Subscribe to RSS
DOI: 10.1055/a-1029-6494
Authors
Korrespondenzadresse
Publication History
Publication Date:
16 March 2020 (online)

Abstract
High-quality treatment of patients suffering from allergies should be a first priority of ENT specialists. In daily routine of otolaryngologists, allergic diseases play a significant role and have to be diagnosed and treated competently. A multitude of guidelines provide a clear corridor for identification of suitable methods. The most important sensitization tests such as skin tests and the determination of specific IgE in the serum lay the foundations of allergy diagnostics. Nasal provocation tests with allergens as most important and most frequently applied allergen provocation tests can be performed especially by highly qualified ENT specialists. They allow the determination of the clinical relevance of single allergens.
Beside pharmacotherapy and avoidance of allergens, the allergen-specific immunotherapy has a central position in the treatment of allergy diseases. Also in this context, correct indication and targeted selection of the pharmaceutics lead to an increased treatment quality.
In particular complex or severe allergic diseases require specialized and even highly specialized treatment. In Germany, structured requirements for establishing Comprehensive Allergy Centers have been developed. The involvement of otolaryngology in the further development of such centers should be improved.
Sound allergy education and training are the basis for competence and quality of the treatment of allergy patients. In medical studies, allergology is currently underrepresented. In specialization, some basic aspects of allergies are taken into account. The medical education for the additional specialization in allergology is currently changing; it is intended to be simplified but this might lead to devaluation. A full speciality of allergology does currently not exist in Germany.
In particular in the areas of allergy training, allergy research, and in the cooperation of ENT specialists in highly specialized allergy centers, an enormous potential for improvement is seen for the discipline of otolaryngology.
Abstract
High-quality treatment of patients suffering from allergies should be a first priority of ENT specialists. In daily routine of otolaryngologists, allergic diseases play a significant role and have to be diagnosed and treated competently. A multitude of guidelines provide a clear corridor for identification of suitable methods. The most important sensitization tests such as skin tests and the determination of specific IgE in the serum lay the foundations of allergy diagnostics. Nasal provocation tests with allergens as most important and most frequently applied allergen provocation tests can be performed especially by highly qualified ENT specialists. They allow the determination of the clinical relevance of single allergens.
Beside pharmacotherapy and avoidance of allergens, the allergen-specific immunotherapy has a central position in the treatment of allergy diseases. Also in this context, correct indication and targeted selection of the pharmaceutics lead to an increased treatment quality.
In particular complex or severe allergic diseases require specialized and even highly specialized treatment. In Germany, structured requirements for establishing Comprehensive Allergy Centers have been developed. The involvement of otolaryngology in the further development of such centers should be improved.
Sound allergy education and training are the basis for competence and quality of the treatment of allergy patients. In medical studies, allergology is currently underrepresented. In specialization, some basic aspects of allergies are taken into account. The medical education for the additional specialization in allergology is currently changing; it is intended to be simplified but this might lead to devaluation. A full speciality of allergology does currently not exist in Germany.
In particular in the areas of allergy training, allergy research, and in the cooperation of ENT specialists in highly specialized allergy centers, an enormous potential for improvement is seen for the discipline of otolaryngology.
1. Introduction
For every ENT specialist, allergic diseases are relevant, since in Germany one person of three suffers from allergic disease during his/her life [1]. Furthermore, allergies are also relevant in the clinical context of ENT diseases, as co-factors or even as their origin.
Therefore, it is necessary that ENT specialists can perform high-quality prevention, diagnostics, and therapy of allergic diseases. One significant basis to assure this quality is education. Diagnostics and therapy of allergic diseases are consequently already taught in medical specialization of otolaryngologists. After otolaryngology specialization, a subspecialisation in allergology is possible.
The simultaneous or sequential occurrence of atopic diseases – allergic multimorbidity – is very frequently observed [2] [3]. Often these are diseases that are typically assigned to different medical disciplines such as for example allergic asthma and allergic rhinitis that may even trigger each other. Interdisciplinary pathways for diagnostics and therapy but also interdisciplinary training and education are of high relevance.
In clinical routine and in the structure of ENT departments and medical offices, allergology is established to very various extents. With regard to the quality of allergy treatment and education, a basic structure that should be available everywhere can be differentiated from specialized structures in hospitals and medical offices that deal more intensively with diagnostics and therapy of allergy diseases and from highly specific allergy centers.
Quality differences could always be observed. Nowadays, there is the increasing need, the invitation, and finally the political desire to objectify quality, to describe it, and to assure it transparently. For this purpose, quality management is used which is generally also required for the establishment of centers, i. e. also allergy centers. A basic principle is the so-called PDCA cycle [4] consisting of “plan-do-check-act”. Primarily conditions, activities, and treatment pathways are described and made visible. By generating defined patient pathways, operating procedures, and if necessary further documents such as checklists or other forms, the clinical pathways and their basic principles are stratified and obligatorily planned in the institution, fixed (“plan”), and implemented. These requirements display the actual state according to which actions are and shall be performed (“do”). In order to verify the outcome of various aspects (patient outcome, financial effectiveness, efficiency, consumption of resources etc.), representative parameters are considered for verification.
Furthermore, flaws and failures as well as errors in the logistic and practical course are questioned (“check”) and finally also innovations and knowledge gain are implemented. For further improvement, the present pathways and operating procedures as well as other documents are revised and completed that are again implemented in daily routine. Then they are again checked and so on. The objective of this cycle is to achieve new improvements and thus quality increase with every “turn”. Also based on this fact, significant parameters are often presented for certifications. They ought to contribute to transparency and quality assurance. Their selection, however, must be made thoroughly. Parameters are only useful if they reasonably display the quality and if they are suitably assessed. In this context, audits are tools of quality testing and should give suggestions for improvements; their re-evaluation in follow-up audits may then show if the parameters could be actually improved and on the other hand if the implemented suggestions were the best measures.
For this reason, certified institutions have to provide a certain basic quality in order to be and to remain certified. In comparison to non-certified institutions that may potentially also act in a highly qualitative way, the quality in certified institutions is generally more standardized and thus more consistent and in particular more transparent.
Establishing certified allergy centers on one hand as well as structured education and training of physicians in the field of allergy that can be transparently shown by according tests and titles and that is based on a standardized basic requirement is essential for the short- and long-term maintenance of quality of physicians and institutions working in the field of allergology.
Another means of quality assurance in diagnostics and therapy are guidelines that will be focused on in the following chapter and that also follow the basic principle of a PDCA cycle.
2. Allergy guidelines
Guidelines are considered as being one of the most important tools of medical quality management. In Germany, the Association of Scientific Medical Societies (Arbeitsgemeinschaft für medizinische Fachgesellschaften, AWMF) coordinates the implementation of medical guidelines since 1992. The AWMF defines guidelines as systematically developed statements representing the current state of knowledge and designed to help practitioners and patients to make decisions about appropriate health care for specific circumstances. Guidelines are important and effective instruments of quality development in healthcare. Their predominant objective is the improvement of medical treatment by providing current knowledge. Guidelines can be distinguished from knowledge elaborated from other sources (evidence reports, systematic reviews, health technology assessments with or without meta-analyses) by formulating clear operating recommendations that also include a clinical valuation of the significance and applicability of study results. Guidelines must be understood as action and decision making corridors; in justified cases, another option can or even has to be chosen. The applicability of a guideline or single guideline recommendations must be verified in the individual situation based on the principle of indication, consultation, assessment of the preferences, and participative decision making [5].
Guidelines set quality standards because they are developed by experts in a guideline committee based on defined regulations [5]. They are targeted and thus they are designed in cooperation of users and representatives of patient groups. A guideline should reflect the best possible quality standard based on current knowledge that is objectifiable and understandable and does not focus on individual interests of the parties involved. Guidelines may refer to diagnostics, therapy, methods, or all aspects together.
In order to transparently display the quality standard of the single guidelines also to the outside, they are classified in development levels according to their methods. This classification includes important criteria, for example if consensus finding had taken place, if evidence research had taken place, or if all systematic development levels had been passed ([Fig. 1]). This leads to the following categories:

Guidelines should permanently be kept on a high quality level. For this purpose, they need to be regularly verified and revised. This process is also standardized. Five years after implementation, the AWMF removes them from its publication system if they were not updated.
In summary, a guideline provides support for the users in the context of decision making in diagnostics, methods, and therapy but it also provides the possibility for patients to claim quality standards. In individual cases, the non-adherence to these standards may be reasonable or even necessary but it should always be well justified. Guidelines are tools to set quality standards and to describe them transparently and objectively. Their observance is a basic principle of current quality assurance in medicine and thus also in allergology.
In the field of allergology, several guidelines exist of different development levels (S1–S3) and of different up-to-dateness. The AWMF guidelines can be retrieved on the internet (https://www.awmf.org/leitlinien/leitlinien-suche.html). They are also found on the websites of the DGAKI (Deutsche Gesellschaft für Allergologie und Klinische Immunologie; German Society for Allergology and Clinical Immunology); here also the full texts of already expired guidelines are found (https://dgaki.de/leitlinien/).
3. Clinical allergology
Clinical allergology is based on a general and focused allergy history; subsequently targeted stepwise diagnostic prcedures are planned and performed, which represents then the foundations for an effective therapy that should be as specific as possible.
Beside general history taking for which diseases, medication, general complaints but also already known allergies and intolerances are asked, the specific allergy history may be obtained in a more stratified way, e. g. by using standardized questionnaires. They should focus on the type and severity of the complaints as well as the time and circumstances (location, causal) of their occurrence. In this context, scoring systems or visual analogue scales may be used that can improve the estimation of the individual severity and the level of suffering [6].
