

Subscribe to RSS
DOI: 10.1055/s-0044-1793808
Intestinal Obstruction in a Toddler Secondary to Betel Nut Ingestion
Authors
Funding None.


We describe the case of a 2-year-old girl with abdominal pain and no passage of flatus or stool for 3 days. These symptoms were not accompanied by vomiting or rectal bleeding, and there was no history of similar episodes. She was born full-term via normal vaginal delivery, with an uneventful birth history.
On physical examination, abdominal distension was noted. An erect abdominal radiograph showed dilated small bowel loops in the central abdomen with multiple air–fluid levels, and ultrasound revealed dilated small bowel loops with to-and-fro peristalsis. Within the distal ileal loop, a well-defined intraluminal round hypoechoic structure with radiating hyperechoic folds and central echogenicity was identified, showing no internal vascularity ([Fig. 1A–C]). On probe compression, mobility of the intraluminal lesion was observed. The absence of a gut signature, telescoping of bowel loops, or attachment to the bowel wall effectively ruled out intussusception and inverted Meckel's diverticulum. Although a mucus plug was considered as a differential, no similar intraluminal structures were observed.
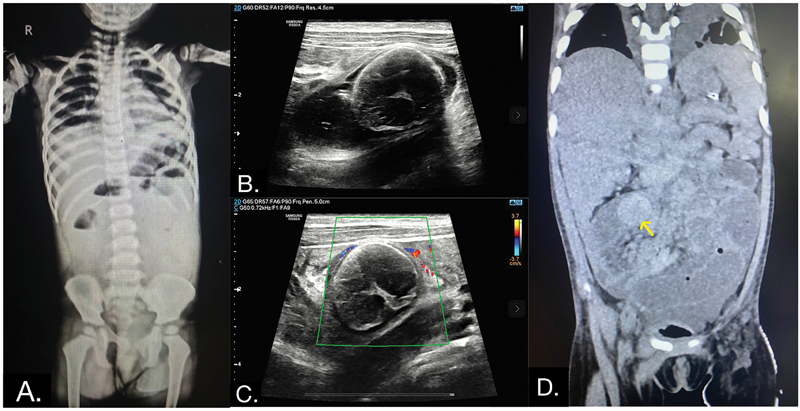
A contrast-enhanced computed tomography (CT) scan was performed, which revealed a round hyperdense intraluminal structure in the mid-ileal loop on plain imaging ([Fig. 1D]), without any contrast enhancement. There was also dilatation of the upstream proximal ileal and jejunal loops. The differentials included foreign body ingestion and a mucus plug. However, we were unable to identify the exact nature of the foreign body, which displayed nonconcerning features such as a round shape and nonsharp edges. The primary concern was the resulting intestinal obstruction, which necessitated surgical intervention.
The patient underwent emergency laparotomy, which revealed an impacted betel nut as the cause of intestinal obstruction ([Fig. 2]). The postoperative period was uneventful.

