
RSS-Feed abonnieren
DOI: 10.1055/a-1366-9379
Antiphospholipid Syndrome with Monoclonal Gammopathy—A Mechanism for Recurrent Thrombosis?


Recurrent thromboses are a feature of antiphospholipid syndrome (APS) despite anticoagulation.[1] The mechanism for the development of antiphospholipid (aPL) antibodies remains elusive. Circulating plasmablasts are thought to produce aPL antibodies to domain I of β2-glycoprotein when a cryptic epitope is exposed.[1] [2]
Treatment for thrombotic APS is with long-term anticoagulation. Vitamin K antagonists are the preferred anticoagulant particularly in those with “triple-positive” aPL serology.[3] Khamashta et al described 20 to 40% rates of thrombosis recurrence per year without anticoagulation.[4] Crowther et al showed that with adequate warfarin treatment, the estimated recurrence is 3 to 10% per year.[5] Bazzan et al described rates of thrombosis recurrence after the initial thrombosis of 7.5% over 5 years although 45% were not receiving anticoagulation.[6] The mechanism(s) for thrombosis recurrence despite appropriate anticoagulation remain largely unclear.[1] [6]
Monoclonal gammopathy producing a paraprotein can cause various renal conditions (monoclonal gammopathy of renal significance), AL amyloidosis, and type 1 cryoglobulinemia. In some cases, these may progress to myeloma or lymphoma although many remain within diagnostic thresholds of monoclonal gammopathy of undetermined significance. Paraproteins have been increasingly associated with numerous systemic conditions due to the paraprotein having functional autoantibody activity.[6] These include C1 inhibitor deficiency, acquired von Willebrand syndrome, cutaneous bullous diseases, immunoglobulin M (IgM)-associated peripheral neuropathy, and xanthomatosis.[7] [8] The development of aPL antibodies in the setting of a monoclonal gammopathy may therefore be distinct from those with an autoimmune-driven syndrome. Case reports have described the presence of aPL antibodies in monoclonal gammopathies.[9] [10] [11] [12] [13] [14] Some have had thrombotic events and others have described aPL activity attributed to the identified paraprotein.
We present a group of patients with thrombotic APS found to have an associated monoclonal gammopathy. We recognized this feature in a small number of patients who were found to have thrombosis recurrence despite appropriate anticoagulation.
Patients diagnosed with thrombotic APS at our center with an identifiable paraprotein from January 1, 2015 to January 1, 2020 were reviewed. Cases were age- and gender-matched to patients with thrombotic APS without a paraprotein over this period. Clinical records were reviewed retrospectively for medical history and treatments. Diagnosis was made by Sydney Criteria with methods for aPL detection described previously in accordance with current recommendations.[15] [16] [17] Protein electrophoresis was performed using Capillarys 2 system (Sebia, France).
Nine patients were identified with thrombotic APS with associated monoclonal gammopathy. Their clinical features and treatment are described in [Table 1]. Cryoglobulinemia and hyperviscosity syndrome were not seen. The median age at monoclonal gammopathy diagnosis was 55 years (range: 45–73 years) and median time from first thrombosis to monoclonal gammopathy diagnosis was 10.6 years (range: 2–26 years). The paraprotein immunoglobulin subtype was the same as immunoglobulin subtype of the identified anticardiolipin and/or anti-β2-glycoprotein-1 antibody in all patients.
Abbreviations: ACL, anticardiolipin antibody; APS, antiphospholipid syndrome; β2GP-1, anti β2GP-1 antibody; CAPS, catastrophic antiphospholipid syndrome; CVST, cerebral venous sinus thrombosis; DOAC, direct oral anticoagulant; DRC, dexamethasone, rituximab, cyclophosphamide; DVT, deep vein thrombosis; LA, lupus anticoagulant; MGUS, monoclonal gammopathy of unknown significance; PEX, plasma exchange; PP, paraprotein; R-CVP, rituximab, cyclophosphamide, vincristine, prednisolone; R-CVD, rituximab, cyclophosphamide, dexamethasone.