If the survey is performed repeatedly at different times (e. g. different seasons) or also before or during therapy, a structured questionnaire may contribute to better objectify the course of the disease or to verify the effect of a therapy and thus to assess the treatment quality. Questionnaires of different institutions focusing on various aspects can be retrieved for example on the internet. Especially in the context of scientific exchange between colleagues and multidisciplinary patient presentations, the use of standardized questionnaires contributes to the quality assurance of history taking, to interdisciplinary comparability, and to unbiased information exchange. Since they allow statistical evaluation in cases of appropriate classification, they are already essential for scientific trials for many years.
Depending on the complaints and the affected organs, additional clinical examinations should be performed by specific clinical disciplines. Most frequently, those are dermatologists, pneumologists, pediatricians, and if needed gastroenterologists or ophthalmologists. To sufficiently faciliate interdisciplinary cooperation, the foundation of centers and networks is reasonable. Such a setting should ideally minimize time and information loss via the implementation of defined care pathways for diagnosis and treatment. The connection to well-organized centers does not only improve the diagnostic and therapeutic quality but also the adherence of the patients and thus the outcome.
3.1 Diagnostics
Of course, also the diagnostics of allergy diseases should be performed according to highest quality standards. Different well established and evaluated methods are available. Also in allergy diagnostics basic examinations such as skin tests and the measurement of specific IgE for the most frequent allergens may generally be differentiated from special diagnostics such as performing provocation tests and more complex laboratory methods.
In particular in the field of molecular allergy diagnostics, the possibilities rapidly develop and in many cases they allow significant improvement of the diagnostic specificity.
3.1.1 Sensitization tests
In order to detect an IgE mediated allergic sensitization, skin tests are performed or the concentration of specific IgE in serum is measured.
Cell-mediated allergic reactions (type IV) are identified by means of skin tests (epicutaneous tests). In particular cases, cell-based in vitro tests are performed (e. g. basophil activation test [BAT]).
3.1.1.1 Skin tests
In the context of skin tests, (standardized) allergen solutions are applied into (cutaneous tests) or onto (epicutaneous tests) the skin in order to induce a controlled allergen-specific immune reaction that may then be compared to a positive and negative control.
Exact information about indications, contraindications, and the performance of skin tests is found on the AWMF guideline on skin tests for diagnostics of allergic reactions of the immediate type [7]. The skin prick test is considered as the method of first choice and only in cases of particular questions an intracutaneous test should be performed. If this test procedure is correctly performed and standardized allergen solutions are used, this method shows a good reproducibility as well as a high sensitivity and specificity [8]. This procedure should be performed under standardized conditions and with standardized test solutions and standardized material (lancets) to minimize the potential interindividual variability of the examiners. The type and size of the developing wheals (and the erythema) are used as measure for evaluating the reaction in the context of skin prick tests and intracutaneous tests. The documentation of the test results should also be made in a standardized way. Metric measurement of the wheal diameter is considered as the best method [7]. The semiquantitative measurement that is often applied reveals poorer congruence between single examiners and is not recommended [9].
The test allergens that are applied have to be approved according to the European and German Medicines Act; all test allergens that are currently approved in Germany were approved by the Paul Ehrlich Institute [10]. When allergens are intended to be used for testing that are not approved or available, physicians may themselves produce those test materials. Even if the production and also the application in patients does not necessarily require approval (§ 13 of the Medicines Act), a one-time application (according to § 67 of the Medicines Act) has to be submitted to the responsible supervising authorities (e. g. district government).
Regarding the indication, performance, and interpretation of epicutaneous tests, the S3 guideline on the performance of epicutaneous tests with contact allergens and pharmaceuticals is referred to [11].
3.1.1.2 In vitro allergy diagnostics/specific IgE
Like in every lab diagnostics, also the application of in-vitro diagnostics of allergic diseases has to follow the general standards of “good laboratory practice” (GLP) [12]. In Germany, the Federal Institute for Risk Assessment (Bundesinstitut für Risikobewertung, BfR) is responsible. Generally, exclusively suitable, scientifically proven methods have to be used also the field of allergology.
With regard to the specific execution, indication, and interpretation of the in vitro allergy diagnostics, the corresponding S1 guideline is referred to [13] even if its validity has expired according to the AWMF standards. The revision of this guideline (in the new version as S2k guideline) is in its final phase. In the actualized version, also exact recommendations will be given for the first time regarding molecular allergy diagnostics on the level of a guideline. ([Table 1])
|
Cognitive and method competence Knowledge |
Competence to act Experience and skills |
Reference |
|---|---|---|
|
Allergic and immunologic diseases as well as environmental medicine |
||
|
Basics of type I-IV reactions of allergic diseases |
||
|
Diagnostics of allergic diseases, in particular |
||
|
cutaneous (prick) test, if needed also epi- and intracutaneous tests, unspecific tests, provocation tests |
200 |
|
|
interpretation of allergologic in vitro test procedures |
||
|
Therapy of allergic and pseudo-allergic diseases including development of a therapy plan, e. g. avoidance, drug therapy, specific immunotherapy |
25 |
|
|
Therapy of anaphylaxis according to the severity including anaphylactic shock |
||
In vitro procedures in allergology can measure relevant biomarkers that are relevant for diagnostics and sometimes also for the selection and control of therapy. The key principle that may be applied is that positive test results confirm allergic sensitization – i. e. the “allergy disposition”. However, the clinical relevance is always seen only in combination with respective symptoms or after a positive provocation test with allergens. The clear differentiation between allergic sensitization and allergy disease is highly relevant for consultation and treatment of patients.
The most relevant applications are the measurement of specific IgE and total IgE. The measurement of inflammatory mediators (ECP, tryptase, histamine), cellular test systems for mast cells, basophilic and eosinophilic granulocytes as well as cellular test systems for T-lymphocytes are relevant in more specific cases.
The measurement of allergen specific IgG and IgG4 is methodically standardized and generally reliable. It is commercially available for diagnostics of food-associated complaints and food allergies. However, a guideline that has been written specifically on this topic clearly and strictly refuses the application of this method [14].
In vitro diagnostics provide the possibility of methods that can be optimally standardized, at least regarding antibody and mediator determination, and thus allows a comparability of diagnostics of different sites and at different times. This may significantly contribute to quality consolidation and to benchmarking between single centers.
3.1.2 Provocation testing
The identification of allergic sensitization must not be equated with the presence of allergic disease. Sensitization alone without clinical symptoms is frequently observed – in 48.6% of the Germans allergic sensitization may be confirmed [15] but only a part of these sensitizations is associated with allergic disease [16]. Therefore, it is crucial to assess the clinical relevance of the identified sensitization. In first place, history taking regarding location and time-related correlations between allergen exposition and symptoms must be performed. In many cases, however, no clear correlations can be found. In these frequent situations, controlled provocations with allergens should be performed. They provide the highest diagnostic significance in order to differentiate between clinically irrelevant sensitization and the presence of allergic disease.
Allergen provocation as a diagnostic tool requires a standardized and controlled procedure in order to avoid false positive results and in order to minimize the possible risk for patients. The principle is based on the aspect that allergic reactions of the effector organ are reproduced under controlled and standardized conditions.
In clinical routine, the nasal allergen provocation and the double-blind, placebo-controlled food challenge (DBPCFC) [17] play the most relevant roles. Provocations with pharmaceuticals are an important tool in the diagnosis of hypersensitivity reactions to drugs [18]. More rarely, provocation testing is applied in cases of allergic asthma as bronchial allergen provocation, sting provocation for allergies against insect venom allergies [19] and the atopy patch test for atopic dermatitis [20].
For indication, performance, and interpretation of nasal allergen provocation, a European guideline of the EAACI is available [21]. The project of a German guideline on nasal allergen provocation is submitted to the AWMF.
The quality of these tests also depends on the training and experience of the examiners, the patients’ compliance, the accuracy of the measurement methods (rhinomanometry) as well as the quality of the applied allergens. Assuming a certain “grey area” in the interpretation of the results by the examiners, the quality and comparability of examinations is only possible based on strictly regulated internal measures. They include standardized high-quality trainings of the performing staff, application of high-quality, regularly maintained rhinomanometry devices, standardized provocation solutions, exact instruction of the patients before examination so that they may be as cooperative as possible during the examinations, and discarding of examinations that have not been regularly performed. To support this process, the criteria might be fixed for examiners and patients and the examination procedure might be defined as operating procedure with all details.
With regard to the diagnostics of N-ERD (non-steroidal anti-inflammatory drug exacerbated respiratory disease), an EAACI guideline gives clear information [22]. The oral provocation with aspirin represents the gold standard. Nasal and inhalation provocations may also be appropriate under certain circumstances. Tthese procedures should also be performed in a standardized way – on one hand in order to assure the quality of the diagnostic significance and on the other hand in order to optimize patient safety. In vitro diagnostics are not recommended for this disease.
3.2 Therapy
The treatment of allergic diseases is generally based on the three pillars of allergen avoidance, pharmacotherapy, and allergen-specific immunotherapy (SIT). In order to achieve an optimal outcome, all available therapies must be coordinated. Furthermore, the estimation of the outcome must not only consider the most objective testing and evaluation of examination findings but also the individual perception of the patients. This subjective estimation may be stratified by the use of questionnaires and put into an overall context.
