
Subscribe to RSS
DOI: 10.1055/a-0877-8781
Surgical treatment of varicose veins with the CHIVA method
Article in several languages: deutsch | EnglishKorrespondenzadresse / Correspondence
Publication History
09 November 2018
14 March 2019
Publication Date:
02 May 2019 (online)
- Abstract
- Introduction
- Franceschi shunt classification
- CHIVA treatment strategy
- Treatment of the saphenofemoral junction
- Treatment of incompetent perforating veins
- Treatment of tributary veins
- Pelvic reflux
- Results
- Summary
- Literatur / References
Abstract
In 1988, just after the upcoming of duplex ultrasound, the French vascular surgeon and angiologist Claude Franceschi developed a hemodynamic strategy to treat venous insufficiency on ambulatory patients. He gave the treatment the name of the French acronym. CHIVA.
The strategy is based on the preservation of draining pathways, specially the saphenous veins. The first step consists in an analysis of the recirculation pathway, which was classified by Franceschi into veno-venous shunts, depending on the reflux source and the drainage. Each shunt type requires a special way of treatment to achieve the best result and to avoid superficial thrombosis. The method has found its place in the treatment options in Spain and Italy, actually it is becoming popular in CHINA and the European Eastern Countries, especially in countries, where duplex is common in phlebology diagnostics and financial resources are small.
The method can be applied in each degree of venous illness and chronic venous insufficiency, excepting post-thrombotic saphenous trunks, which might not need to be preserved. A meta-analysis in a Cochrane review certifies that CHIVA produces less side effects and long term recidives with the same immediate results as stripping.
New techniques, like endoluminal (heat) procedures and ultrasound guided foam sklerotherapy help to make the procedure even less invasive in the future.
#
Introduction
Until the 1980 s, there was only one surgical technique for the treatment of trunk vein insufficiency: high ligation and stripping. The strategic consideration behind the stripping procedure was to remove the diseased vein. The procedure was progressively refined and became much less traumatic with the introduction of invaginated stripping and an approach that took the length of reflux in saphenous vein into account [1]. Duplex sonography as the diagnostic method of choice for varicose veins also provides guidance during the therapeutic procedure and has therefore changed treatment options regarding the tactic of ‘eliminating the vein’. Without ultrasonography, ultrasound-guided sclerotherapy, endovenous thermal procedures and extraluminal valvuloplasty would not have been possible.
Duplex ultrasonography has also altered our understanding of the haemodynamics of varicose veins, allowing us to establish the direction of flow and analyse the recirculation pathways – aspects that had been discussed in theory by Trendelenburg and Hach, but never determined in detail or comprehensively for each individual patient.
This analysis allowed Dr Claude Franceschi to classify the recirculation according to the origin of the reflux, its pathway and its drainage in terms of ‘shunts’ [2]. His strategy was to then interrupt the recirculation without removing the vein – with the aim of preserving a functioning trunk vein without disconnecting any venous drainage channels for blood from the skin.
Since 1988, the first theoretical approach has been progressively developed by findings from clinical practice. At the beginning, only surgical techniques were used. But over time other methods such as sclerotherapy and endovenous thermal ablation were then called upon, provided they did not destroy the saphenous vein [3].
This article explains the strategy and addresses the possible state-of-the-art surgical techniques for its implementation.
#
Franceschi shunt classification
Ultrasonography showed that the trunk veins (the great and small saphenous veins) run in a fascial compartment, which differentiates them from other superficial leg veins. Franceschi divided the leg veins into networks – the deep venous network (N1), the trunk veins of the ‘interfascial’ network between the muscle fascia and the saphenous fascia (N2) and the ‘epifascial’ veins (N3) [2], [4]. Blood draining from the leg usually flows from superficial to deep, i. e. from a higher numbered network (N3, the superficial network) into a lower numbered network (N2, the interfascial network, or N1, the deep network). Reflux is present when the direction of the flow is reversed.