Foreign body ingestion in children is a frequent occurrence that can lead to serious complications, such as intestinal obstruction, perforation, esophageal stricture, airway obstruction, fistula formation, infection, toxicity, and chronic pain or discomfort. Due to their natural curiosity, children often swallow various objects, including toys, coins, batteries, and food items. These objects can become lodged in the digestive tract, leading to blockages. Timely recognition and intervention are crucial to avoid potentially life-threatening complications, such as intestinal perforation. Studies indicate that approximately 1 in 1,000 children experience foreign body ingestion annually, with 80 to 90% of objects passing through the gastrointestinal tract without intervention.[1] [2]
While most swallowed objects pass without issue, their safe passage depends on factors like size, shape, and composition, as well as the absence of structural abnormalities in the bowel. According to a review by Khorana et al, coins are the most frequently ingested objects, accounting for 57% of cases, followed by batteries (15%), which are associated with higher complication rates.[2] Certain cases may require endoscopic removal or surgery, especially when dealing with magnets, sharp objects, or toxic materials. About 80 to 90% of cases require no intervention; the remaining 10 to 15% may need endoscopic retrieval, which could result in a difficult or unsuccessful attempt that necessitates surgery.[3] Diagnostic imaging plays a critical role in this process. X-rays have 80 to 90% sensitivity for detecting radiopaque foreign bodies, while CT scans offer a higher sensitivity and specificity, exceeding 95%, for visualizing the location and nature of ingested objects.[4]
In addition to foreign bodies, other ileal pathologies in children presenting with abdominal pain include intussusception and inverted Meckel diverticulum. Intussusception is characterized by the intussusceptum filling the lumen of the intussuscipiens, displacing gas, and showing eccentric hyperechoic mesenteric fat adjacent to the intussuscepted bowel segment. Conversely, an inverted Meckel diverticulum does not fill the lumen and is identified by central hyperechoic serosal fat.[5] In our case, although central echogenicity was observed, it did not originate from the bowel wall, lacked the typical gut signature, and showed mobility on probe compression which favors intraluminal foreign body. The distinct echogenic appearance of the impacted betel nut and absence of internal vascularity underscored its nature as a foreign body rather than a viable intraluminal pathological entity.
Intussusception, a leading cause of intestinal obstruction in children aged 3 to 36 months, often presents with intermittent abdominal pain and signs of obstruction. The condition can be complicated by the presence of foreign bodies that may act as lead points.[6]
Beyond foreign objects, phytobezoars—masses formed from indigestible plant material like fibers, seeds, or fruit pits—can also contribute to gastrointestinal obstruction. Phytobezoars are found in 7.5% of patients with small bowel obstruction, with up to 17% occurring in the small intestine.[7] [8] The size, shape, and indigestibility of seeds are key factors in whether they cause blockage. Seed bezoars, a specific type of phytobezoar, are most commonly located in the rectum (78%) and terminal ileum (16%). Due to their small size, they can cross the ileocecal junction and impact the large bowel. Manual disimpaction under general anesthesia is the preferred method for removal, with success in 95% of cases. Complications such as anal fissures may occur in 5% of patients, and surgical intervention might be necessary in some cases.[9] [10]
In conclusion, accurate identification of the type and nature of a foreign body is crucial for effective management and treatment. In this case, the sonographic appearance of the betel nut was distinctive yet challenging, as it was not immediately recognizable. This case underscores the importance of imaging techniques in differentiating between foreign bodies and other intraluminal pathologies.
Publication History
Article published online:
19 November 2024
© 2024. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Jayachandra S, Eslick GD. A systematic review of paediatric foreign body ingestion: presentation, complications, and management. Int J Pediatr Otorhinolaryngol 2013; 77 (03) 311-317
- 2 Khorana J, Tantivit Y, Phiuphong C, Pattapong S, Siripan S. Foreign body ingestion in pediatrics: distribution, management and complications. Medicina (Kaunas) 2019; 55 (10) 686
- 3 Sugawa C, Ono H, Taleb M, Lucas CE. Endoscopic management of foreign bodies in the upper gastrointestinal tract: A review. World J Gastrointest Endosc 2014; 6 (10) 475-481
- 4 Guelfguat M, Kaplinskiy V, Reddy SH, DiPoce J. Clinical guidelines for imaging and reporting ingested foreign bodies. AJR Am J Roentgenol 2014; 203 (01) 37-53
- 5 Hollerweger A, Rieger S, Hübner E, Macheiner P. Sonographic diagnosis of an inverted Meckel diverticulum: distinct criteria enable the correct diagnosis. J Ultrasound Med 2007; 26 (09) 1263-1266
- 6 Mandeville K, Chien M, Willyerd FA, Mandell G, Hostetler MA, Bulloch B. Intussusception: clinical presentations and imaging characteristics. Pediatr Emerg Care 2012; 28 (09) 842-844
- 7 Bouali M, Ballati A, El Bakouri A, Elhattabi K, Bensardi F, Fadil A. Phytobezoar: an unusual cause of small bowel obstruction. Ann Med Surg (Lond) 2021; 62: 323-325
- 8 Hirji SA, Robertson FC, Chao GF, Khurana B, Gates JD. Phytobezoar: a brief report with surgical and radiological correlation. Case Rep Surg 2018; 2018 (01) 5253162
- 9 Caleça Emidio F, Pereira RC, Blanco Saez R, Abegão T, Ribeiro AS. Rectal bezoar: a rare cause of intestinal obstruction. Cureus 2023; 15 (03) e35726
- 10 Ali SW, Usmani SU, Zia A. Seed bezoars as a rare cause of fecal impaction in pediatric patients: a report of two cases from Pakistan. J Pediatr Surg Case Rep 2022; 86: 102457