Another important element is the involvement of the patients in the sense of information and training but also their participation in therapy decisions [23] [24] which can improve the quality of therapy.
In the context of allergen avoidance, patient education plays a crucial role. Allergens are not visible so that patients have to learn where and how they are exposed and how they can avoid this exposure. Nowadays, different approaches may support the patient information. First of all, the physician has to talk with the patient after confirmed diagnosis. Information material may be handed out and further information sources may be indicated. Those are services on the internet or apps of different providers, e. g. pollen services of weather portals. For patients with food allergies like for example frequently severe peanut allergies, allergen avoidance is potentially life-saving. However, this does not only concern the patients’ knowledge but also of the patients’ families and their environment. Thus, information about allergies and their triggering substances are also important for groups that go far beyond the affected patients themselves. A systematic investigation of employees of restaurants in Düsseldorf revealed that only 30% could list three important food allergens and the knowledge about food allergies was very poor [25].
For other chronic diseases such as COPD [26] or diabetes mellitus [27] it could be demonstrated that training for “self-management” of the disease contributes to a beneficial outcome. Both aspects contribute to therapy individualization and compliance and thus to its quality. Also information about the effects, side effects, benefit, and purpose of a treatment, single drugs, and in particular of immunotherapy improve the acceptance and thus therapy adherence and of course the outcome.
Depending on the allergic disease, the three mentioned pillars of therapy differ in their relevance and certain therapeutic options are not possible or recommended for some diseases. For example, chronic urticaria should not be treated with SIT. However for insect sting allergies, this therapy approach may be central. In this context, the specific information of the patients by means of an appropriate information medium is essential.
The outcome quality of pharmacotherapy for allergic diseases is most frequently measured in controlled clinical trials. For this purpose, objective parameters such as for example pulmonary function in cases of asthma, symptom scores like nasal symptoms in cases of allergic rhinitis, but also standardized instruments for measurement of the disease-specific (e. g. SNOT22 [28]) or general quality of life (e. g. SF36) are applied. Increasingly, the quality of interventions is also investigated outside of trials in real everyday application (“real world evidence”). Hereby, often less positive effects are observed and an important objective of those studies also consists in identifying those factors that are responsible. Often registry studies, e. g. based on prescription databases, are applied. Exemplarily a trial is mentioned that investigated how frequently a specific immunotherapy was performed to treat allergic rhinitis in Germany [29]. The results are disillusioning because only 7% of the patients received this guideline-recommended therapy. In the near future, such “real world evidence” data will gain significantly in importance since digital tools and the digital assessment may not only increase the quantity but also improve the quality and granularity of disease-relevant data. Combined with new methods for evaluation and display of such information, the significance of classic clinical controlled trials will decrease in comparison to real world evidence [30].
Specific immunotherapy with allergens is very important in many allergic diseases because it is the only treatment method that does not only reduce the symptoms but that also has a disease-modifying effect. In contrast to pharmacotherapy, it can prevent the development of bronchial asthma [31] [32] and reduce the development of new allergic sensitizations [33] [34]. Regarding allergen-specific immunotherapy, an AWMF guideline (S2k) is available [35]. One particularity of this guideline is that it provides regularly revised tables describing a product-specific rating of the preparations that are available in Germany, Switzerland, and Austria. They are based on five criteria that were defined by the responsible workgroup of the AWMF guideline commission. This applies exclusively for the so-called TAV preparations (see below). The question is controversially discussed to what extent evidence-based statements about the effectiveness of the preparations may be made and if this information should be relevant for the choice of the preparation [36] [37] [38] [39]. The authors of the guideline make clear that the table reveals “published evidence”, i. e. if studies have been published regarding the preparations that correspond to the five criteria. This guideline is currently being revised and it will be up-leveled to S3 according to the classification of AWMF regulations.
In 2008, the therapy allergen directive (Therapieallergene Verordnung, TAV) [40] became effective. The legal frame was established for the approval of therapy allergens for the most important allergens (birch, alder, hazel; sweet grass except corn; dust mites; bee and wasp venom). In this way, the quality, safety, and effectiveness of the products that have only been on the market as unapproved individual prescriptions should be assured. The preparations have to be checked by means of approval procedures supervised by the Paul Ehrlich Institute (PEI) with regard to their quality, effectiveness, and safety. This structured process for new approvals is very long and is expected to be finalized in 2026.
Meanwhile, also biologics, i. e. monoclonal antibodies, are approved for the treatment of severe cases of many allergy diseases. In most of the cases, they are applied in addition to other pharmaceuticals. This aspect concerns atopic dermatitis [41], bronchial asthma [42] [43], and chronic spontaneous urticaria [44].
For many other atopic diseases, biologics are investigated in studies or tested apart from their approval [45] [46]. By applying these new medications, the quality of the treatment of severe cases could be significantly improved. This is true for the improvement of the symptoms like for example in atopic dermatitis [47] and chronic spontaneous urticaria [44] as well as for avoiding side effects by reducing the use of systemic glucocorticosteroids in asthma [42].
For the therapy of all frequently observed allergy diseases, German or international guidelines are available that have a high methodical quality.
The orientation of the therapy towards guidelines increases the quality of the treatment outcomes. Bousquet et al. investigated in a randomized controlled trial if treatment standardized according to guidelines leads to better results in allergic rhinitis. For this purpose, two groups of general practitioners were formed; one group performed the treatment in conformity to guidelines while the other group had free therapy choice. The standardized and categorized approach led indeed to better treatment outcomes [48].
Based on the concept of multimorbidity – i. e. the fact that several allergy diseases often occur simultaneously – the international ARIA initiative (Allergic Rhinitis and its Impact on Asthma) that was originally limited to the development and revision of guidelines was extended to an interdisciplinary concept of integrated care pathways with application of medical apps on smartphones that allow daily symptom entry by the patients [6] [24].
The principle of using medical apps for improvement of the symptom assessment and therapy control [49] as well as the increased integration of the patients’ interests in terms of developing treatment pathways [50] will gain in importance.
4. Structure of Allergy Treatment
Diagnostics and therapy of allergy diseases can and should generally be performed on all levels of medical care if the necessary quality standards with regard to education, structure, and performance are available.
It may be differentiated between basic allergy treatment, specialized allergy treatment, and highly specialized allergy treatment in centers. The borders between these areas are fluent and mainly depend on the perspective of the beholder. Nonetheless, there is no doubt that there are complex, severe, or even life-threatening cases that cannot and must not be treated by all physicians who are active in allergology. At the same time, there are allergic diseases that may be easily diagnosed and treated. In the interest of the affected patients, of the physicians, and of the healthcare system it seems to be reasonable to establish criteria that allow classifying the quality of allergy competence as transparently and reliably as possible. However, this is currently possible only to a very limited extent.
The different steps of allergy education will be described later in this manuscript. With regard to the organizational structure, the existence of a specific allergy clinic or allergy sections or departments in hospitals already allows a first rough classification. To a limited extent, the presence and the application of quality management allow drawing conclusions on the quality of performing allergy-related measures. Since many allergy diseases manifest at various organ systems at the same time or sequentially, the existence and the level of structured interdisciplinary cooperation may give hints. These or comparable criteria, however, are not systematically assessed in the field of allergology. Based on this perspective, a very important development is the establishment of certified comprehensive allergy centers according to an initiative of the German Society for Allergology and Clinical Immunology (Deutsche Gesellschaft für Allergologie und Klinische Immunologie [DGAKI]).
4.1 Comprehensive Allergy Center
4.1.1 Definition
The network of comprehensive allergy centers (CAC) [51] was initiated in 2014 by the medical societies of the DGAKI, the German Dermatologic Society (Deutsche Dermatologische Gesellschaft [DDG]), and the German Respiratory Society (Deutsche Gesellschaft für Pneumologie [DGP]). The German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (Deutsche Gesellschaft für Hals-Nasen-Ohren-Heilkunde, Kopf- und Hals-Chirurgie [DGHNOKHC]) is not involved up to now.
The objective of this initiative is a cross-sectional, highly competent treatment of patients in comprehensive allergy centers. The centers ought to assure the medical care on the highest standard in a step-by-step concept with certified quality and oriented towards the most recent state of research. Furthermore, clinical and experimental research as well as education should be assured. According to modern quality management requirements, a specific certification process was developed. Currently, 8 allergy centers are successfully certified as CAC in Germany.
4.1.2 Mode of certification
The criteria and content-related preconditions for certification are defined in a checklist and are the basis for successful certification [52].
4.1.2.1 Structure of a CAC
All departments, institutes, or disciplines that focus on clinical allergology, allergic patients, and/or basic research in this field are invited to become members of a CAC. It is obligatory for a CAC to have at least three members from the disciplines of dermatology, ENT, internal medicine/pneumology, pediatrics, and laboratory medicine. Other members might be for example the disciplines of occupational medicine, physiotherapy, psychosomatics, or research labs with focus on allergology. If needed, also external experts and cooperation partners may be integrated in the CAC. This is necessary, especially when obligatory disciplines are not directly included in the CAC ([Fig. 2]). The interdisciplinary cooperation with different departments and institutions of the CAC is essential for the treatment of complex allergy cases. Due to the daily availability of the partners and the rapid mutual consultation, the CAC should be able to rapidly make joint decisions for diagnostic and therapeutic problems.

