

Subscribe to RSS
DOI: 10.1055/a-0593-5679
Successful removal of a bezoar: treatment of a rare complication after Billroth II surgery
Authors
Publication History
Publication Date:
09 May 2018 (online)

A 68-year-old man presented to our hospital with paroxysmal abdominal pain for 2 months. He had undergone a Billroth II operation 11 months previously, and esophagogastroduodenoscopy at another hospital 1 month ago had shown an anastomotic ulcer. However, his abdominal pain had not been relieved by administration of strong proton-pump inhibitors.
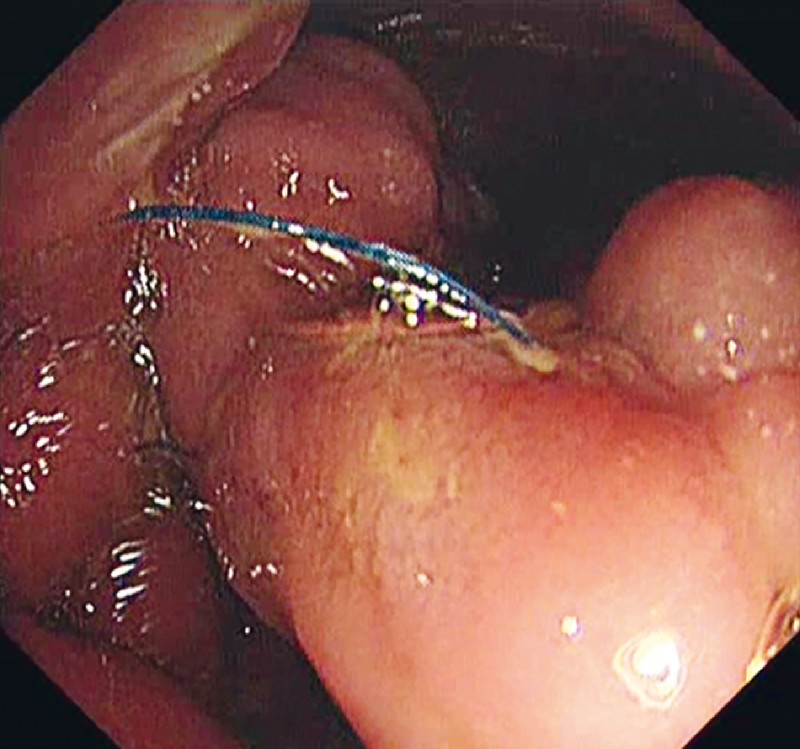
Therefore a computed tomography (CT) scan was performed, which revealed a foreign body in the efferent loop and uneven thickening of the gastric wall ([Fig. 1]). Esophagogastroduodenoscopy at our hospital showed residual sutures, accompanied by ulcers, at the beginning of the efferent loop and anastomosis ([Fig. 2]). To identify the foreign body, the endoscope was deeply inserted into the efferent loop and the afferent loop. We found that the longest sutures were about 10 cm in length, and that their distal ends formed a ring that entangled a bezoar of size 2 cm × 3 cm × 8 cm, hanging deep in the efferent loop ([Fig. 3, ] [Fig. 4]). However, the afferent loop was clear. We suspected that the sutures, which had become free from the anastomosis, had entangled undigested food thus leading to the abdominal pain ([Fig. 5]).




Therefore, stitch scissors were used to cut down the residual sutures. Then we trapped the bezoar and dragged it out using a snare ([Video 1]). The procedure took 40 minutes. The patient’s abdominal pain was relieved promptly and he received medical therapy with aluminum sulfate prokinetics and lansoprazole. Re-examination 1 month later showed both the afferent loop and efferent loop were clear without any discomfort. Of note, we took biopsies during every esophagogastroduodenoscopy and they all revealed chronic inflammation.
Video 1 Endoscopic removal of a bezoar from the afferent loop in a patient with Billroth II anatomy.
Efferent loop syndrome refers to purely mechanical complications in efferent loops following gastrojejunostomy, and bezoars are rare causes of efferent loop syndrome [1]. This is the first case of abdominal pain induced by a bezoar caused by residual sutures, to the best of our knowledge, and we successfully removed the bezoar by endoscopic intervention.
Endoscopy_UCTN_Code_CCL_1AC_2AH
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
-
Reference
- 1 Lee WY, Moon JS. Endoscopic treatment of efferent loop syndrome with insertion of double pigtail stent. World J Gastroenterol 2013; 19: 7209-7212