
RSS-Feed abonnieren
DOI: 10.1055/a-1287-6932
Anatomy of the great and small saphenous veins
Artikel in mehreren Sprachen: deutsch | English
- Abstract
- Introduction
- Course of the great saphenous vein
- Draining of the great saphenous vein
- The course of the small saphenous vein
- Saphenopopliteal junction
- Summary
- Literatur
Abstract
Varicose veins are by far the most frequent illness phlebologists deal with. Great and small saphenous vein are nearly always involved in the pathological recirculation. Their anatomy is constant, excepting for variation in their course and junctions. In times where we can apply patient tailored treatments, adapting different techniques and strategies to the findings, we can offer the least harming method after analyzing the anatomy of the patient and perhaps reduce recurrence rate. Today ultrasound is the gold standard to explore varicose veins. Thus, information about anatomy of superficial leg veins has to be implemented with the ultrasound anatomy of the situs. The present article describes the anatomy of the saphenous veins with schematic images and ultrasound examples of the typical findings.
#
Key words
great saphenous vein - small saphenous vein - saphenofemoral junction - saphenopopliteal junction - muscle veinsSchlüsselwörter
V. saphena magna - V. saphena parva - saphenofemoraler Übergang - saphenopoplitealer Übergang - Venenstern - MuskelvenenIntroduction
The term ‘saphenous’ was first coined by Avicenna, from the Arabic el safin, which means ‘concealed’ [1]. In each leg, the great saphenous vein (V. saphena magna) runs along the inner aspect of the leg, while the small saphenous vein (V. saphena parva) runs along the back of the calf. These two veins are the ones most frequently involved in pathological conditions of the superficial venous system requiring treatment. In the proximal thigh, there may be two accessory saphenous trunks – the anterior accessory saphenous vein (V. saphena accessoria anterior; see the article by Riabinska and Mendoza in this issue) and the posterior accessory saphenous vein (V. saphena accessoria posterior; see Valesky and Brenner in this issue).
From the various names used in the literature for the saphenous veins, the International Consensus on the Nomenclature of the Anatomy of the Leg Veins (UIP 2001, Rome, published in 2002 [2]), determined that ‘great saphenous vein (GSV)’ and ‘small saphenous vein (SSV)’ were used most often. The organisation of the veins into different anatomical compartments was also defined. The veins had formerly been divided into the ‘deep veins’ (running within the muscle fascia) and the ‘superficial veins’ (running outside the muscle fascia). The deep venous system remained the same in the new nomenclature, designated network 1 (N1). In accordance with the papers by Caggiati and Ricci [3] [4] [5], the superficial veins were divided into two anatomical compartments: the saphenous compartment (network 2; N2) containing the saphenous veins and the epifascial compartment with all the other superficial leg veins (network 3; N3).
The saphenous veins therefore run directly on the muscle fascia, separated from the subcutaneous fatty tissue by their own fascia, the saphenous fascia. A ligament (the saphenous ligament) fixes the saphenous vein to the muscle fascia and the saphenous fascia, which is why the saphenous veins almost never follow a winding course ([Fig. 1], [2]).