A CAC needs to have a steering committee with speaker and representative of the center. The speaker and his representative should dispose of experience in clinical allergy diagnostics, therapy, and education as well as in research. The steering committee decides about the election and nomination of the members and defines the objectives, focus, and development of the allergy center. Furthermore, the contribution of the disciplines and the central quality management have to be coordinated. Further tasks of the steering committee are the public relations work, the cooperation with external and cross-regional institutions such as scientific societies or patient associations as well as the creation of the financial plan and the annual review.
4.1.2.2 External cooperation
One central aspect is the cooperation and integration of referring physicians and the close relation with patients. Announcing and publishing the names of contact persons of the CAC and the description of treatment modalities, staff members, and cooperation partners on a CAC website leads to a direct relation with referring physicians and facilitates the contact to the CAC. The referring physicians have the possibility to participate in CAC circles and to present their patients. In addition, at least once per year meetings for exchange of experiences and for education of the referring physicians are offered by the CAC as well as information events for patients. The satisfaction of the referring physicians is assessed every three years and the one of the patients every year by means of a survey. Also cooperation with local media and self-help groups is desired.
4.1.2.3 Trials
For quality assurance, allergy trials with participation or performance of the university should be primarily coordinated by the CAC. This includes the maintenance of a study list and the study plans, qualification of the staff, and organization of the trials with the necessary infrastructure, e. g. care for study patients and division of the responsibilities between the CAC partners. The trials should also be described on the CAC homepage in order to inform patients and to allow the contact for trial inclusion.
4.1.2.4 Internal quality management
In case conferences that take place at least once every three months, cases with complex allergy problems are discussed on an interdisciplinary level. Furthermore, CAC circles that also take place once every three months provide education about significant allergy-related topics.
In order to assure guideline-conform treatment of the patients, current guidelines, e. g. of the AWMF or the EAACI, are applied as the basis for diagnostics and therapy and the internal guidelines and processes are adapted to the recommendations of the guidelines. For this purpose, the guideline representative implements the current guidelines in the CAC and verifies their up-to-dateness and development. Changes are presented for example in education or CAC circles at least 4 weeks after their appearance.
The current knowledge of physicians and nursing staff in the context of managing emergency intervention has to be proven every year by participating in training units or dealing with a real emergency situation during the working hours. The team leader controls that the physicians can prove their knowledge in allergology by collecting CME points from congresses and trainings or reading specific literature.
Diagnostic and therapeutic procedures such as skin prick test, skin patch test, intracutaneous test, pulmonary function, nasal provocation, the application of allergen-specific immunotherapy, food and drug provocation tests have to be determined in form of protocols, manuals, and standard operating procedures (SOP) and thus be standardized in the CAC.
It must be taken into account that not only medical staff plays an important role for a successful CAC. Already when fixing an appointment, the patient should be directed to the optimal primary institution by trained employees based on targeted anamnestic questions. Care must be intensively involved in the CAC by means of training of the nursing staff in allergology (outpatient and inpatient sector) and in specific allergic diseases as well as diagnostic techniques, e. g. emergency situations. Every staff member is regularly trained in specific education and training courses and also invited to attend CAC case conferences. This concept should also be written down in the catalogue of initiating new nursing staff members. An own or cooperating pharmacy with knowhow in allergology and pharmaceutical manufacturing license should for example be available for manufacturing patient-specific allergen test preparations.
It is also important to have an open failure and error culture and to assess complaints in the CAC. The Critical Incidence Reporting System (CIRS) allows reporting severe incidences and failures such as for example anaphylaxis, confusion of medicines or dosage errors in written form. The incidences are critically discussed, analyzed, and the reasons are investigated. As a consequence, measures should be taken to avoid those mistakes in the future. The complaint management identifies further problems such as the assessment of the satisfaction of patients and referring physicians, it analyzes them and defines measures for quality and performance improvement.
5. Allergology education
Education in allergology should have its basis in medical studies, be incorporated in residency, and deepened in the specialization of allergology. The full speciality of allergology does not exist in Germany up to now.
In the curricula of the medical universities in Germany, allergology is not systematically taught but is at best considered in the context of specific teaching. Currently separate and independent full-time professorships for allergology do not exist at German medical faculties. Basic knowledge in allergologic diseases, however, should be included in medical teaching already because of the enormous prevalence of allergies. Thus a systematic and optimized implementation of allergology should be imperatively required already in medical studies.
The curricula for the disciplines of otorhinolaryngology, pediatrics, dermatology, and internal medicine and pneumology contain teaching in allergology. In this way the education assures the basic treatment of uncomplicated allergic diseases.
After recognition as specialist, the subspecialisation for allergology can be completed after 18 months.
These regulations of the current further education guidelines (Weiterbildungsordnung), however, will not be effective for longer time because after a long preparation, the German Physicians’ Board (Deutscher Ärztetag) and the German Medical Association (Bundesärztekammer) issued new model further education guidelines (Muster-Weiterbildungsordnung, MWBO). However, before becoming effective, the individual regional medical associations (Landesärztekammer) have to adopt them or conclude individual regulations.
In the preamble of the current MWBO [53], the German Medical Association defines further education as the learning of specific medical abilities and skills for performing medical activities. The medical competences and attitudes taught in medical training are deepened in further education for the benefit of the patients. It is characteristic for this education that medical knowledge is extensively applied in the professional activity.
Further education is performed in a structured way in order to achieve the qualification as specialist and to further specialize in additional disciplines or to achieve additional further education.
The defined contents of further education and the durations are minimum requirements. The duration of further education is prolonged individually if the contents cannot be learned within the minimum time frame.
Further education is performed in full-time performance of medical employment at approved education institutions with adequate remuneration. It is performed under supervision of physicians licensed in practical training and theoretical teaching as well as partly by the successful participation in approved courses.
The achievement of further education is assessed based on certificates issued by the teachers and supervisors and on an exam. The successful completion of further education is confirmed by a certificate of recognition.
The recognition as specialist is the evidence for acquired competence. It serves for quality assurance of patient healthcare and citizen orientation.
5.1 Allergology in residency
During the 5-year residency to become specialist in otorhinolaryngology (24 months of basic education and 36 months of further education) already some aspects from the field of allergology are incorporated.
The new version of the MWBO mentions the following in the section of ENT [54]:
This list makes clear that during the specialization in otorhinolaryngology only a small fraction of allergy diagnostics and therapy is necessary to meet the requirements mentioned in the table.
In comparison to the previous MWBO from 2003, no particular changes are visible with regard to allergology. However, the reference number of 25 hyposensitizations was required, in the new version the same number is very generally given for the treatment of allergic and “pseudo-allergic” diseases.
It must be critically mentioned that not all education institutions for otorhinolaryngology in German dispose of the necessary structural conditions in order to perform and thus teach these basic procedures in diagnostics and therapy of allergies.
In order to solve problems of this kind, already many years ago a two-step system was established for assistant physicians in further education. These courses were intended to teach the basics and practical skills in allergology. The Work Group of Clinical Immunology, Allergology, and Environmental Medicine of the DGHNOKHC (Arbeitsgemeinschaft Klinische Immunologie, Allergologie und Umweltmedizin der Deutschen Gesellschaft für Hals-Nasen-Ohren-Heilkunde, Kopf- und Hals-Chirurgie) has established guidelines that were revised in November 2009 and that define the conditions to provide these courses, the number of participants, the contents, and the course program [55].
The comparison with further aspects in the new version of the MWBO shows that also the specialization for dermatology, internal medicine and pneumology, and pediatrics does not include higher requirements to educational contents in allergology [53].
For this reason, an additional qualification plays a particularly important role for competent high-quality diagnostics and therapy of allergic diseases.
5.2 Subspecialisation in allergology
In order to further increase the qualification in allergology, the subspecialisation can be achieved after specialization. The MWBO describes that in completion of specialization, the additional subspecialisation in allergology includes the prevention, identification, and treatment of diseases triggered by allergens and pseudo-allergens of different organ systems including the immunological aspects [56].
Allergic diseases do not only occur very frequently but they are often highly complex and may be life-threatening – e. g. as anaphylactic reactions [57]. These complicated cases, however, require sound and often interdisciplinary treatment by highly qualified specialists in allergology. But also allergy diseases that are not life-threatening are often characterized by an enormous complexity with regard to diagnostics and therapy and require highly qualified care in order to adequately treat the patients. Therefore, high-quality, multidisciplinary, and thorough education is essential.
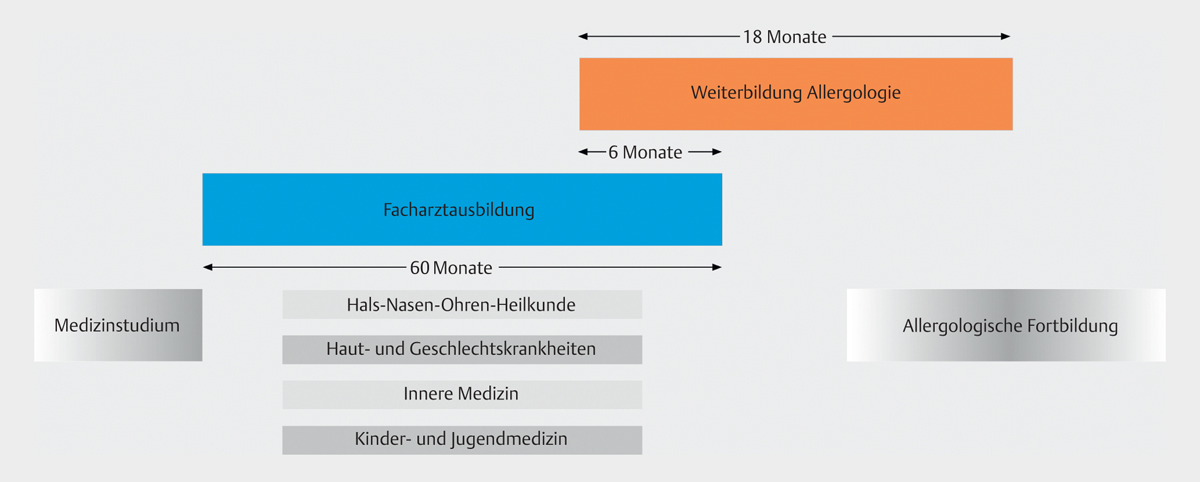
According to the previous version of the subspecialisation guidelines in allergology, this education takes 18 months. It has to be achieved in full-time activity and under supervision of a physician licensed for subspecialisation. Afterwards an exam has to be passed.