Comparison was made between those with monoclonal gammopathy and matched controls ([Table 2]). This showed lower rates of other autoimmune conditions and preponderance for arterial events at presentation. Lupus anticoagulant was largely present in both cases (100%) and control (92%). The rate of “triple-positive” serology was 4/9 (44%) versus 12/36 (33%) (Fisher's exact test, p = 0.7) with monoclonal gammopathy versus without.
Abbreviations: AI, autoimmune; aPL, antiphospholipid antibody; APS, antiphospholipid syndrome; SLE, systemic lupus erythematosus.
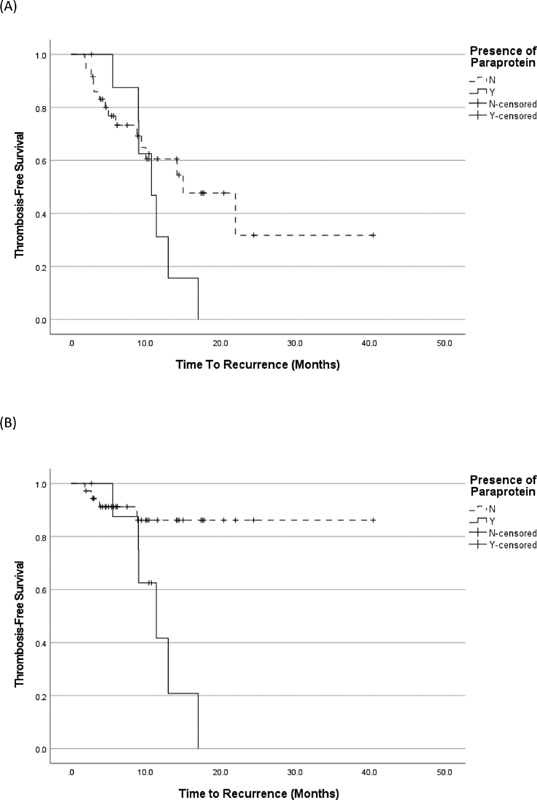
The rates of thrombosis recurrence in all patients with a monoclonal gammopathy were 7/9 (89%) versus 15/36 (42%) in those without (p = 0.058; [Fig. 1A]). Rates of thrombosis recurrence with monoclonal gammopathy while on anticoagulation were 6/9 (67%) versus 4/36 (8%) without (p = 0.002; [Fig. 1B]). Two patients received multiple lines of cytoreductive treatment for lymphoplasmacytic lymphoma. Both patients had a reduction in their IgM paraprotein levels with cytoreduction corresponding to >50% decrease in their IgM aPL titers. One patient received both anticoagulation and ibrutinib resulting in intracranial hemorrhage. Further thrombosis occurred with temporary cessation of anticoagulation. One patient also received monthly plasma exchange in conjunction with anticoagulation, stopping the progression of cerebral small-vessel disease.
We describe a novel finding of monoclonal gammopathy in a small group of patients with thrombotic APS, who demonstrated higher rates of recurrent thrombosis when receiving anticoagulation when compared with those without a paraprotein. In our clinical management of APS with recurrent thromboses, protein electrophoresis is now performed. The overall incidence of paraprotein associated with thrombotic APS is unclear as they are not routinely assessed in APS. This should be the subject of further evaluation. In the interim, we feel that analysis for a paraprotein and subsequent histopathological studies if present should be considered in APS with unexplained recurrent thrombosis, particularly those on appropriate long-term anticoagulation.
