

Subscribe to RSS
DOI: 10.1055/a-1314-9818
Pancreatic perforation and fistula caused by pancreatic spontaneous dislodgement stent: an endoscopic rescue technique
Authors

Pancreatic stenting is widely used to prevent pancreatitis occurring after endoscopic retrograde cholangiopancreatography (ERCP) [1]. In general, a pancreatic spontaneous dislodgement stent (PSDS) with a duodenal pigtail prevents intraductal migration. Serious adverse events after PSDS placement, such as migration into the portal vein, have been reported [2]. Here, we present a case of pancreatic perforation and fistula caused by a dislocated and migrated PSDS and the technique by which rescue was achieved.
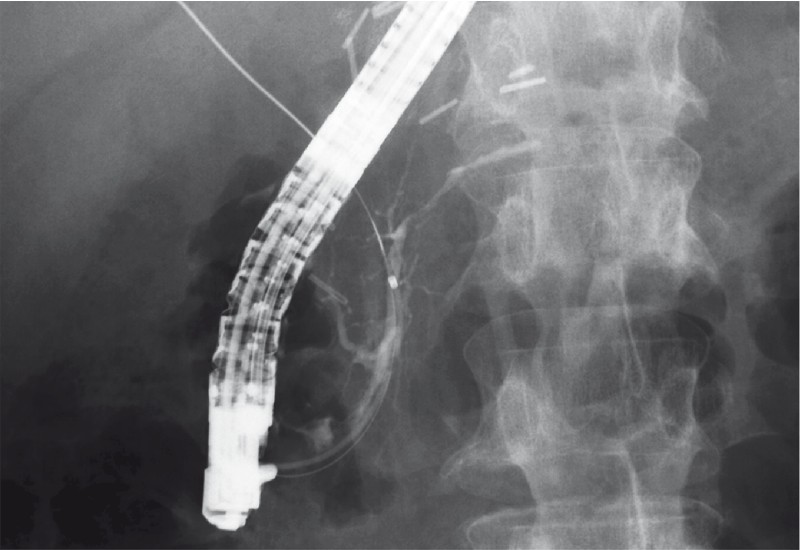
A 58-year-old man with biliary stones after Billroth-I reconstruction for gastric cancer was referred. We performed endoscopic stone extraction; however, selective biliary cannulation was difficult. A 7-Fr biliary stent and 5-Fr PSDS (Advanix pancreatic stent, single pigtail on the duodenal side, unflanged, 5 cm; Boston Scientific Japan, Tokyo, Japan) were placed following transpancreatic sphincterotomy in the first session ([Fig. 1]; [Video 1]). Two days later, the patient suddenly complained of severe exacerbation of abdominal pain and fever. Computed tomography showed pancreatic perforation and fistula caused by PSDS ([Fig. 2]). A second ERCP was performed, and the PSDS was removed using alligator forceps. Endoscopic retrograde pancreatography (ERP) confirmed the perforation and fistula, and endoscopic nasopancreatic drainage was placed across the perforated site ([Fig. 3]; [Video 1]). The symptoms immediately improved. Three days later, a third ERCP was performed with successful biliary stone extraction. However, ERP still showed perforation and fistula, and a 7-Fr pancreatic stent (Flexima, straight, double-flanged, 7-cm; Boston Scientific) was placed ([Fig. 4]; [Video 1]). Two days later, abdominal ultrasound revealed a portal vein thrombus (PVT), and direct oral anticoagulants were administered. One month later the PVT had resolved completely, and after 3 months the perforation and fistula were completely healed ([Fig. 5]; [Video 1]).

Video 1 Endoscopic rescue technique for management of pancreatic perforation and fistula caused by placement of a pancreatic spontaneous dislodgement stent.



When a prophylactic PSDS is placed, the possibility of adverse effects caused by dislocation and inward migration should be taken into account. Although challenging, if perforation and fistula are diagnosed, endoscopists should consider not only stent removal [2] but also immediate pancreatic drainage across the perforated site as a rescue treatment.
Endoscopy_UCTN_Code_CPL_1AK_2AC
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Dumonceau JM, Kapral C, Aabakken L. et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020; 52: 127-149
- 2 Leung WD, Parashette KR, Molleston JP. et al. Pancreatic stent migration into the portal vein causing portal vein thrombosis: a rare complication of a prophylactic pancreatic stent. Pancreatology 2012; 12: 463-465
Corresponding author
Publication History
Article published online:
17 December 2020
© 2020. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Dumonceau JM, Kapral C, Aabakken L. et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020; 52: 127-149
- 2 Leung WD, Parashette KR, Molleston JP. et al. Pancreatic stent migration into the portal vein causing portal vein thrombosis: a rare complication of a prophylactic pancreatic stent. Pancreatology 2012; 12: 463-465