In the fields of otorhinolaryngology, dermatology, internal medicine, and pediatrics, six of these 18 months may be acknowledged from the specialization so that there remains a minimum duration of 12 months ([Fig. 3]).

5.3 Planned changes in the subspecialisation guidelines on allergology
At the occasion of the 121st Congress of German Physicians in Erfurt, the revision of the (model) subspecialisation rules (Muster-Weiterbildungsordnung; MWBO) was concluded [58]. This MWBO is the basis for subspecialisation rules of the single regional medical boards. However, the innovations are only applied practically after respective decisions of the regional medical boards that may also change those regulations for their boards and the implementation into healthcare legislation of the federal states. Also the preconditions and minimum intervals for the acquisition of the specializations were defined here.
The suggestion made by the subspecialisation committees regarding allergology (with a subspecialisation period of 12 months) was not concluded but instead a proposed amendment of three delegates was confirmed. This amendment had not been agreed upon with the professional societies and it should allow the additional further qualification as allergologist only as in-service education without specific education periods (or defined course durations) [58].
The discussion around this topic was very controversial [59]. A defined minimum duration of subspecialisation for the specialists in pediatrics, otorhinolaryngology, dermatology, and pneumology should no longer be obligatory in contrast to the still effective regulation of a duration of 18 months. Furthermore, it should be possible to achieve the additional qualification of allergology as “in-service training”.
The specific contents were not concluded in the frame of the congress of physicians but they ought to be elaborated in cooperation with the scientific societies, professional associations, and regional medical boards. Finally, the German Medical Association presented a draft that is now discussed in the committees [56].
Also the European Association of Medical Specialists (UEMS; Union Européenne des Médecins Spécialistes) commented on the planned changes of the medical education in allergology based on the new model subspecialisation regulation in Germany [60]. The UEMS is responsible for the standardization and determination of minimum requirements of medical specialization in Europe which also includes allergology. This open letter states that a full speciality for allergology currently exists in 22 European countries. Only in five European countries – including Germany – allergology is considered as subspecialisation. The planned reduction of the subspecialisation in allergology in Germany is severely criticized and it is explicitly mentioned that not even the minimum requirements for qualification in allergology are fulfilled that have recently been defined in a European position paper with German contribution [61].
Several German scientific societies and professional associations (DGAKI, DGP, DDG, GPA, AeDA, BVDD) contradicted to the decision by means of a letter written to the German Medical Association because they fear that this deterioration of qualification might lead to a poorer quality of healthcare for affected patients.
This led to a new discussion of the MWBO of allergology (in 2018) in the committees of the German Medical Association and an application for amendment was submitted to the 122nd German Congress of Physicians. This application was re-referred to the German Medical Association that finally refused a change of the MWBO of 2018 for allergology (document dated September 30, 2019).
The implementation of these new regulations is now under the responsibility of the regional medical associations that may decide if and how they implement or adjust these amendments.
5.4 International situation
5.4.1 Certification by EAACI
Since 2008, the European Academy of Allergy and Clinical Immunology (EAACI) provides a European exam in allergology and clinical immunology (https://www.eaaci.org/activities/eaaci-exam/upcoming-exam.html) in cooperation with the UEMS (https://www.uems.eu).
This initiative is based on the interest of the UEMS and the EAACI to standardize the qualification in allergology and clinical immunology in Europe [62] and to improve the standard of allergology in Europe. The exam is intended to contribute to the standardization of professional exams in allergology and clinical immunology for European scientific societies, support (allergology-related) societies by providing a written exam on an internationally standardized level and identify medical colleagues who meet the standard of knowledge for continuous professional development.
The exams can be passed every year in the context of the annual meeting of the EAACI in form of a three-hour multiple choice test with 120 items (in English). 70% of the questions are allergology-related and 30% deal with immunologic basics and clinical immunology. A general test is offered, and since 2018 also one focussing on pediatric allergology. The execution and evaluation of the test is performed in cooperation with the Institute for Medical Teaching (Institut für Medizinische Lehre, IML) of the University of Bern, Switzerland (https://www.iml.unibe.ch). The IML also provides an online module for self-assessment in German (https://www.iml.unibe.ch/angebote/assessment/pruefungsdienstleistungen/self-assessment) and English (https://www.iml.unibe.ch/en/offers/assessment-en/exam-services/self-assessment) language.
5.4.2 Allergology in Europe
In most European countries, a medical specialization in allergology (and clinical immunology) is established. A systematic evaluation in Europe by the EAACI and the UEMS that collected data from 37 countries [63] could show that a full speciality of allergology (and clinical immunology) exists in 23 countries (62%). In some countries such as France, Estonia, and Slovenia it was only recently established. In 9 European countries (24%) – including Germany – a subspecialisation can be acquired; and 5 countries (14%) do not even provide a subspecialisation in allergology ([Fig. 4]).

The UEMS and the EAACI request the introduction of a full speciality of allergology in all European countries in order to improve the quality of allergy treatment and to achieve the comparability of the qualifications within Europe [61].
6 Societies and associations
This chapter lists societies and associations that are active in allergology.
Germany
-
Deutsche Gesellschaft für Allergologie und klinische Immunologie (DGAKI)
-
Scientific society
-
Weblink: https://dgaki.de
-
-
Ärzteverband Deutscher Allergologen (AeDA)
-
Professional association
-
Weblink: https://www.aeda.de
-
-
Gesellschaft Pädiatrischer Allergologen (GPA)
-
Umbrella association of regional pediatric allergology/pneumology groups, associated work group of the German Society for Pediatrics (Deutsche Gesellschaft für Kinder- und Jugendmedizin)
-
Weblink: https://www.gpau.de
-
International
-
European Academy of Allergy and Clinical Immunology (EAACI)
-
Scientific society for Europe
-
Weblink: https://www.eaaci.org
-
-
American Academy of Allergy, Asthma, and Immunology (AAAAI)
-
Scientific society for the USA
-
Weblink: https://www.aaaai.org
-
-
World Allergy Organization (WAO)
-
Worldwide association of national allergy societies
-
Weblink: http://www.worldallergy.org
-
7. Conclusion
Many ENT-specific diseases have an allergic basis or at least component. At the same time, many patients suffering from allergies apart from otorhinolaryngology show relevant manifestations in our discipline. Therefore, the quality of qualification in allergology and the competent diagnostics and treatment of these diseases plays a major role for otorhinolaryngologists.
Data support the fact that the incidence, severity, and the complexity of allergies have increased in the last years [64] and will further increase. In order to provide high-quality care of these patients, the optimal education, improved organizational structures, documentation of the quality but also research in allergology are urgently required. This is especially true for otorhinolaryngology because the most frequently occurring allergic diseases manifest in our discipline [65].
In order to meet these requirements, the qualification in allergology must be improved on all levels, i. e. starting with medical studies up to specialization.
In the context of scientific high-quality research in the fields of allergology and immunology, ENT is still underrepresented although our competence provides strategic advantages, for example due to the good exposure or the affected organs (like the nose). It is in our interest but also in the patients’ interest who might benefit from innovative developments to close the gaps and to seize the chances.
The practical performance of allergy diagnostics and therapy should be standardized in all ENT institutions in the interest of the patients but also regarding the qualification. In order to be able to treat severe and complex cases with the necessary quality, the number of highly-specialized and certified allergy centers should be increased involving and actively supported by the field of otorhinolaryngology.
Interessenskonflikt
Honorare für Vorträge und/oder Mitarbeit in wissenschaftlichen Beirat (advisory board): ALK-Abelló, AstraZeneca, Bencard, Genzyme, HAL Allergie, Leti Pharma, Meda Pharma, Novartis, Sanofi Aventis, Stallergenes, Teva Mitgliedschaft /Funktion in Interessenverbänden: DGAKI (Mitglied des engeren Vorstands (Schatzmeister), Sprecher der Sektion HNO), American Academy of Allergy, Asthma & Immunology (AAAAI) (bis 2017 Chair der Sektion IRSO und Annual Meeting Program Committee der AAAAI), DGHNO KHC, EAACI, Gesellschaft für Schädelbasischirurgie (GSB), ERS (European Rhinologic Society).