Franceschi subdivided the shunts according to the networks concerned and the order, in which they are involved, i. e. the source of the reflux and the drainage pathway. As reflux sources, he considered the reflux N1 → N2 (reflux from the deep veins into the trunk veins, [Fig. 1]) or from other sources (reflux from a perforating vein into a tributary vein, [Fig. 2], then flowing into the trunk vein (N1 → N3 → N2) or from pelvic reflux sources (e. g. veins physiologically draining at the confluence of superficial inguinal veins, in German also known as the Venenstern, as shown in [Fig. 3]). He regarded drainage from the trunk vein into the deep leg vein via a perforating vein (N2 → N1, [Fig. 4a ]) or via a tributary vein connecting to the perforating vein (N2 → N3 → N1, [Fig. 4b ]) as reentry pathways. In order to distinguish between the two pathways, Franceschi and Cappelli developed the reflux elimination test (see [Fig. 4c ]) [5], [6].




The most common shunts are those, in which the reflux
passes from the deep veins, N1, directly into the trunk veins, N2 (N1 → N2), usually across the saphenofemoral or saphenopopliteal junction and more rarely via perforating veins [5].
In a Type 1 shunt (reflux N1 → N3), blood drains from the trunk vein directly to the deep leg vein via a perforating vein (N2 → N1) ([Figures 4a] and [Figures 4c] and [Fig. 5], top left). A Type 3 shunt also has N1 → N2 reflux, but there is no draining perforating vein to be found on the trunk vein. The drainage pathway requires a tributary vein: N2 → N3 → N1 ([Figures 4b] and [Figures 4c] and [Fig. 5], top right).

If the reflux originates from a pelvine tributary that opens at the confluence of superficial inguinal veins or comes from a perforating vein and a tributary into the trunk vein, i. e. a tributary vein is connected between the perforating vein and the trunk vein, we refer to Type 4 or Type 5 shunts, depending on the drainage pathway. Does the flow travel from the saphenous vein to the deep vein directly via a perforating vein (Type 4, [Fig. 3]) or is a tributary vein involved (Type 5, [Fig. 7])?


#
CHIVA treatment strategy
Ambulatory conservative hemodynamic correction of venous insufficiency (CHIVA) aims to interrupt the recirculation pathway without removing the trunk veins. This aim can essentially be achieved by disconnecting the source of reflux, i. e. stopping the pathological transfer from a smaller N to a larger N.
#
Treatment of the saphenofemoral junction
In the case of reflux at the saphenofemoral junction, high saphenous ligation would be the obvious therapeutic step. As with all ablative procedures for varicose veins, this is the region with the most recurrences. Many different procedures and techniques have therefore been developed, such as isolated ligation with non-absorbable suture material, ligation with additional titanium clips, conventional extensive ligation of the saphenofemoral junction without stripping and the endovenous thermal ablation of 7–10 cm in the region of the saphenofemoral junction [7], [8], [9], [10]. In Germany, because of the possible statutory health insurance reimbursement according to the fee schedule (Uniform Evaluation Scale, EBM), only conventional SFJ ligation of the sapheno-femoral junction and all the tributaries or the alternative endovenous occlusion of a short segment distal to the confluence of superficial inguinal veins come into question at this point. A very favourable side effect of short endoluminal ablation distal to the groin tributaries for CHIVA in comparison with extensive saphenofemoral junction ligation is that it continues to allow drainage from the pelvic veins through confluence to the deep leg vein. If additional distal reflux from the saphenous vein into a tributary vein is present, it can be interrupted flush at the level of the trunk vein, either at the same time or at a later date, depending on the individual situation.
However, this is not the only criterion on which the decision is based. Simultaneous ligation of the great saphenous vein and the tributary vein gives very good long-term results with Type 1 shunts [11], [12], [13]. But this is not the case with Type 3 shunts, as superficial venous thrombosis, spider veins on the thigh and a non-draining situation may develop postoperatively, giving rise to the same haemodynamic results as we see after stripping (see [Fig. 5]). For this reason, analysis of the re-entry point is extremely important. If a perforating vein is draining the trunk vein, high saphenous ligation and tributary vein ligation will bring sustained success. If there is no draining perforating vein on the saphenous trunk, the first step is to interrupt the tributary vein, as high ligation alone will lead to persistent tributaries. Alternatively, high ligation may be performed and the tributary vein can be ligated or sclerosed after reduction in diameter [14].
