [50]. In 2019, Vogl et al. [25] concluded that the combination of TPCE and an ablative therapy produced positive results. The advantages of ablation compared to resection would be the lack of a need for general anesthesia and the decreased loss of functional lung parenchyma.
All studies to date are based on the assumption that the optimization of thermoablation by combining it with other locoregional chemotherapy techniques could allow the treatment of patients with larger lesions and a higher tumor burden [10].
#
#
Conclusion
Locoregional intravascular chemotherapy techniques could be a promising treatment option in the treatment of lung malignancies with fewer side effects than systemic chemotherapy. However, additional studies are needed to define the optimal treatment concept with the best clinical results. For good results, it makes sense to use a locoregional technique to achieve high uptake of the chemotherapeutic agent in target tissue with fast systemic clearance of the chemotherapeutic agent being used. It is also conceivable that the use of these techniques as neoadjuvant methods prior to thermoablation could improve survival rates.
#
#
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Duma N, Santana-Davila R, Molina JR. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin Proc 2019; 94 (08) 1623-1640
- 2 Rau B, Roth C, Schnider A. et al. Chirurgie der Lungenmetastasen extrapulmonaler Primärtumoren. Schweiz Med Forum 2002; 49: 1166-1170
- 3 Branscheid D, Krysa S, Stoelben E. et al. Chirurgische Therapie von Lungenmetastasen beim Nierenzellkarzinom – Diagnostik, Strategie, Ergebnisse. Akt Urol 1992; 23: 107-112
- 4 David EA, Andersen SW, Beckett LA. et al. Survival benefits associated with surgery for advanced non-small cell lung cancer. The Journal of Thoracic and Cardiovascular Surgery 2019; 157 (04) 1620-1628
- 5 Lemjabbar-Alaoui H, Hassan OU, Yang Y-W. et al. Lung cancer: Biology and treatment options. Biochim Biophys Acta 2015; 1856: 189-210
- 6 Minchinton AI, Tannock IF. Drug penetration in solid tumours. Nature Reviews Cancer 2006; 6: 583-592
- 7 Mentzer SJ, Antman KH, Attinger C. et al. Selected benefits of thoracotomy and chemotherapy for sarcoma metastatic to the lung. Journal of Surgical Oncology 1993; 53: 54-59
- 8 Genestreti G, Grossi F, Genova C. et al. Third- and further-line therapy in advanced non-small-cell lung cancer patients: an overview. Future Oncology 2014; 10: 2081-2096
- 9 Ren K, Wang J, Li Y. et al. The Efficacy of Drug-eluting Bead Transarterial Chemoembolization Loaded With Oxaliplatin for the Treatment of Stage III-IV Non-small-cell Lung Cancer. Acad Radiol 2022; 14 S1076-6332(22)00065-4
- 10 Vogl TJ, Shafinaderi M, Zangos S. et al. Regional chemotherapy of the lung: transpulmonary chemoembolization in malignant lung tumors. Semin Interven Radiol 2013; 30: 176-184
- 11 Boas FE, Kemeny NE, Sofocleous CT. et al. Bronchial or Pulmonary Artery Chemoembolization for Unresectable and Unablatable Lung Metastases: A Phase I Clinical Trial. Radiology 2021; 301 (02) 474-484
- 12 Vogl TJ, Nour-Eldin NA, Albrecht MH. et al. Thermal Ablation of Lung Tumors: Focus on Microwave Ablation. Fortschr Röntgenstr 2017; 189 (09) 828-843
- 13 van Putte BP, Hendriks JM, Romijn S. et al. Isolated lung perfusion for the treatment of pulmonary metastases current mini-review of work in progress. Surgical Oncology 2003; 12: 187-193
- 14 Burt ME, Liu D, Abolhoda A. et al. Isolated lung perfusion for patients with unresectable metastases from sarcoma: a phase I trial. Ann Thorac Surg 2000; 69: 1542-1549
- 15 Urano M. Invited Review: For the clinical application of thermo-chemotherapy given at mild temperatures. International Journal of Hyperthermia 1999; 15: 79-107
- 16 Muller H, Hilger R. Curative and palliative aspects of regional chemotherapy in combination with surgery. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 2003; 11: 1-10