-
Literatur
- 1 Bergmann KC, Heinrich J, Niemann H. Current status of allergy prevalence in Germany: Position paper of the Environmental Medicine Commission of the Robert Koch Institute. Allergo J Int 2016; 25: 6-10
- 2 Cingi C, Gevaert P, Mösges R. et al. Multi-morbidities of allergic rhinitis in adults: European Academy of Allergy and Clinical Immunology Task Force Report. Clin Transl Allergy 2017; 7: 17
- 3 Bousquet J, Anto JM, Wickman M. et al. Are allergic multimorbidities and IgE polysensitization associated with the persistence or re-occurrence of foetal type 2 signalling? The MeDALL hypothesis. Allergy 2015; 70: 1062-1078
- 4 Deming WE. Out of the crisis. Cambridge, Massachusetts: The MIT Press; 2018. xv 430 pages
- 5 Leitlinien ADWMFAWMF–SK „AWMF-Regelwerk „Leitlinien““ .2012. 3.10.2019. http://www.awmf.org/leitlinien/awmf-regelwerk.html
- 6 Klimek L, Bergmann KC, Biedermann T. et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J Int 2017; 26: 16-24
- 7 Ruëff F, Bergmann KC, Brockow K. et al. Hauttests zur Diagnostik von allergischen Soforttypreaktionen. Allergo J. 2010; 19: 402-415
- 8 Bousquet J, Heinzerling L, Bachert C. et al. Practical guide to skin prick tests in allergy to aeroallergens. Allergy 2012; 67: 18-24
- 9 McCann WA, Ownby DR. The reproducibility of the allergy skin test scoring and interpretation by board-certified/board-eligible allergists. Ann Allergy Asthma Immunol 2002; 89: 368-371
- 10 Mahler V. Testallergene: Aktueller Stand der Verfügbarkeit aus regulatorischer Sicht. Allergologie 2019; 42: 309-313
- 11 Mahler V, Becker D, Brasch J et al. AWMF-S3-Leitlinie. Durchführung des Epikutantests mit Kontaktallergenen und Arzneimitteln. 2019;AWMF-Register-Nr.: 013-018 2019;
- 12 Bundesrat Allgemeine Verwaltungsvorschrift zur Änderung der Allgemeinen Verwaltungsvorschrift zum Verfahren der behördlichen Überwachung der Einhaltung der Grundsätze der Guten Laborpraxis. 2011
- 13 Renz H, Biedermann T, Bufe A. et al. In-vitro-Allergiediagnostik. Allergo J 2010; 19: 110-128
- 14 Kleine-Tebbe J, Reese I, Ballmer-Weber B. et al. Keine Empfehlung für IgG-und IgG4-Bestimmungen gegen Nahrungsmittel. Allergo J 2009; 18: 267-273
- 15 Haftenberger M, Laußmann D, Ellert U. et al. Prevalence of sensitisation to aeraoallergens and food allergens: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2013; 56: 687-697
- 16 Burbach GJ, Heinzerling LM, Edenharter G. et al. GA(2)LEN skin test study II: clinical relevance of inhalant allergen sensitizations in Europe. Allergy 2009; 64: 1507-1515
- 17 Worm M, Reese I, Ballmer-Weber B. et al. Guidelines on the management of IgE-mediated food allergies: S2k-Guidelines of the German Society for Allergology and Clinical Immunology (DGAKI) in collaboration with the German Medical Association of Allergologists (AeDA), the German Professional Association of Pediatricians (BVKJ), the German Allergy and Asthma Association (DAAB), German Dermatological Society (DDG), the German Society for Nutrition (DGE), the German Society for Gastroenterology, Digestive and Metabolic Diseases (DGVS), the German Society for Oto-Rhino-Laryngology, Head and Neck Surgery, the German Society for Pediatric and Adolescent Medicine (DGKJ), the German Society for Pediatric Allergology and Environmental Medicine (GPA), the German Society for Pneumology (DGP), the German Society for Pediatric Gastroenterology and Nutrition (GPGE), German Contact Allergy Group (DKG), the Austrian Society for Allergology and Immunology (Æ-GAI), German Professional Association of Nutritional Sciences (VDOE) and the Association of the Scientific Medical Societies Germany (AWMF). Allergo J Int 2015; 24: 256-293
- 18 Brockow K, Przybilla B, Aberer W. et al. Guideline for the diagnosis of drug hypersensitivity reactions: S2K-Guideline of the German Society for Allergology and Clinical Immunology (DGAKI) and the German Dermatological Society (DDG) in collaboration with the Association of German Allergologists (AeDA), the German Society for Pediatric Allergology and Environmental Medicine (GPA), the German Contact Dermatitis Research Group (DKG), the Swiss Society for Allergy and Immunology (SGAI), the Austrian Society for Allergology and Immunology (ÖGAI), the German Academy of Allergology and Environmental Medicine (DAAU), the German Center for Documentation of Severe Skin Reactions and the German Federal Institute for Drugs and Medical Products (BfArM). Allergo Journal International 2015; 24: 94-105
- 19 Przybilla B, Ruëff F, Walker A. et al. Diagnose und Therapie der Bienen-und Wespengiftallergie. Allergo Journal 2011; 20: 318-339
- 20 Werfel T, Heratizadeh A, Aberer W. et al. S2k guideline on diagnosis and treatment of atopic dermatitis – short version. Allergo J Int 2016; 25: 82-95
- 21 Augé J, Vent J, Agache I. et al. EAACI Position paper on the standardization of nasal allergen challenges. Allergy 2018; 73: 1597-1608
- 22 Kowalski ML, Agache I, Bavbek S. et al. Diagnosis and management of NSAID-Exacerbated Respiratory Disease (N-ERD) – a EAACI position paper. Allergy 2019; 74: 28-39
- 23 Barry MJ, Edgman-Levitan S. Shared decision making – pinnacle of patient-centered care. N Engl J Med 2012; 366: 780-781
- 24 Bousquet J, Hellings PW, Agache I. et al. Allergic Rhinitis and its Impact on Asthma (ARIA) Phase 4 (2018): Change management in allergic rhinitis and asthma multimorbidity using mobile technology. J Allergy Clin Immunol. 2019. 143 864-879
- 25 Loerbroks A, Tolksdorf SJ, Wagenmann M, Smith H. Food allergy knowledge, attitudes and their determinants among restaurant staff: A cross-sectional study. PLoS One 2019; 14: e0214625
- 26 Promoting effective self-management programmes to improve COPD. [editorial]. Eur Respir J 2009; 33: 461
- 27 Dinneen SF. Structured education for people with type 2 diabetes. BMJ 2008; 336: 459-460
- 28 Chowdhury NI, Mace JC, Bodner TE. et al. Does Medical Therapy Improve SinoNasal Outcomes Test-22 Domain Scores? An Analysis of Clinically Important Differences. Laryngoscope 2019; 129: 31-36
- 29 Biermann J, Merk HF, Wehrmann W, Klimek L, Wasem J. Allergic disorders of the respiratory tract – findings from a large patient sample in the German statutory health insurance system. Allergo Journal 2013; 22: 366-373
- 30 Seyfert-Margolis V. The evidence gap. Nat Biotechnol 2018; 36: 228-232
- 31 Valovirta E, Petersen TH, Piotrowska T. et al. Results from the 5-year SQ grass sublingual immunotherapy tablet asthma prevention (GAP) trial in children with grass pollen allergy. J Allergy Clin Immunol 2018; 141: 529-538.e13
- 32 Wahn U, Bachert C, Heinrich J, Richter H, Zielen S. Real-world benefits of allergen immunotherapy for birch pollen-associated allergic rhinitis and asthma. Allergy 2019; 74: 594-604
- 33 Kristiansen M, Dhami S, Netuveli G. et al. Allergen immunotherapy for the prevention of allergy: A systematic review and meta-analysis. Pediatr Allergy Immunol 2017; 28: 18-29
- 34 Purello-D’Ambrosio F, Gangemi S, Merendino RA. et al. Prevention of new sensitizations in monosensitized subjects submitted to specific immunotherapy or not. A retrospective study. Clin Exp Allergy 2001; 31: 1295-1302
- 35 Pfaar O, Bachert C, Bufe A. et al. Leitlinie zur (allergen-) spezifischen Immuntherapie bei IgE-vermittelten allergischen Erkrankungen. Allergo J Int 2014; 23: 282-319
- 36 Brehler R, Klimek L, Vogelberg C, Werfel T, Pfaar O, Hamelmann E. Evidenz vs . Wirksamkeit am Beispiel von in Deutschland verkehrsfähigen Präparaten zur (allergen-) spezifischen Immuntherapie. Allergo J Int 2016; 38-43
- 37 Klimek L, Hamelmann E, Werfel T. Therapieallergene-Verordnung (TAV) und allergenspezifische Immuntherapie: Was darf man überhaupt noch verordnen?. Allergologie 2018; 41: 15-18
- 38 Bachert C, Horn A, Wagenmann M, Brehmer D, Wahn U, Leserbrief zum Beitrag L, Klimek E. Hamelmann und T Werfel: Therapieallergene-Verordnung (TAV) und allergenspezifische Immuntherapie: Was darf man überhauptnoch verordnen?. Allergologie 2018; 41: 231-233
- 39 Klimek L, Werfel T, Vogelberg C. et al. Versuchte Verordnungssteuerung durch Fehlinterpretation. Allergo J 2018; 27: 78-80