#
Treatment of incompetent perforating veins
First of all, it has to be stated that perforating veins are only incompetent in terms of recirculation when they fill the varicose veins. We can establish this fact with an ultrasound scan examining the perforating vein in pulsed wave (PW) mode. In diastole – the relaxation phase following a provocation manoeuvre – the blood flow in an incompetent perforating vein must be directed outwards (see [Fig. 6a
]) [22]. We can then say that there is reflux and the vein is ‘guilty’ in terms of the recirculation [23]. However, if we find that the blood in a dilated perforating vein flows towards the deep vein, this dilated vein is part of the recirculation drainage and, according to the CHIVA strategy, should therefore not be touched (see
[Figures 6b] and [Figures 6c]).
When reflux from a perforating vein is present – whether it flows directly into the trunk vein or into a tributary vein – interruption of the perforating vein will cut off the source of the reflux. This interruption can be performed surgically, using an endovenous laser technique when the perforating vein runs straight (see figure 6 d) [15] or foam sclerotherapy, if the perforating vein is thin [10], [14], [15].
#
Treatment of tributary veins
The preservation of tributary veins is not the aim of CHIVA. Phlebectomy of tributaries is therefore not inconsistent with CHIVA procedures. However, the associated trauma is often unnecessary, as the tributary veins frequently disappear after the reflux in the trunk vein has been reduced. In the case of a Type 1 shunt, there is an optimal therapeutic situation: the source of reflux from the deep vein into the trunk vein (usually the saphenofemoral or saphenopopliteal junction) is closed and all refluxing tributary veins can be disconnected at their confluence with the trunk vein. The flow still present in the trunk vein drains into the re-entry perforating vein and the tributary veins are no longer filled pathologically (see [Fig. 5], left). But this is not the solution for a Type 3 shunt (see [Fig. 5], right). If the saphenofemoral junction and the tributary vein are disconnected in this case, thrombosis will occur in the trunk vein between the two. Type 3 shunts are therefore more problematic. If only the saphenofemoral junction is disconnected leaving the tributary vein, the distal great saphenous vein will continue to fill the tributary vein, which regresses, but does not disappear from view (see [ Figures 7a ]–[ Figures 7f ]). It can usually then be sclerosed at a later date, if so desired. In cases where the proximal great saphenous vein is of a small diameter, the tributary vein can first be interrupted: this leads to reversal of flow in the trunk vein in 42 % of cases, which lasts for one year and is still present after three years in 29 % (see [Fig. 7f ]) [6]. Surgery must ensure that the tributary is disconnected cleanly from the trunk vein, otherwise there will be an early recurrence (see [Fig. 7g ]).
The optimal situation for isolated tributary vein ligation with the aim of reversing the flow in the trunk vein is a Type 5 shunt – the terminal valve is competent and there is no draining perforating vein on the trunk vein (see [Fig. 8a ]). After disconnecting the tributary vein flush with the trunk vein, a sustained stable reversal of the flow is achieved in 97 % of cases (see [Fig. 8b ]).

#
Pelvic reflux
We often find incontinent pelvic networks after pregnancy, after surgical procedures in the pelvis or when there is a varicocoele. The pelvic network is surrounded by fascia – there are only a few connections with the superficial venous system of the leg. One is across the inguinal canal, another through perineal veins, which lie superficially in the labia and are often considerably dilated during pregnancy. Delfrate and Franceschi developed specific minimally invasive surgical techniques to interrupt these points at the fascial level (16).
#
Results
Time and again it is said of CHIVA that there are no results or long-term studies. Three randomised trials on CHIVA vs stripping are
included in a Cochrane Review; they have a follow-up period of 5–10 years. This confirms that CHIVA has similar initial results with fewer side-effects. The recurrence rate is considerably lower in the CHIVA group [11], [12], [17], [18].