Previous case reports have described the presence of aPL antibodies in both plasmacytic and lymphocytic disorders. These cases have demonstrated either incidental aPL antibodies in patients with monoclonal gammopathy or following thrombotic events, for which aPL antibodies were considered as a contributing or causative factor.[9] [10] [11] [12] [13] [14] Other aPL-antibody-mediated conditions such as lupus anticoagulant hypoprothrombinemia syndrome presenting with a bleeding diathesis have been described with multiple myeloma.[18] [19] Paraproteins with aPL-antibody activity in patients with a variety of monoclonal disorders, including myeloma and Waldenström's macroglobulinemia, have been described.[20] [21] [22] [23] [24] [25] Both monoclonal gammopathy and APS are independently associated with an increased risk of thrombosis and therefore thrombotic events may be due to this cumulative effect.[1] [26] However, we suspect that in some patients, the paraprotein has an aPL-antibody activity and therefore is potentially driving this thrombotic tendency particularly in those with higher levels of paraprotein. The next step to test this hypothesis would be to isolate these paraproteins and assess their aPL activity.
Long-term anticoagulation with vitamin K antagonists is advised in patients with thrombotic APS.[26] In those with a paraprotein, targeting the monoclonal disorder may be an additional treatment option. Two patients in our case series received cytoreductive therapy for their associated hematological malignancy with thrombosis recurrence in one patient following lymphoma progression. Considerations of drug interactions, bleeding, and prothrombotic risk must be considered due to the recognized adverse effects of some cytoreductive therapies.
To conclude, the investigation of APS with recurrent thrombosis despite anticoagulation should include protein electrophoresis. This could be considered as a potentially distinct mechanism of thrombotic APS. Optimization of anticoagulation and consideration for cytoreduction to reduce paraprotein levels may be tentative treatment options. This is being explored in other disorders with monoclonal gammopathy causing end-organ damage.[7] Further research is required to define this association: these include the frequency of paraproteins in APS, whether these paraproteins have aPL activity, and lastly, what optimal treatment options are.
Author Contributions
A.J.D. designed the study, collected the data, and wrote the manuscript. K.A.B. and B.J.H. designed the study and critically reviewed the manuscript.
Publikationsverlauf
Eingereicht: 21. Dezember 2020
Angenommen: 18. Januar 2021
Accepted Manuscript online:
20. Januar 2021
Artikel online veröffentlicht:
03. März 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Schreiber K, Sciascia S, de Groot PG. et al. Antiphospholipid syndrome. [published correction appears in Nat Rev Dis Primers. 2018 Jan 25;4:18005] Nat Rev Dis Primers 2018; 4: 17103
- 2 Hisada R, Kato M, Sugawara E. et al. Circulating plasmablasts contribute to antiphospholipid antibody production, associated with type I interferon upregulation. J Thromb Haemost 2019; 17 (07) 1134-1143
- 3 Pengo V, Denas G, Zoppellaro G. et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood 2018; 132 (13) 1365-1371
- 4 Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, Hughes GR. The management of thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med 1995; 332 (15) 993-997
- 5 Crowther MA, Ginsberg JS, Julian J. et al. A comparison of two intensities of warfarin for the prevention of recurrent thrombosis in patients with the antiphospholipid antibody syndrome. N Engl J Med 2003; 349 (12) 1133-1138
- 6 Bazzan M, Vaccarino A, Stella S. et al; Piedmont APS Consortium. Patients with antiphosholipid syndrome and thrombotic recurrences: a real world observation (the Piedmont cohort study). Lupus 2016; 25 (05) 479-485
- 7 Fermand JP, Bridoux F, Dispenzieri A. et al. Monoclonal gammopathy of clinical significance: a novel concept with therapeutic implications. Blood 2018; 132 (14) 1478-1485