- 40 Bundesrat Therapieallergene Verordnung. 2008; 1
- 41 Wollenberg A, Barbarot S, Bieber T. et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. [letter]. J Eur Acad Dermatol Venereol 2018; 32: 850-878
- 42 Schulz M, Martin E, Dalhoff K. et al. Nationale VersorgungsLeitlinie Asthma. www.asthmaversorgungsleitliniende 20181-106
- 43 Buhl R, Bals R, Baur X et al. S2k-Leitlinie zur Diagnostik und Therapie von Patienten mit Asthma. AWMF-Registernummer 020-009 httpswwwawmforgleitliniendetailll-html 2017
- 44 Zuberbier T, Aberer W, Asero R. et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018; 73: 1393-1414
- 45 Chaker AM. Biologics in Rhinology – Forthcoming Personalized Concepts: the Future Starts Today. Laryngorhinootologie 2018; 97: S142-S184
- 46 Palomares O, Untersmayr E, Gutermuth J et al. Biologicals in allergic diseases and asthma: Towards personalized medicine and precision health: Highlights of the 3rd EAACI Master Class on Biologicals, San Lorenzo de El Escorial, Madrid, 2019. Allergy 2019
- 47 Han Y, Chen Y, Liu X. et al. Efficacy and safety of dupilumab for the treatment of adult atopic dermatitis: A meta-analysis of randomized clinical trials.[letter]. J Allergy Clin Immunol 2017; 140: 888-891.e6
- 48 Bousquet J, Lund VJ, van Cauwenberge P. et al. Implementation of guidelines for seasonal allergic rhinitis: a randomized controlled trial. Allergy 2003; 58: 733-741
- 49 Sleurs K, Seys S, Bousquet J et al. Mobile health tools for the management of chronic respiratory diseases. Allergy 2019
- 50 Pugin B, Deneyer L, Bachert C. et al. Patient Advisory Board for Chronic Rhinosinusitis - A EUFOREA initiative. Rhinology 2019; 57: 331-335
- 51 “Netzwerk allergologischer Referenzzentren”. Berlin, 2014. 5.10.2019 2019. <https://dgaki.de/cac/>
- 52 “CAC-Zertifizierungsprozess.” Berlin, 2014. 5.10.2019 2019. <https://dgaki.de/cac/checklisten/>
- 53 Bundesärztekammer. (Muster-)Weiterbildungsordnung. Berlin: Bundesärztekammer; 2018: 1
- 54 Bundesärztekammer. Gebiet Hals-Nasen-Ohrenheilkunde. Facharzt/Fachärztin für Hals-Nasen-Ohrenheilkunde. In Ärztekammern ADD. editor (Muster-) Weiterbildungsordnung; 2018. p 92-97
- 55 Arbeitsgemeinschaft Klinische Immunologie AUU, DGHNO-KHC. “Richtlinien des Grund- und Aufbaukurses „Allergologie. in der HNO-Heilkunde“.” Ed DGHNO-KHC. 1.10.2019 2019. <https://allergologie.hno.org/storage/app/media/PDF/RichtlinienAllergiekurse.pdf>
- 56 Bundesärztekammer. Zusatz-Weiterbildung Allergologie. In Ärztekammern ADD. editor (Muster-)Weiterbildungsordnung; 2018. p 299-301
- 57 Worm M, Francuzik W, Renaudin JM. et al. Factors increasing the risk for a severe reaction in anaphylaxis: An analysis of data from The European Anaphylaxis Registry. Allergy 2018; 73: 1322-1330
- 58 editor 121. Deutscher Ärztetag. Beschlussprotokoll. 2018 Berlin: Bundesärztekammer (Arbeitsgemeinschaft der deutschen Ärztekammern); 2018
- 59 Werfel T. Allergologen-Ausbildung auf dem Holzweg. Allergo J 2018; 27: 64
- 60 Gerth van Wijk R. Stellungnahme der UEMS zur neuen Musterweiterbildungsordnung Allergologie (an die DGAKI). Allergo J 2018; 27: 65
- 61 Gerth van Wijk R, Eguiluz-Gracia I, Gayraud J. et al. The roadmap for allergology in Europe: The subspecialty of allergology as “stop-over” on the way to a full specialty. An EAACI position statement. Allergy 2018; 73: 540-548
- 62 Malling HJ, Gayraud J, Papageorgiu-Saxoni P, Hornung B, Rosado-Pinto J, Del Giacco SG. Objectives of training and specialty training core curriculum in allergology and clinical immunology. Allergy 2004; 59: 579-588
- 63 Fyhrquist N, Werfel T, Bilò MB, Mülleneisen N, Gerth van Wijk R. The roadmap for the Allergology specialty and allergy care in Europe and adjacent countries. An EAACI position paper. Clin Transl Allergy 2019; 9: 3
- 64 Panesar SS, Javad S, de Silva D. et al. The epidemiology of anaphylaxis in Europe: a systematic review. Allergy 2013; 68: 1353-1361
- 65 Langen U, Schmitz R, Steppuhn H. Prevalence of allergic diseases in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2013; 56: 698-706
Korrespondenzadresse
-
Literatur
- 1 Bergmann KC, Heinrich J, Niemann H. Current status of allergy prevalence in Germany: Position paper of the Environmental Medicine Commission of the Robert Koch Institute. Allergo J Int 2016; 25: 6-10
- 2 Cingi C, Gevaert P, Mösges R. et al. Multi-morbidities of allergic rhinitis in adults: European Academy of Allergy and Clinical Immunology Task Force Report. Clin Transl Allergy 2017; 7: 17
- 3 Bousquet J, Anto JM, Wickman M. et al. Are allergic multimorbidities and IgE polysensitization associated with the persistence or re-occurrence of foetal type 2 signalling? The MeDALL hypothesis. Allergy 2015; 70: 1062-1078
- 4 Deming WE. Out of the crisis. Cambridge, Massachusetts: The MIT Press; 2018. xv 430 pages
- 5 Leitlinien ADWMFAWMF–SK „AWMF-Regelwerk „Leitlinien““ .2012. 3.10.2019. http://www.awmf.org/leitlinien/awmf-regelwerk.html
- 6 Klimek L, Bergmann KC, Biedermann T. et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J Int 2017; 26: 16-24
- 7 Ruëff F, Bergmann KC, Brockow K. et al. Hauttests zur Diagnostik von allergischen Soforttypreaktionen. Allergo J. 2010; 19: 402-415
- 8 Bousquet J, Heinzerling L, Bachert C. et al. Practical guide to skin prick tests in allergy to aeroallergens. Allergy 2012; 67: 18-24
- 9 McCann WA, Ownby DR. The reproducibility of the allergy skin test scoring and interpretation by board-certified/board-eligible allergists. Ann Allergy Asthma Immunol 2002; 89: 368-371
- 10 Mahler V. Testallergene: Aktueller Stand der Verfügbarkeit aus regulatorischer Sicht. Allergologie 2019; 42: 309-313
- 11 Mahler V, Becker D, Brasch J et al. AWMF-S3-Leitlinie. Durchführung des Epikutantests mit Kontaktallergenen und Arzneimitteln. 2019;AWMF-Register-Nr.: 013-018 2019;
- 12 Bundesrat Allgemeine Verwaltungsvorschrift zur Änderung der Allgemeinen Verwaltungsvorschrift zum Verfahren der behördlichen Überwachung der Einhaltung der Grundsätze der Guten Laborpraxis. 2011
- 13 Renz H, Biedermann T, Bufe A. et al. In-vitro-Allergiediagnostik. Allergo J 2010; 19: 110-128
- 14 Kleine-Tebbe J, Reese I, Ballmer-Weber B. et al. Keine Empfehlung für IgG-und IgG4-Bestimmungen gegen Nahrungsmittel. Allergo J 2009; 18: 267-273
- 15 Haftenberger M, Laußmann D, Ellert U. et al. Prevalence of sensitisation to aeraoallergens and food allergens: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2013; 56: 687-697
- 16 Burbach GJ, Heinzerling LM, Edenharter G. et al. GA(2)LEN skin test study II: clinical relevance of inhalant allergen sensitizations in Europe. Allergy 2009; 64: 1507-1515
- 17 Worm M, Reese I, Ballmer-Weber B. et al. Guidelines on the management of IgE-mediated food allergies: S2k-Guidelines of the German Society for Allergology and Clinical Immunology (DGAKI) in collaboration with the German Medical Association of Allergologists (AeDA), the German Professional Association of Pediatricians (BVKJ), the German Allergy and Asthma Association (DAAB), German Dermatological Society (DDG), the German Society for Nutrition (DGE), the German Society for Gastroenterology, Digestive and Metabolic Diseases (DGVS), the German Society for Oto-Rhino-Laryngology, Head and Neck Surgery, the German Society for Pediatric and Adolescent Medicine (DGKJ), the German Society for Pediatric Allergology and Environmental Medicine (GPA), the German Society for Pneumology (DGP), the German Society for Pediatric Gastroenterology and Nutrition (GPGE), German Contact Allergy Group (DKG), the Austrian Society for Allergology and Immunology (Æ-GAI), German Professional Association of Nutritional Sciences (VDOE) and the Association of the Scientific Medical Societies Germany (AWMF). Allergo J Int 2015; 24: 256-293