#
Course of the great saphenous vein
The great saphenous vein arises from the veins on the dorsum of the foot and can be seen on the inner aspect of the ankle anterior to the medial malleolus. It then runs proximally parallel to the tibial crest, turning slightly posterior just below the knee and continuing on the medial aspect of the thigh to the groin ([Fig. 1]). The great saphenous vein opens fairly consistently into the common femoral vein below the inguinal ligament. It receives various tributaries, forming the structure known in German as the ‘venous star’. Due to its aspect like a bishop’s hook, this region has been referred to as ‘the crosse’ but is now termed as the saphenofemoral junction (SFJ), which will be described in the next paragraph.
The great saphenous vein always runs in its fascial compartment. A doubled great saphenous vein is therefore only possible when there are indeed two parallel lumens in the compartment. This variant of normal occurs in only 1 % of cases [6]. They are then bound together with part of the saphenous ligament. The earlier high figure of a 27 % duplication of the great saphenous vein [7] is the sum of the true doubled vessels (1 %) and an extrafascial superficial accessory saphenous vein running parallel to the GSV in 26 % of cases [6].
Segmental aplasia of the great saphenous vein is present if no lumen can be demonstrated in the fascial compartment on ultrasound scanning or in the dissected specimen. On histology, there is always a cellular rudiment of the GSV without a lumen [8]. This variant is found in the thigh in 12 % of people with healthy veins and 25 % of patients with reflux [9]. Some authors also distinguish hypoplasia: in this case the great saphenous vein can still be demonstrated but the lumen is very small in diameter, measuring between 1 and 2 mm. An accessory superficial saphenous vein drains into the great saphenous vein distal and proximal to these aplastic or hypoplastic segments, allowing a continued flow by providing a bypass to the aplastic segment – the flow will be antegrade in a healthy vein or retrograde if there is valvular incompetence. This is not an extrafascial saphenous vein, but rather a superficial bypass.
Seidel analysed the possible types of aplastic segment and described six types ([Fig. 3a–g], [Table 1]) [10]. The author considers that there is yet another type, with aplasia of the GSV from distal to the terminal valve to the middle of the thigh, with a bypass via the anterior accessory saphenous vein; this variant is described in the article by Riabinska in this issue ([Fig. 3g]).
|
Aplasia type |
Number |
% of aplasias |
% overall |
|
I |
18 |
4.1 % |
0.7 % |
|
II |
61 |
13.8 % |
2.3 % |
|
III |
319 |
72.2 % |
12 % |
|
IV |
15 |
3.4 % |
0.6 % |
|
V |
28 |
6.3 % |
1.1 % |
|
VI |
1 |
0.2 % |
0.04 % |
|
Total |
442 |
100 % |
16.74 % |

On ultrasound scanning, the great saphenous vein has a relatively consistent diameter through the calf and thigh (with the exception of the groin). It is quite small in those with healthy veins, being less than 4 mm in the thigh [11]. In cross-section, the vein is round and embedded in the fascial compartment, sometimes also with a visible saphenous ligament ([Fig. 4a–c]). As tributaries of the main venous trunk drain from the saphenous compartment by running through the saphenous fascia to the skin, tributaries always run between the saphenous fascia and the skin ([Fig. 4d], [5b]). Perforating veins on the other hand penetrate the muscle fascia and run away from the skin surface ([Fig. 4e]).


In longitudinal section, the saphenous vein appears as a smooth tube with parallel walls ([Fig. 5a]). If a segment of the vein shows reflux and the reflux is transmitted back to the tributary, we see a sudden increase in size. The valves are often visible along the course of the vein and the vein walls widen at these points ([Fig. 5b]).
#
Draining of the great saphenous vein
The great saphenous vein drains into the common femoral vein at the level of the inguinal ligament. It typically has two valves in this region: the terminal valve and the preterminal valve (see [Fig. 6], [7]), although they are not present in every individual and often cannot be seen on ultrasound [12].
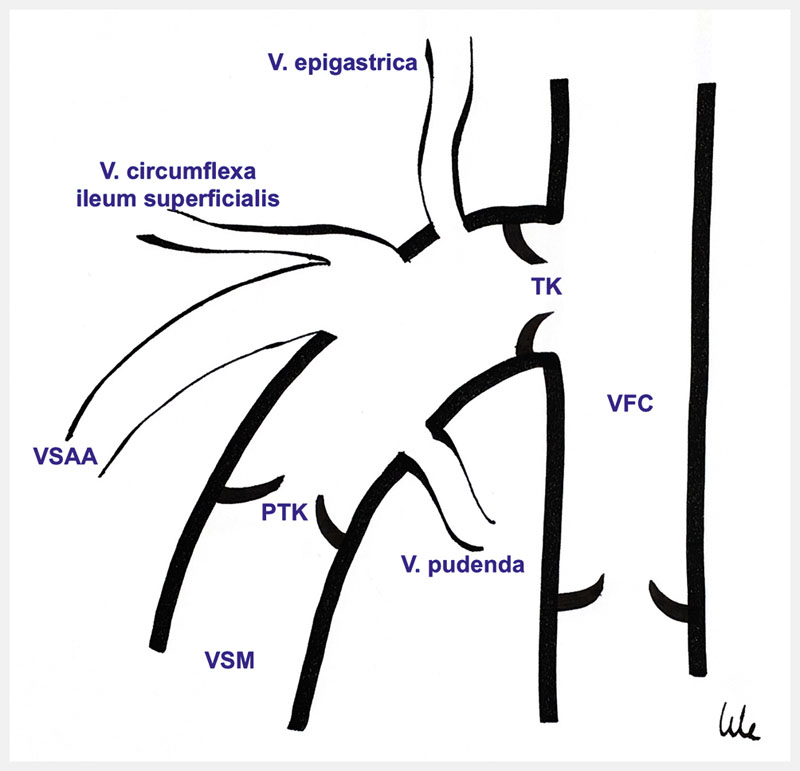
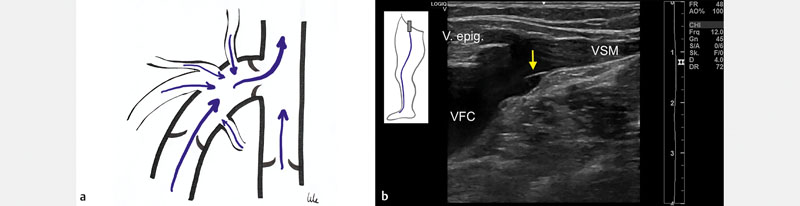
The great saphenous vein is often bent at the junction, giving rise to the earlier name of ‘crosse’ (from the French) for its resemblance to a bishop’s hook. The opening in the common femoral vein through which the blood flows from the great saphenous vein to the deep leg vein is called the ‘ostium’ and the whole region is known as the saphenofemoral junction. Here, the great saphenous vein receives various tributaries from all sides, giving rise to the name of “venous star” in German. These tributary veins may or may not all be present; they may open individually or collectively into the great saphenous vein, or even directly into the deep veins of the leg.
Tributaries that drain from above are the superficial circumflex iliac vein and the epigastric vein from above and lateral, and the pudendal veins from above and medial. The anterior accessory saphenous vein drains from below and lateral. It may open alone but often drains together with the epigastric vein into the great saphenous vein. Coming from below and medially, the posterior accessory saphenous vein rarely drains at the saphenofemoral junction but usually more distally ([Fig. 6]).
Depending on whether the valves in the SFJ are competent or not, there are various constellations of reflux. If all valves close, there is only an antegrade flow draining to the deep leg vein. Flow in the superior SFJ tributaries is directed towards the foot but usually does not last longer than 0.5 seconds after a Valsalva or other reflux provocation manoeuvre [13].
If the preterminal valve is competent but the terminal valve is not, there is a type 1 Stücker reflux [14] into the anterior accessory saphenous vein (see article by Riabinska in this issue). The great saphenous vein shows reflux only at the junction itself, as more distally the competent preterminal valve protects the vein from reflux ([Fig. 8]).