In addition, there are studies on individual situations such as ‘CHIVA 2’, i. e. interruption of a tributary vein [6] or reduction in the diameters of the trunk vein and the deep veins and improvement of measurable parameters such as photoplethysmography [8], [13], [19]. The chapter CHIVA: Results from the literature [20] gives an up-to-date overview.
#
Summary
CHIVA is a surgical strategy to preserve the trunk vein as a drainage pathway. High ligation and tributary vein disconnection provide a good and sustained stable solution for the situation most commonly encountered in phlebology – namely reflux from the deep leg vein across the terminal and preterminal valves (Stücker type 3) with drainage via a perforating vein (Type 1 shunt, about 35 % of patients with an indication for surgery). For Type 5 shunts (reflux from the lesser pelvis with a competent terminal valve) – which is still the case in about 20 % of patients [21] – a complete flow reversal in the trunk vein can be obtained by merely interrupting the tributary vein. It also revolutionises the idea that refluxing trunk veins are permanently damaged and therefore not worth preserving, as many of our colleagues often assert.
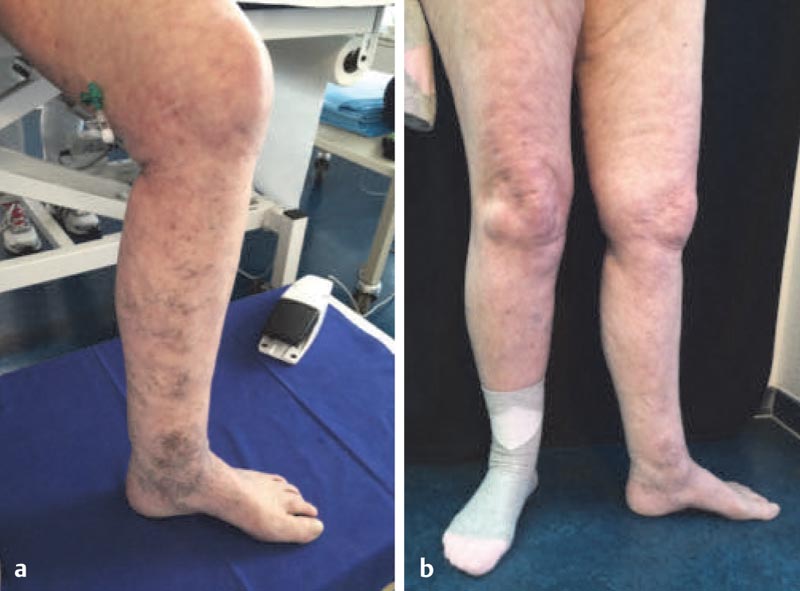
High ligation alone or the endovenous ablation of 7–10 cm of the proximal vein in some situations can considerably improve the clinical picture – allowing patients with comorbidities or on full anticoagulation to be treated with clear symptomatic improvement and minimal side effects (see [Fig. 9]).
The new surgical techniques have made the whole procedure even less traumatic. Many of our colleagues are deterred from learning about the shunt types. However, the classification is actually quite easy – there are two possible sources of reflux and two possible drainage pathways that can be combined to give four types of shunt – thus establishing the rules for treatment. It would be desirable for more doctors to include CHIVA in their therapeutic spectrum for the optimal care of all patients.
#
#
Interessenkonflikt / Conflict of interest
Der Autor gibt an, dass kein Interessenkonflikt besteht.
The authors declare that they have no conflict of interest.
-
Literatur / References
- 1 Hach W, Hach-Wunderle V. Die Wandlung der theoretischen Konzepte in der Chirurgie der Stammvarikose vom 19. Jahrhundert bis in die Gegenwart. Gefäßchirurgie 2001; 6: 111-118
- 2 Franceschi C. Théorie et Pratique de la Cure Conservatrice et Hémodynamique de l’Insuffisance Veineuse en Ambulatoire, Précy-sous-Thil 1988 (Armançon).