- 17 van Putte BP, Hendriks JM, Romijn S. et al. Single-pass isolated lung perfusion versus recirculating isolated lung perfusion with melphalan in a rat model. Ann Thorac Surg 2002; 74: 893-898
- 18 Demmy TL, Wagner-Mann C, Allen A. Isolated lung chemotherapeutic infusions for treatment of pulmonary metastases: a pilot study. Journal of Biomedical Science 2002; 9: 334-338
- 19 Mallick R, Demmy T. Regional lung chemotherapy techniques. Innovations 2011; 6: 1-9
- 20 van Putte BP, Grootenboers M, van Boven WJ. et al. Selective pulmonary artery perfusion for the treatment of primary lung cancer: Improved drug exposure of the lung. Lung Cancer 2009; 65: 208-213
- 21 Den HengstWA, Hendriks JMH, Van Hoof T. et al. Selective pulmonary artery perfusion with melphalan is equal to isolated lung perfusion but superior to intravenous melphalan for the treatment of sarcoma lung metastases in a rodent model†. European Journal of Cardio-Thoracic Surgery 2012; 42: 341-347
- 22 Weksler B, Ng B, Lenert JT. et al. Isolated single-lung perfusion with doxorubicin is pharmacokinetically superior to intravenous injection. Ann Thorac Surg 1993; 56: 209-214
- 23 Lindemayr S, Lehnert T, Korkusuz H. et al. Transpulmonary chemoembolization: a novel approach for the treatment of unresectable lung tumors. Techniques in Vascular and Interventional Radiology 2007; 10: 114-119
- 24 Huppert PE, Geißler F, Duda SH. et al. Chemoembolisation des hepatozellulären Karzinoms: Computertomographische Befunde und klinische Resultate bei prospektiv repetitiver Therapie. Fortschr Röntgenstr 1994; 160: 425-432
- 25 Vogl TJ, Mekkawy AIA, Thabet DB. et al. Transvenous pulmonary chemoembolization (TPCE) for palliative or neoadjuvant treatment of lung metastases. European Radiology 2019; 29: 1939-1949
- 26 Schneider P, Kampfer S, Loddenkemper C. et al. Chemoembolization of the lung improves tumor control in a rat model. Clin Cancer Res 2002; 8: 2463-2468
- 27 Golder WA. Chemoembolisation der Lunge. Der Onkologe 2008; 14: 934-939
- 28 Nguyen-Kim TD, Frauenfelder T, Strobel K. et al. Assessment of bronchial and pulmonary blood supply in non-small cell lung cancer subtypes using computed tomography perfusion. Investigative Radiology 2015; 50: 179-186
- 29 Gadaleta CD, Solbiati L, Mattioli V. et al. Unresectable lung malignancy: combination therapy with segmental pulmonary arterial chemoembolization with drug-eluting microspheres and radiofrequency ablation in 17 patients. Radiology 2013; 267: 627-637
- 30 Lewis AL, Gonzalez MV, Lloyd AW. et al. DC bead: in vitro characterization of a drug-delivery device for transarterial chemoembolization. Journal of Vascular and Interventional Radiology: JVIR 2006; 17: 335-342
- 31 Kitai T, Nomura A, Miki A. et al. [Clinical benefit of bronchial arterial infusion chemotherapy to pulmonary metastasis from colorectal cancer--report of two cases]. Gan to kagaku ryoho Cancer & Chemotherapy 2003; 30: 2125-2128
- 32 Kahn PC, Paul RE, Rheinlander HF. Selective bronchial arteriography and intra-arterial chemotherapy in carcinoma of the lung. Journal of Thoracic and Cardiovascular Surgery 1965; 50: 640-645
- 33 Jiang GM, Zhao JW, Chen YX. et al. [Blood supply of pulmonary metastases and its clinical significance]. Chinese Journal of Cancer 2006; 25: 885-887
- 34 Sheng S, Zheng J, Cui S. et al. Complete remission of multiple lung metastases after ablation of hepatocellular carcinoma by transarterial infusion with the p53 gene. Anti-cancer Drugs 2015; 26: 227-231
- 35 Kaseda S, Shimizu K, Yamane T. et al. Bronchial arterial infusion with cisplatin followed by irradiation successfully treats recurrent stage IVb thymic large cell carcinoma. European journal of Cardio-thoracic Surgery 1999; 16: 471-474
- 36 Koshiishi H, Utsumi K, Tamamoto F. et al. [Evaluation of bronchial arterial infusion (BAI) for high risk lung cancer]. Gan To Kagaku Ryoho 2000; 27: 1907-1910