If the terminal valve is competent but the preterminal valve is not, we do not find any reflux into the trunk vein from the deep veins but there is reflux from the tributaries around the SFJ (type 2 Stücker reflux) [14], in various combinations: from only one superior vein ([Fig. 9a, b]), only the pudendal vein ([Fig. 9c]) or both ([Fig. 9d]). Such reflux is not rare, with a frequency of 21.3 % [15] (cf. table in the article by Riabinska in this issue).

In principle it is possible that the superior reflux fills not only the anterior accessory saphenous vein but also the great saphenous vein ([Fig. 10]); according to Zollmann, this occurs in 2 % of cases [15].

When both the terminal and preterminal valves are incompetent, there is an axial or type 3 Stücker reflux ([Fig. 11a]). The reflux across the terminal valve is measured directly at its opening ([Fig. 11b]).

In 7.6 % of cases [15], we find an axial reflux from the deep vein with simultaneous drainage via the great saphenous vein and the anterior accessory saphenous vein ([Fig. 12]).

In 1.1 %, we find simultaneous reflux from the common femoral vein and the superior veins into the anterior accessory saphenous vein with competent preterminal valves ([Fig. 13a]).

Type 4 reflux with both valves being competent but with reflux from an SFJ tributary into the anterior accessory saphenous vein was not defined in Stücker’s original publication on staging [14], although it is present in 3.7 % of cases according to Zollmann ([Fig. 13b]) [16].
#
The course of the small saphenous vein
The small saphenous vein (SSV) runs along the back of the calf from the lateral malleolus to the popliteal fossa, where it drains into the popliteal vein at various levels ([Fig. 14]).

In the calf, it is clearly contained in the fascial compartment above the muscle fascia and below the saphenous fascia ([Fig. 15]). Aplasia has not been described for the SSV, and segmental duplication in only 1 % of cases. Rarely, a small artery runs besides the SSV, and this must not be punctured during sclerotherapy. Duplex ultrasound scanning along the vein beforehand is therefore essential.