- 3 Zamboni P, Mendoza E, Gianesini S. Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 4 Caggiati A, Bergan JJ, Gloviczki P. et al. Nomenclature of the veins of the lower limbs: An international interdisciplinary consensus statement. J Vasc Surg 2002; 36: 416-422
- 5 Mendoza E. CHIVA, ein Handbuch. Arrien Verlag; 2002
- 6 Zamboni P, Gianesini S, Menegatti E. et al. Great saphenous varicose vein surgery without saphenofemoral junction disconnection. British Journal of Surgery 2010; 97: 820-825
- 7 Delfrate R, Bricchi M, Franceschi C. et al. Multiple ligation of the proximal greater saphenous vein in the CHIVA treatment of primary varicose veins. Veins and Lymphatics 2014; 3: 19-22
- 8 Mendoza E, Amsler F. CHIVA with endoluminal procedures: LASER versus VNUS – treatment of the saphenofemoral junction. Phlebologie 2017; 46: 5-12
- 9 Franceschi C, Cappelli M, Ermini S. et al. CHIVA: hemodynamic concept, strategy and results. Int Angiol 2016; 35 (Suppl. 01) 8-30 Epub 2015; 5. Review
- 10 Gianesini S, Delfrate R, Cappelli M. et al. CHIVA Surgical Tips and Tricks. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 11 Carandina S, Mari C, De Palma M. et al. Varicose vein stripping vs. haemodynamic correction (CHIVA): a long term randomised trial. Eur J Vasc Endovasc Surg 2008; 35: 230-237
- 12 Parés JO, Juan J, Tellez R. et al. Varicose vein surgery: stripping versus the CHIVA method: a randomized controlled trial. Ann Surg 2010; 251: 624-631
- 13 Mendoza E. Diameter reduction of the great saphenous vein and the common femoral vein after CHIVA Long-term results. Phlebologie 2013; 42: 65-69
- 14 Mendoza E, Cappelli M. Sclerotherapy technique in CHIVA Strategy. Phlebology 2017; 46: 5-12
- 15 Mendoza E. Duplexsonographie der oberflächlichen Beinvenen. Springer; 2013
- 16 Delfrate R, Mendoza E. Minimally Invasive Surgical Treatment of Pelvic Leak Points. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 17 Iborra-Ortega E, Barjau-Urrea E, Vila-Coll R. et al. Estudio comparativo de dos técnicas quirúrgicas en el tratamiento de las varices de las extremidades inferiores: resultados tras cinco años de seguimiento. ANGIOLOGÍA 2006; 58 (Suppl. 06) 459-468
- 18 Bellmunt-Montoya S, Escribano JM, Dilme J. et al. CHIVA method for the treatment of chronic venous insufficiency. Cochrane Database Syst Rev 2013; 3: CD009648 doi: 10.1002/14651858.CD009648.pub2. Review. Update in: Cochrane Database Syst Rev. 2015:CD009648
- 19 Mendoza E, Berger V, Zollmann C. et al. (Calibre reduction of great saphenous vein and common femoral vein after CHIVA) Kaliberreduktion der V. saphena magna und der V. femoralis communis nach CHIVA. Phlebologie 2011; 40 (Suppl. 02) 73-78
- 20 Mendoza E, Menegatti E. CHIVA Results from literature in. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 21 Zollmann P, Zollmann C, Zollmann P. et al. Determining the origin of superficial venous reflux in the groin with duplex ultrasound and implications for varicose vein surgery. JVS V & L 2017; 5 (Suppl. 01) 82-86
- 22 Mendoza E. Provokationsmanöver zur duplexsonographischen Diagnostik der Varikose. Phlebologie 2013; 42 (Suppl. 06) 357-362
- 23 Mendoza E. Duplex-Untersuchung von Perforansvenen. Phlebologie 2014; 43: 206-209
Korrespondenzadresse / Correspondence
-
Literatur / References
- 1 Hach W, Hach-Wunderle V. Die Wandlung der theoretischen Konzepte in der Chirurgie der Stammvarikose vom 19. Jahrhundert bis in die Gegenwart. Gefäßchirurgie 2001; 6: 111-118
- 2 Franceschi C. Théorie et Pratique de la Cure Conservatrice et Hémodynamique de l’Insuffisance Veineuse en Ambulatoire, Précy-sous-Thil 1988 (Armançon).
