
Subscribe to RSS
DOI: 10.4103/ijmbs.ijmbs_23_21
Dopa-responsive dystonia: Guanosine triphosphate cyclohydrolase 1, tyrosine hydroxylase, and sepiapterin reductase


Dear Editor,
We read the article entitled “Nephrocalcinosis in genetically proved dopa-responsive dystonia (DRD) due to sepiapterin reductase (SPR) deficiency in a Libyan girl” in this Journal with great interest. Etarhuni et al. reported the case of a female with DRD secondary to SPR deficiency who also presented nephrocalcinosis.[[1]] This unique characteristic was not already reported in other individuals affected by this pathology.
DRD is a very rare (1 in 1 million people) inherited type of dystonia that typically begins during childhood but may begin in adolescence or adulthood. DRD may be caused by the mutations in the guanosine triphosphate cyclohydrolase 1, tyrosine hydroxylase (TH), SPR genes, or the cause may be unknown. These genes are related to the enzymes that are associated with a common pathway responsible for the production of dopamine and serotonin (TH is not related).[[2]] The deficiency of dopamine can lead to a disbalance on the nigrostriatal area leading to dystonia and parkinsonism, mainly in the lower limbs,[[3]] where the most common clinical manifestation is tip-toe walking. A special type of DRD is the Segawa disease (DYT5 dystonia), which is dopa-responsive generalized dystonia, caused by abnormalities of the gene GCH-1 located on chromosomes 14q22.1–q22.2.[[2]]
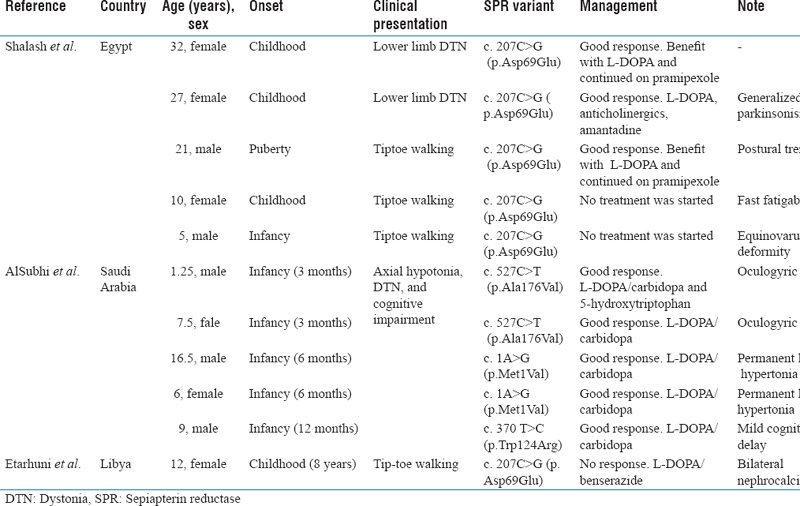
We provided [[Figure 1]] to remember the main metabolic pathway related to DRD. [[Table 1]] is a resume of the main characteristics of the DRD due to SPR deficiency cases from the Middle Eastern and North Africa region.[[1]],[[4]],[[5]] It is interesting to observe that the majority of the patients manifested symptoms during infancy and early childhood. The main clinical presentation was dystonia in the lower limbs, in which the majority had tiptoe walking. Some individuals had unique characteristics such as generalized Parkinsonism, postural tremor, fast fatigability, equinovarus deformity, oculogyric crisis, permanent limb hypertonia, mild cognitive delay, and bilateral nephrocalcinosis. It is worthy of mentioning that the earlier the disease begins, the greater the impairment; also, the cognitive decline is sometimes refractory to treatment.[[5]]

The association of DRD due to SPR deficiency and nephrocalcinosis may be new, but the deposition of calcium in the renal parenchyma and dystonia was already reported with Lesch–Nyhan syndrome (hypoxanthine-guanine phosphoribosyl-transferase deficiency).[[6]] One clinical clue is the localization of dystonia because lower limbs are more commonly associated with DRD. Moreover, the presence of dystonia should be evaluated by a specialist to classify accordingly sometimes other diseases such as adrenoleukodystrophy can present with dystonia[[7]] or even the dystonia could be a benign finding that resolves without treatment.[[8]]
Authors' contributions
Equal.
#
Compliance with ethical principles
Not required.
Reviewers:
Not Applicable
Editors:
Dr Salem A Beshyah (Abu Dhabi, UAE)
#
Financial support and sponsorship
Nil.
Publication History
Received: 11 March 2021
Accepted: 12 March 2021
Article published online:
14 July 2022
© 2021. The Libyan Authority of Scientific Research and Technologyand the Libyan Biotechnology Research Center. All rights reserved. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License,permitting copying and reproductionso long as the original work is given appropriate credit. Contents may not be used for commercial purposes, oradapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India