#
Saphenopopliteal junction
The junction of the SSV with the popliteal vein is usually at the level of the knee joint or up to 5 cm above it. It can, however, be much further proximal in the thigh or very rarely via a muscle vein distal to the popliteal fossa. In 60 % of cases there is a ‘thigh extension of the small saphenous vein’ which, depending on its course, is also referred to as the Giacomini vein (see article by Valesky and Brenner in this issue). The variants of the saphenopopliteal junction were summarised in the UIP anatomy consensus document as follows [17]:
-
Type A: The SSV clearly joins the deep vein (with or without the presence of a Giacomini vein
-
A1: The SSV joins the popliteal vein independently of the muscle veins ([Fig. 16a, b])
-
A2: The SSV receives muscle veins as tributaries before it joins the popliteal vein ([Fig. 16c, d]).
-
-
Type B: The SSV continues upwards as the thigh extension (Giacomini vein) and there is only a very thin vessel anastomosing with the deep system, which may almost be considered a perforating vein ([Fig. 17a]).
-
Type C: There is no connection between the SSV and the deep veins. No reflux is then found in the SSV ([Fig. 17b, c]).


The very variable anatomy of the SSV drainage, especially the fact that it sometimes receives muscle veins as tributaries at the junction, makes a preoperative duplex ultrasound examination of the area absolutely essential. It is relevant for planning the type of procedure and the level of intervention: if the vein drains at a very high level, it usually cannot be reached surgically, at least not without a very large incision. In the case of tributary muscle veins, the SSV must be separated from them distally in order to prevent very painful muscle vein thrombosis.
#
Summary
The great saphenous vein and less often the small saphenous vein are most frequently involved in the recirculation with varicose veins. Knowledge of their anatomy and the possible variations of normal is fundamental for diagnosis and planning treatment. As ultrasonography is the gold standard in the investigation of the leg veins today, an understanding of the venous anatomy as seen on ultrasound scans is always necessary.
#
#
-
Literatur
- 1 Caggiati A, Bergan J. The saphenous vein: Derivation of ist name and ist relevant anatomy. J Vasc Surg 2002; 35: 172-175
- 2 Caggiati A, Bergan JJ, Gloviczki P. et al. International Interdisciplinary Consensus Committee on Venous Anatomical Terminology. Nomenclature of the veins of the lower limbs: an international interdisciplinary consensus statement. J Vasc Surg 2002; 36: 416-422
- 3 Caggiati A, Ricci S. The long saphenous vein compartment. Phlebology 1999; 12: 107-111
- 4 Caggiati A. Fascial relations and structure of the tributaries of the saphenous veins. Surg Radiol Anat 2000; 22: 1-4
- 5 Caggiati A. Fascial relationships of the short saphenous vein. J Vasc Surg 2001; 34: 241-246
- 6 Ricci S, Caggiati A. Does a Double Long Saphenous Vein Exist?. Phlebology 1999; 14: 59-64
- 7 Kubik S. Anatomie der Beinvenen. In: Wuppermann T. (Hrsg) Varizen, Ulcus cruris und Thrombose. Berlin Heidelberg: Springer Verlag; 1986: 1-54
- 8 Kokova J, Horakova M, Horakova MA. The development of pre- and post-natal veins. Phlebologie 1993; 46: 241-251
- 9 Caggiati A, Mendoza E. Segmental Hypoplasia of the Great Saphenous Vein and Varicose Disease. Eur J Vasc Endovasc Surg 2004; 28: 257-261
- 10 Seidel AC, Cavalari PJr, Rossi RM. et al. Proposal for Classification of the Sapnehous Vein Aplasia by the B-Mode Ultra- sound. Ann Vasc Surg 2016; 31: 170-178
- 11 Mendoza E, Blättler W, Amsler F. Great Saphenous Vein Diameter at the Saphenofemoral Junction and Proximal Thigh as Parameters of Venous Disease Class. European Journal of Vascular and Endovascular Surgery 2013; 45 (01) 76-83
- 12 Mühlberger D, Morandini L, Brenner E. Venous valves and major superficial tributary veins near the saphenofemoral junction. J Vasc Surg 2009; 49: 1562-1569