- 3 Zamboni P, Mendoza E, Gianesini S. Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 4 Caggiati A, Bergan JJ, Gloviczki P. et al. Nomenclature of the veins of the lower limbs: An international interdisciplinary consensus statement. J Vasc Surg 2002; 36: 416-422
- 5 Mendoza E. CHIVA, ein Handbuch. Arrien Verlag; 2002
- 6 Zamboni P, Gianesini S, Menegatti E. et al. Great saphenous varicose vein surgery without saphenofemoral junction disconnection. British Journal of Surgery 2010; 97: 820-825
- 7 Delfrate R, Bricchi M, Franceschi C. et al. Multiple ligation of the proximal greater saphenous vein in the CHIVA treatment of primary varicose veins. Veins and Lymphatics 2014; 3: 19-22
- 8 Mendoza E, Amsler F. CHIVA with endoluminal procedures: LASER versus VNUS – treatment of the saphenofemoral junction. Phlebologie 2017; 46: 5-12
- 9 Franceschi C, Cappelli M, Ermini S. et al. CHIVA: hemodynamic concept, strategy and results. Int Angiol 2016; 35 (Suppl. 01) 8-30 Epub 2015; 5. Review
- 10 Gianesini S, Delfrate R, Cappelli M. et al. CHIVA Surgical Tips and Tricks. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 11 Carandina S, Mari C, De Palma M. et al. Varicose vein stripping vs. haemodynamic correction (CHIVA): a long term randomised trial. Eur J Vasc Endovasc Surg 2008; 35: 230-237
- 12 Parés JO, Juan J, Tellez R. et al. Varicose vein surgery: stripping versus the CHIVA method: a randomized controlled trial. Ann Surg 2010; 251: 624-631
- 13 Mendoza E. Diameter reduction of the great saphenous vein and the common femoral vein after CHIVA Long-term results. Phlebologie 2013; 42: 65-69
- 14 Mendoza E, Cappelli M. Sclerotherapy technique in CHIVA Strategy. Phlebology 2017; 46: 5-12
- 15 Mendoza E. Duplexsonographie der oberflächlichen Beinvenen. Springer; 2013
- 16 Delfrate R, Mendoza E. Minimally Invasive Surgical Treatment of Pelvic Leak Points. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 17 Iborra-Ortega E, Barjau-Urrea E, Vila-Coll R. et al. Estudio comparativo de dos técnicas quirúrgicas en el tratamiento de las varices de las extremidades inferiores: resultados tras cinco años de seguimiento. ANGIOLOGÍA 2006; 58 (Suppl. 06) 459-468
- 18 Bellmunt-Montoya S, Escribano JM, Dilme J. et al. CHIVA method for the treatment of chronic venous insufficiency. Cochrane Database Syst Rev 2013; 3: CD009648 doi: 10.1002/14651858.CD009648.pub2. Review. Update in: Cochrane Database Syst Rev. 2015:CD009648
- 19 Mendoza E, Berger V, Zollmann C. et al. (Calibre reduction of great saphenous vein and common femoral vein after CHIVA) Kaliberreduktion der V. saphena magna und der V. femoralis communis nach CHIVA. Phlebologie 2011; 40 (Suppl. 02) 73-78
- 20 Mendoza E, Menegatti E. CHIVA Results from literature in. in: Zamboni P, Mendoza E, Gianesini S. (Eds) Saphenous Vein-Sparing Strategies in Chronic Venous Disease. Springer; 2018
- 21 Zollmann P, Zollmann C, Zollmann P. et al. Determining the origin of superficial venous reflux in the groin with duplex ultrasound and implications for varicose vein surgery. JVS V & L 2017; 5 (Suppl. 01) 82-86
- 22 Mendoza E. Provokationsmanöver zur duplexsonographischen Diagnostik der Varikose. Phlebologie 2013; 42 (Suppl. 06) 357-362
- 23 Mendoza E. Duplex-Untersuchung von Perforansvenen. Phlebologie 2014; 43: 206-209