- 37 Freckman HA, Mendez Jr FL, Maurer ER. et al. Chemotherapy for lung cancer by intra-aortic infusion. Jama 1966; 196: 5-10
- 38 YOSHIKAWA K. Ten Years' Experience With Intra-Aortic Infusion Chemotherapy for Gastrointestinal Malignant Tumors. Japanese Journal of Clinical Oncology 1981; 11: 391-398
- 39 Collins JM. Pharmacologic rationale for regional drug delivery. Journal of Clinical Oncology 1984; 2: 498-504
- 40 Takeda N, Diksic M. Relationship between drug delivery and the intra-arterial infusion rate of SarCNU in C6 rat brain tumor model. Journal of Neuro-oncology 1999; 41: 235-246
- 41 Vogl TJ, Lindemayr S, Naguib NN. et al. Nonselective transarterial chemoperfusion: a palliative treatment for malignant pleural mesothelioma. Radiology 2013; 266: 649-656
- 42 Dempsey PJ, Ridge CA, Solomon SB. Advances in Interventional Oncology: Lung Cancer Cancer. J 2016; 22 (06) 393-400
- 43 Ponder E. The Coefficient of Thermal Conductivity of Blood and of Various Tissues. Journal of General Physiology 1962; 45: 545-551
- 44 Safavi AH, Mak DY, Boldt RG. et al. Stereotactic ablative radiotherapy in T1-2N0M0 small cell lung cancer: A systematic review and meta-analysis. Lung Cancer 2021; 160: 179-186
- 45 Hohenforst-Schmidt W, Zarogoulidis P, Stopek J. et al. DDMC-p53 gene therapy with or without cisplatin and microwave ablation. OncoTargets and Therapy 2015; 8: 1165-1173
- 46 Lee JM, Youk JH, Kim YK. et al. Radio-frequency thermal ablation with hypertonic saline solution injection of the lung: ex vivo and in vivo feasibility studies. European Radiology 2003; 13: 2540-2547
- 47 Oshima F, Yamakado K, Akeboshi M. et al. Lung radiofrequency ablation with and without bronchial occlusion: experimental study in porcine lungs. Journal of Vascular and Interventional Radiology: JVIR 2004; 15: 1451-1456
- 48 Inoue Y, Miki C, Hiro J. et al. Improved survival using multi-modality therapy in patients with lung metastases from colorectal cancer: A preliminary study. Oncology Reports 2005; 14: 1571-1576
- 49 Dupuy DE, DiPetrillo T, Gandhi S. et al. Radiofrequency ablation followed by conventional radiotherapy for medically inoperable stage I non-small cell lung cancer. Chest 2006; 129: 738-745
- 50 Zeng Y, Yin M, Zhao Y. et al. Combination of Bronchial Arterial Infusion Chemotherapy plus Drug-Eluting Embolic Transarterial Chemoembolization for Treatment of Advanced Lung Cancer-A Retrospective Analysis of 23 Patients. J Vasc Interv Radiol 2020; 31 (10) 1645-1653
Correspondence
Publication History
Received: 06 January 2022
Accepted: 04 December 2022
Article published online:
02 March 2023
© 2023. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Duma N, Santana-Davila R, Molina JR. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin Proc 2019; 94 (08) 1623-1640
- 2 Rau B, Roth C, Schnider A. et al. Chirurgie der Lungenmetastasen extrapulmonaler Primärtumoren. Schweiz Med Forum 2002; 49: 1166-1170
- 3 Branscheid D, Krysa S, Stoelben E. et al. Chirurgische Therapie von Lungenmetastasen beim Nierenzellkarzinom – Diagnostik, Strategie, Ergebnisse. Akt Urol 1992; 23: 107-112
- 4 David EA, Andersen SW, Beckett LA. et al. Survival benefits associated with surgery for advanced non-small cell lung cancer. The Journal of Thoracic and Cardiovascular Surgery 2019; 157 (04) 1620-1628
- 5 Lemjabbar-Alaoui H, Hassan OU, Yang Y-W. et al. Lung cancer: Biology and treatment options. Biochim Biophys Acta 2015; 1856: 189-210
- 6 Minchinton AI, Tannock IF. Drug penetration in solid tumours. Nature Reviews Cancer 2006; 6: 583-592
- 7 Mentzer SJ, Antman KH, Attinger C. et al. Selected benefits of thoracotomy and chemotherapy for sarcoma metastatic to the lung. Journal of Surgical Oncology 1993; 53: 54-59
- 8 Genestreti G, Grossi F, Genova C. et al. Third- and further-line therapy in advanced non-small-cell lung cancer patients: an overview. Future Oncology 2014; 10: 2081-2096