- 13 Mendoza E. V. saphena magna. In: Mendoza E. (Hrsg) Duplexsonographie der oberflächlihcen Beinvenen. 3. Auflage. Springer Verlag; 2020: 133-186 https://doi.org/10.1007/978-3-662-58982-3_7
- 14 Stücker M, Moritz R, Altmeyer P. et al. New concept: different types of insufficiency of the saphenofemoral junction identified by duplex as a chance for a more differentiated therapy of the great saphenous vein. Phlebology 2013; 28: 268-274
- 15 Zollmann P, Zollmann C, Zollmann P. et al. Determining the origin of superficial venous reflux in the groin with duplex ultrasound and implications for varicose vein surgery. JVS V&L 2017; 5 (01) 82-86
- 16 Mendoza E, Stücker M. Duplex-ultrasound assessment of the saphenofemoral junction (Review). Phlebological Review 2015; 23 (03) 1-8
- 17 Cavezzi A, Labropoulos N, Partsch H. et al. Duplex Ultrasound Investigation of the Veins in Chronic Venous Disease of the Lower Limbs – UIP Consensus Document. Part II. Anatomy Eur J Vasc Endovasc Surg 2006; 31: 288-299
Korrespondenzadresse
Publikationsverlauf
Artikel online veröffentlicht:
17. Februar 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
Literatur
- 1 Caggiati A, Bergan J. The saphenous vein: Derivation of ist name and ist relevant anatomy. J Vasc Surg 2002; 35: 172-175
- 2 Caggiati A, Bergan JJ, Gloviczki P. et al. International Interdisciplinary Consensus Committee on Venous Anatomical Terminology. Nomenclature of the veins of the lower limbs: an international interdisciplinary consensus statement. J Vasc Surg 2002; 36: 416-422
- 3 Caggiati A, Ricci S. The long saphenous vein compartment. Phlebology 1999; 12: 107-111
- 4 Caggiati A. Fascial relations and structure of the tributaries of the saphenous veins. Surg Radiol Anat 2000; 22: 1-4
- 5 Caggiati A. Fascial relationships of the short saphenous vein. J Vasc Surg 2001; 34: 241-246
- 6 Ricci S, Caggiati A. Does a Double Long Saphenous Vein Exist?. Phlebology 1999; 14: 59-64
- 7 Kubik S. Anatomie der Beinvenen. In: Wuppermann T. (Hrsg) Varizen, Ulcus cruris und Thrombose. Berlin Heidelberg: Springer Verlag; 1986: 1-54
- 8 Kokova J, Horakova M, Horakova MA. The development of pre- and post-natal veins. Phlebologie 1993; 46: 241-251
- 9 Caggiati A, Mendoza E. Segmental Hypoplasia of the Great Saphenous Vein and Varicose Disease. Eur J Vasc Endovasc Surg 2004; 28: 257-261
- 10 Seidel AC, Cavalari PJr, Rossi RM. et al. Proposal for Classification of the Sapnehous Vein Aplasia by the B-Mode Ultra- sound. Ann Vasc Surg 2016; 31: 170-178
- 11 Mendoza E, Blättler W, Amsler F. Great Saphenous Vein Diameter at the Saphenofemoral Junction and Proximal Thigh as Parameters of Venous Disease Class. European Journal of Vascular and Endovascular Surgery 2013; 45 (01) 76-83
- 12 Mühlberger D, Morandini L, Brenner E. Venous valves and major superficial tributary veins near the saphenofemoral junction. J Vasc Surg 2009; 49: 1562-1569
- 13 Mendoza E. V. saphena magna. In: Mendoza E. (Hrsg) Duplexsonographie der oberflächlihcen Beinvenen. 3. Auflage. Springer Verlag; 2020: 133-186 https://doi.org/10.1007/978-3-662-58982-3_7
- 14 Stücker M, Moritz R, Altmeyer P. et al. New concept: different types of insufficiency of the saphenofemoral junction identified by duplex as a chance for a more differentiated therapy of the great saphenous vein. Phlebology 2013; 28: 268-274
- 15 Zollmann P, Zollmann C, Zollmann P. et al. Determining the origin of superficial venous reflux in the groin with duplex ultrasound and implications for varicose vein surgery. JVS V&L 2017; 5 (01) 82-86
- 16 Mendoza E, Stücker M. Duplex-ultrasound assessment of the saphenofemoral junction (Review). Phlebological Review 2015; 23 (03) 1-8
- 17 Cavezzi A, Labropoulos N, Partsch H. et al. Duplex Ultrasound Investigation of the Veins in Chronic Venous Disease of the Lower Limbs – UIP Consensus Document. Part II. Anatomy Eur J Vasc Endovasc Surg 2006; 31: 288-299
