- 18 Brockow K, Przybilla B, Aberer W. et al. Guideline for the diagnosis of drug hypersensitivity reactions: S2K-Guideline of the German Society for Allergology and Clinical Immunology (DGAKI) and the German Dermatological Society (DDG) in collaboration with the Association of German Allergologists (AeDA), the German Society for Pediatric Allergology and Environmental Medicine (GPA), the German Contact Dermatitis Research Group (DKG), the Swiss Society for Allergy and Immunology (SGAI), the Austrian Society for Allergology and Immunology (ÖGAI), the German Academy of Allergology and Environmental Medicine (DAAU), the German Center for Documentation of Severe Skin Reactions and the German Federal Institute for Drugs and Medical Products (BfArM). Allergo Journal International 2015; 24: 94-105
- 19 Przybilla B, Ruëff F, Walker A. et al. Diagnose und Therapie der Bienen-und Wespengiftallergie. Allergo Journal 2011; 20: 318-339
- 20 Werfel T, Heratizadeh A, Aberer W. et al. S2k guideline on diagnosis and treatment of atopic dermatitis – short version. Allergo J Int 2016; 25: 82-95
- 21 Augé J, Vent J, Agache I. et al. EAACI Position paper on the standardization of nasal allergen challenges. Allergy 2018; 73: 1597-1608
- 22 Kowalski ML, Agache I, Bavbek S. et al. Diagnosis and management of NSAID-Exacerbated Respiratory Disease (N-ERD) – a EAACI position paper. Allergy 2019; 74: 28-39
- 23 Barry MJ, Edgman-Levitan S. Shared decision making – pinnacle of patient-centered care. N Engl J Med 2012; 366: 780-781
- 24 Bousquet J, Hellings PW, Agache I. et al. Allergic Rhinitis and its Impact on Asthma (ARIA) Phase 4 (2018): Change management in allergic rhinitis and asthma multimorbidity using mobile technology. J Allergy Clin Immunol. 2019. 143 864-879
- 25 Loerbroks A, Tolksdorf SJ, Wagenmann M, Smith H. Food allergy knowledge, attitudes and their determinants among restaurant staff: A cross-sectional study. PLoS One 2019; 14: e0214625
- 26 Promoting effective self-management programmes to improve COPD. [editorial]. Eur Respir J 2009; 33: 461
- 27 Dinneen SF. Structured education for people with type 2 diabetes. BMJ 2008; 336: 459-460
- 28 Chowdhury NI, Mace JC, Bodner TE. et al. Does Medical Therapy Improve SinoNasal Outcomes Test-22 Domain Scores? An Analysis of Clinically Important Differences. Laryngoscope 2019; 129: 31-36
- 29 Biermann J, Merk HF, Wehrmann W, Klimek L, Wasem J. Allergic disorders of the respiratory tract – findings from a large patient sample in the German statutory health insurance system. Allergo Journal 2013; 22: 366-373
- 30 Seyfert-Margolis V. The evidence gap. Nat Biotechnol 2018; 36: 228-232
- 31 Valovirta E, Petersen TH, Piotrowska T. et al. Results from the 5-year SQ grass sublingual immunotherapy tablet asthma prevention (GAP) trial in children with grass pollen allergy. J Allergy Clin Immunol 2018; 141: 529-538.e13
- 32 Wahn U, Bachert C, Heinrich J, Richter H, Zielen S. Real-world benefits of allergen immunotherapy for birch pollen-associated allergic rhinitis and asthma. Allergy 2019; 74: 594-604
- 33 Kristiansen M, Dhami S, Netuveli G. et al. Allergen immunotherapy for the prevention of allergy: A systematic review and meta-analysis. Pediatr Allergy Immunol 2017; 28: 18-29
- 34 Purello-D’Ambrosio F, Gangemi S, Merendino RA. et al. Prevention of new sensitizations in monosensitized subjects submitted to specific immunotherapy or not. A retrospective study. Clin Exp Allergy 2001; 31: 1295-1302
- 35 Pfaar O, Bachert C, Bufe A. et al. Leitlinie zur (allergen-) spezifischen Immuntherapie bei IgE-vermittelten allergischen Erkrankungen. Allergo J Int 2014; 23: 282-319
- 36 Brehler R, Klimek L, Vogelberg C, Werfel T, Pfaar O, Hamelmann E. Evidenz vs . Wirksamkeit am Beispiel von in Deutschland verkehrsfähigen Präparaten zur (allergen-) spezifischen Immuntherapie. Allergo J Int 2016; 38-43
- 37 Klimek L, Hamelmann E, Werfel T. Therapieallergene-Verordnung (TAV) und allergenspezifische Immuntherapie: Was darf man überhaupt noch verordnen?. Allergologie 2018; 41: 15-18
- 38 Bachert C, Horn A, Wagenmann M, Brehmer D, Wahn U, Leserbrief zum Beitrag L, Klimek E. Hamelmann und T Werfel: Therapieallergene-Verordnung (TAV) und allergenspezifische Immuntherapie: Was darf man überhauptnoch verordnen?. Allergologie 2018; 41: 231-233
- 39 Klimek L, Werfel T, Vogelberg C. et al. Versuchte Verordnungssteuerung durch Fehlinterpretation. Allergo J 2018; 27: 78-80
- 40 Bundesrat Therapieallergene Verordnung. 2008; 1
- 41 Wollenberg A, Barbarot S, Bieber T. et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. [letter]. J Eur Acad Dermatol Venereol 2018; 32: 850-878
- 42 Schulz M, Martin E, Dalhoff K. et al. Nationale VersorgungsLeitlinie Asthma. www.asthmaversorgungsleitliniende 20181-106
- 43 Buhl R, Bals R, Baur X et al. S2k-Leitlinie zur Diagnostik und Therapie von Patienten mit Asthma. AWMF-Registernummer 020-009 httpswwwawmforgleitliniendetailll-html 2017
- 44 Zuberbier T, Aberer W, Asero R. et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018; 73: 1393-1414
- 45 Chaker AM. Biologics in Rhinology – Forthcoming Personalized Concepts: the Future Starts Today. Laryngorhinootologie 2018; 97: S142-S184
- 46 Palomares O, Untersmayr E, Gutermuth J et al. Biologicals in allergic diseases and asthma: Towards personalized medicine and precision health: Highlights of the 3rd EAACI Master Class on Biologicals, San Lorenzo de El Escorial, Madrid, 2019. Allergy 2019
- 47 Han Y, Chen Y, Liu X. et al. Efficacy and safety of dupilumab for the treatment of adult atopic dermatitis: A meta-analysis of randomized clinical trials.[letter]. J Allergy Clin Immunol 2017; 140: 888-891.e6
- 48 Bousquet J, Lund VJ, van Cauwenberge P. et al. Implementation of guidelines for seasonal allergic rhinitis: a randomized controlled trial. Allergy 2003; 58: 733-741
- 49 Sleurs K, Seys S, Bousquet J et al. Mobile health tools for the management of chronic respiratory diseases. Allergy 2019
- 50 Pugin B, Deneyer L, Bachert C. et al. Patient Advisory Board for Chronic Rhinosinusitis - A EUFOREA initiative. Rhinology 2019; 57: 331-335
- 51 “Netzwerk allergologischer Referenzzentren”. Berlin, 2014. 5.10.2019 2019. <https://dgaki.de/cac/>
- 52 “CAC-Zertifizierungsprozess.” Berlin, 2014. 5.10.2019 2019. <https://dgaki.de/cac/checklisten/>
- 53 Bundesärztekammer. (Muster-)Weiterbildungsordnung. Berlin: Bundesärztekammer; 2018: 1
- 54 Bundesärztekammer. Gebiet Hals-Nasen-Ohrenheilkunde. Facharzt/Fachärztin für Hals-Nasen-Ohrenheilkunde. In Ärztekammern ADD. editor (Muster-) Weiterbildungsordnung; 2018. p 92-97
- 55 Arbeitsgemeinschaft Klinische Immunologie AUU, DGHNO-KHC. “Richtlinien des Grund- und Aufbaukurses „Allergologie. in der HNO-Heilkunde“.” Ed DGHNO-KHC. 1.10.2019 2019. <https://allergologie.hno.org/storage/app/media/PDF/RichtlinienAllergiekurse.pdf>
- 56 Bundesärztekammer. Zusatz-Weiterbildung Allergologie. In Ärztekammern ADD. editor (Muster-)Weiterbildungsordnung; 2018. p 299-301
- 57 Worm M, Francuzik W, Renaudin JM. et al. Factors increasing the risk for a severe reaction in anaphylaxis: An analysis of data from The European Anaphylaxis Registry. Allergy 2018; 73: 1322-1330
- 58 editor 121. Deutscher Ärztetag. Beschlussprotokoll. 2018 Berlin: Bundesärztekammer (Arbeitsgemeinschaft der deutschen Ärztekammern); 2018
- 59 Werfel T. Allergologen-Ausbildung auf dem Holzweg. Allergo J 2018; 27: 64
- 60 Gerth van Wijk R. Stellungnahme der UEMS zur neuen Musterweiterbildungsordnung Allergologie (an die DGAKI). Allergo J 2018; 27: 65
- 61 Gerth van Wijk R, Eguiluz-Gracia I, Gayraud J. et al. The roadmap for allergology in Europe: The subspecialty of allergology as “stop-over” on the way to a full specialty. An EAACI position statement. Allergy 2018; 73: 540-548
- 62 Malling HJ, Gayraud J, Papageorgiu-Saxoni P, Hornung B, Rosado-Pinto J, Del Giacco SG. Objectives of training and specialty training core curriculum in allergology and clinical immunology. Allergy 2004; 59: 579-588
- 63 Fyhrquist N, Werfel T, Bilò MB, Mülleneisen N, Gerth van Wijk R. The roadmap for the Allergology specialty and allergy care in Europe and adjacent countries. An EAACI position paper. Clin Transl Allergy 2019; 9: 3
- 64 Panesar SS, Javad S, de Silva D. et al. The epidemiology of anaphylaxis in Europe: a systematic review. Allergy 2013; 68: 1353-1361
- 65 Langen U, Schmitz R, Steppuhn H. Prevalence of allergic diseases in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2013; 56: 698-706