- 9 Ren K, Wang J, Li Y. et al. The Efficacy of Drug-eluting Bead Transarterial Chemoembolization Loaded With Oxaliplatin for the Treatment of Stage III-IV Non-small-cell Lung Cancer. Acad Radiol 2022; 14 S1076-6332(22)00065-4
- 10 Vogl TJ, Shafinaderi M, Zangos S. et al. Regional chemotherapy of the lung: transpulmonary chemoembolization in malignant lung tumors. Semin Interven Radiol 2013; 30: 176-184
- 11 Boas FE, Kemeny NE, Sofocleous CT. et al. Bronchial or Pulmonary Artery Chemoembolization for Unresectable and Unablatable Lung Metastases: A Phase I Clinical Trial. Radiology 2021; 301 (02) 474-484
- 12 Vogl TJ, Nour-Eldin NA, Albrecht MH. et al. Thermal Ablation of Lung Tumors: Focus on Microwave Ablation. Fortschr Röntgenstr 2017; 189 (09) 828-843
- 13 van Putte BP, Hendriks JM, Romijn S. et al. Isolated lung perfusion for the treatment of pulmonary metastases current mini-review of work in progress. Surgical Oncology 2003; 12: 187-193
- 14 Burt ME, Liu D, Abolhoda A. et al. Isolated lung perfusion for patients with unresectable metastases from sarcoma: a phase I trial. Ann Thorac Surg 2000; 69: 1542-1549
- 15 Urano M. Invited Review: For the clinical application of thermo-chemotherapy given at mild temperatures. International Journal of Hyperthermia 1999; 15: 79-107
- 16 Muller H, Hilger R. Curative and palliative aspects of regional chemotherapy in combination with surgery. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 2003; 11: 1-10
- 17 van Putte BP, Hendriks JM, Romijn S. et al. Single-pass isolated lung perfusion versus recirculating isolated lung perfusion with melphalan in a rat model. Ann Thorac Surg 2002; 74: 893-898
- 18 Demmy TL, Wagner-Mann C, Allen A. Isolated lung chemotherapeutic infusions for treatment of pulmonary metastases: a pilot study. Journal of Biomedical Science 2002; 9: 334-338
- 19 Mallick R, Demmy T. Regional lung chemotherapy techniques. Innovations 2011; 6: 1-9
- 20 van Putte BP, Grootenboers M, van Boven WJ. et al. Selective pulmonary artery perfusion for the treatment of primary lung cancer: Improved drug exposure of the lung. Lung Cancer 2009; 65: 208-213
- 21 Den HengstWA, Hendriks JMH, Van Hoof T. et al. Selective pulmonary artery perfusion with melphalan is equal to isolated lung perfusion but superior to intravenous melphalan for the treatment of sarcoma lung metastases in a rodent model†. European Journal of Cardio-Thoracic Surgery 2012; 42: 341-347
- 22 Weksler B, Ng B, Lenert JT. et al. Isolated single-lung perfusion with doxorubicin is pharmacokinetically superior to intravenous injection. Ann Thorac Surg 1993; 56: 209-214
- 23 Lindemayr S, Lehnert T, Korkusuz H. et al. Transpulmonary chemoembolization: a novel approach for the treatment of unresectable lung tumors. Techniques in Vascular and Interventional Radiology 2007; 10: 114-119
- 24 Huppert PE, Geißler F, Duda SH. et al. Chemoembolisation des hepatozellulären Karzinoms: Computertomographische Befunde und klinische Resultate bei prospektiv repetitiver Therapie. Fortschr Röntgenstr 1994; 160: 425-432
- 25 Vogl TJ, Mekkawy AIA, Thabet DB. et al. Transvenous pulmonary chemoembolization (TPCE) for palliative or neoadjuvant treatment of lung metastases. European Radiology 2019; 29: 1939-1949
- 26 Schneider P, Kampfer S, Loddenkemper C. et al. Chemoembolization of the lung improves tumor control in a rat model. Clin Cancer Res 2002; 8: 2463-2468
- 27 Golder WA. Chemoembolisation der Lunge. Der Onkologe 2008; 14: 934-939
- 28 Nguyen-Kim TD, Frauenfelder T, Strobel K. et al. Assessment of bronchial and pulmonary blood supply in non-small cell lung cancer subtypes using computed tomography perfusion. Investigative Radiology 2015; 50: 179-186
- 29 Gadaleta CD, Solbiati L, Mattioli V. et al. Unresectable lung malignancy: combination therapy with segmental pulmonary arterial chemoembolization with drug-eluting microspheres and radiofrequency ablation in 17 patients. Radiology 2013; 267: 627-637