- 8 Chen LY, Keddie S, Lunn MP. et al. IgM paraprotein-associated peripheral neuropathy: small CD20-positive B-cell clones may predict a monoclonal gammopathy of neurological significance and rituximab responsiveness. Br J Haematol 2020; 188 (04) 511-515
- 9 Colović N, Miljić P, Colović M, Milosević-Jovcić N. Multiple M components in two patients with splenic lymphoma with villous lymphocytes. Ann Hematol 2006; 85 (01) 51-54
- 10 Dührsen U, Paar D, Kölbel C. et al. Lupus anticoagulant associated syndrome in benign and malignant systemic disease–analysis of ten observations. Klin Wochenschr 1987; 65 (18) 852-859
- 11 von Landenberg P, Schölmerich J, Andreesen R, Vogelhuber M, Lackner KJ. A case of Waldenstroem's disease with a monoclonal IgM antiphospholipid antibody. Rheumatol Int 2002; 22 (03) 129-131
- 12 Wisløff F, Michaelsen TE, Godal HC. Monoclonal IgM with lupus anticoagulant activity in a case of Waldenström's macroglobulinaemia. Eur J Haematol 1987; 38 (05) 456-460
- 13 Hara Y, Makita M, Ishikawa T. et al. Lupus anticoagulant hypoprothrombinemia syndrome in Bence-Jones protein κ-type multiple myeloma patient with phosphatidylserine-dependent antiprothrombin antibody. Ann Hematol 2013; 92 (04) 563-564
- 14 Tait RC, Oogarah PK, Houghton JB, Farrand SE, Haeney MR. Waldenström's macroglobulinaemia secreting a paraprotein with lupus anticoagulant activity: possible association with gastrointestinal tract disease and malabsorption. J Clin Pathol 1993; 46 (07) 678-680
- 15 Miyakis S, Lockshin MD, Atsumi T. et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006; 4 (02) 295-306
- 16 Breen KA, Seed P, Parmar K, Moore GW, Stuart-Smith SE, Hunt BJ. Complement activation in patients with isolated antiphospholipid antibodies or primary antiphospholipid syndrome. Thromb Haemost 2012; 107 (03) 423-429
- 17 Pengo V, Tripodi A, Reber G. et al; Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibody of the Scientific and Standardisation Committee of the International Society on Thrombosis and Haemostasis. Update of the guidelines for lupus anticoagulant detection. J Thromb Haemost 2009; 7 (10) 1737-1740
- 18 Eddou H, Zinebi A, Khalloufi A. et al. Thrombo-haemorrhagic disease-related hypoprothrombinemia-lupus anticoagulant syndrome revealing a light chains multiple myeloma [in French]. J Med Vasc 2018; 43 (05) 325-328
- 19 Yasin Z, Quick D, Thiagarajan P, Spoor D, Caraveo J, Palascak J. Light-chain paraproteins with lupus anticoagulant activity. Am J Hematol 1999; 62 (02) 99-102
- 20 Takamiya O, Machida S, Okuda M, Nojima J, Koreeda C, Kubara K. A non-immunological phospholipid-dependent coagulation inhibitor associated with IgGlambda-type multiple myeloma. Am J Hematol 2004; 75 (01) 34-39
- 21 Wu XY, Yin YF, Teng JL, Zhang LW, Yang CD. IgMk paraprotein from gammopathy patient can bind to cardiolipin and interfere with coagulation assay: a case report. BMC Immunol 2017; 18 (01) 32
- 22 Asherson RA, Davidge-Pitts MC, Wypkema E. “Primary” antiphospholipid syndrome evolving into Waldenstrom's macroglobulinaemia: a case report. Clin Rheumatol 2007; 26 (02) 278-280
- 23 Bellotti V, Gamba G, Merlini G. et al. Study of three patients with monoclonal gammopathies and ‘lupus-like’ anticoagulants. Br J Haematol 1989; 73 (02) 221-227
- 24 Wisløff F, Sletnes KE, Michaelsen T. Shared idiotypic determinant in mono- and polyclonal anti-phospholipid antibodies with lupus anticoagulant activity. Thromb Res 1991; 61 (03) 201-211
- 25 Tektonidou MG, Andreoli L, Limper M, Tincani A, Ward MM. Management of thrombotic and obstetric antiphospholipid syndrome: a systematic literature review informing the EULAR recommendations for the management of antiphospholipid syndrome in adults. RMD Open 2019; 5 (01) e000924
- 26 Crowley MP, Kevane B, O'Shea SI. et al. Plasma thrombin generation and sensitivity to activated protein C among patients with myeloma and monoclonal gammopathy of undetermined significance. Clin Appl Thromb Hemost 2016; 22 (06) 554-562