- 30 Lewis AL, Gonzalez MV, Lloyd AW. et al. DC bead: in vitro characterization of a drug-delivery device for transarterial chemoembolization. Journal of Vascular and Interventional Radiology: JVIR 2006; 17: 335-342
- 31 Kitai T, Nomura A, Miki A. et al. [Clinical benefit of bronchial arterial infusion chemotherapy to pulmonary metastasis from colorectal cancer--report of two cases]. Gan to kagaku ryoho Cancer & Chemotherapy 2003; 30: 2125-2128
- 32 Kahn PC, Paul RE, Rheinlander HF. Selective bronchial arteriography and intra-arterial chemotherapy in carcinoma of the lung. Journal of Thoracic and Cardiovascular Surgery 1965; 50: 640-645
- 33 Jiang GM, Zhao JW, Chen YX. et al. [Blood supply of pulmonary metastases and its clinical significance]. Chinese Journal of Cancer 2006; 25: 885-887
- 34 Sheng S, Zheng J, Cui S. et al. Complete remission of multiple lung metastases after ablation of hepatocellular carcinoma by transarterial infusion with the p53 gene. Anti-cancer Drugs 2015; 26: 227-231
- 35 Kaseda S, Shimizu K, Yamane T. et al. Bronchial arterial infusion with cisplatin followed by irradiation successfully treats recurrent stage IVb thymic large cell carcinoma. European journal of Cardio-thoracic Surgery 1999; 16: 471-474
- 36 Koshiishi H, Utsumi K, Tamamoto F. et al. [Evaluation of bronchial arterial infusion (BAI) for high risk lung cancer]. Gan To Kagaku Ryoho 2000; 27: 1907-1910
- 37 Freckman HA, Mendez Jr FL, Maurer ER. et al. Chemotherapy for lung cancer by intra-aortic infusion. Jama 1966; 196: 5-10
- 38 YOSHIKAWA K. Ten Years' Experience With Intra-Aortic Infusion Chemotherapy for Gastrointestinal Malignant Tumors. Japanese Journal of Clinical Oncology 1981; 11: 391-398
- 39 Collins JM. Pharmacologic rationale for regional drug delivery. Journal of Clinical Oncology 1984; 2: 498-504
- 40 Takeda N, Diksic M. Relationship between drug delivery and the intra-arterial infusion rate of SarCNU in C6 rat brain tumor model. Journal of Neuro-oncology 1999; 41: 235-246
- 41 Vogl TJ, Lindemayr S, Naguib NN. et al. Nonselective transarterial chemoperfusion: a palliative treatment for malignant pleural mesothelioma. Radiology 2013; 266: 649-656
- 42 Dempsey PJ, Ridge CA, Solomon SB. Advances in Interventional Oncology: Lung Cancer Cancer. J 2016; 22 (06) 393-400
- 43 Ponder E. The Coefficient of Thermal Conductivity of Blood and of Various Tissues. Journal of General Physiology 1962; 45: 545-551
- 44 Safavi AH, Mak DY, Boldt RG. et al. Stereotactic ablative radiotherapy in T1-2N0M0 small cell lung cancer: A systematic review and meta-analysis. Lung Cancer 2021; 160: 179-186
- 45 Hohenforst-Schmidt W, Zarogoulidis P, Stopek J. et al. DDMC-p53 gene therapy with or without cisplatin and microwave ablation. OncoTargets and Therapy 2015; 8: 1165-1173
- 46 Lee JM, Youk JH, Kim YK. et al. Radio-frequency thermal ablation with hypertonic saline solution injection of the lung: ex vivo and in vivo feasibility studies. European Radiology 2003; 13: 2540-2547
- 47 Oshima F, Yamakado K, Akeboshi M. et al. Lung radiofrequency ablation with and without bronchial occlusion: experimental study in porcine lungs. Journal of Vascular and Interventional Radiology: JVIR 2004; 15: 1451-1456
- 48 Inoue Y, Miki C, Hiro J. et al. Improved survival using multi-modality therapy in patients with lung metastases from colorectal cancer: A preliminary study. Oncology Reports 2005; 14: 1571-1576
- 49 Dupuy DE, DiPetrillo T, Gandhi S. et al. Radiofrequency ablation followed by conventional radiotherapy for medically inoperable stage I non-small cell lung cancer. Chest 2006; 129: 738-745
- 50 Zeng Y, Yin M, Zhao Y. et al. Combination of Bronchial Arterial Infusion Chemotherapy plus Drug-Eluting Embolic Transarterial Chemoembolization for Treatment of Advanced Lung Cancer-A Retrospective Analysis of 23 Patients. J Vasc Interv Radiol 2020; 31 (10) 1645-1653



