

Subscribe to RSS
DOI: 10.1055/a-1559-2391
Efficacy and safety of cap-assisted endoscopic mucosal resection for treatment of nonlifting colorectal polyps
Authors

Abstract
Background Suboptimal lifting increases complexity of endoscopic mucosal resection (EMR) for benign colorectal polyps. Cap-assisted EMR (EMR-C) may allow fibrotic polyp tissue to be captured in the snare. This study evaluated the efficacy and safety of EMR-C for benign nonlifting colorectal polyps.
Methods This was a multicenter study, which prospectively registered all EMR-C procedures (2016–2018) for presumed benign nonlifting colorectal polyps.
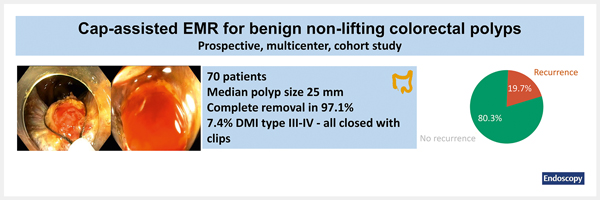
Results 70 nonlifting polyps with a median size of 25 mm (interquartile range [IQR] 15–40) were treated with EMR-C. Complete polyp removal was achieved in 68 (97.1 %), including 47 (67.1 %) with EMR-C alone. Overall, 66 polyps showed benign histology, and endoscopic follow-up after a median of 6 months (IQR 6–10) showed recurrence in 19.7 %. First (n = 10) and second (n = 2) benign recurrences were all treated endoscopically. Deep mural injury type III–V occurred in 7.4 % and was treated successfully with clips.
Conclusion EMR-C may be an alternative therapeutic option for removal of benign nonlifting polyp tissue. Although recurrence still occurs, repeat endoscopic therapy usually leads to complete polyp clearance.
Introduction
Endoscopic mucosal resection (EMR) is the preferred treatment for benign large nonpedunculated colorectal polyps [1]. However, nonlifting due to submucosal fibrosis is one of the most important reasons for incomplete resection [2]. Nonlifting is frequently encountered in recurrent or residual adenoma, but other forms of prior manipulation, inflammatory bowel diseases, and polyp prolapse are also known to induce submucosal fibrosis [3]. Malignant invasion should also be considered, as covert submucosal cancer is found in 7.6 %–10 % of large nonpedunculated colorectal polyps [4] [5]. Avulsion techniques have gained popularity for treatment of diminutive nonlifting (residual) adenoma, but seem less attractive for larger areas [6]. Cap-assisted EMR (EMR-C) has been described for the removal of flat colorectal polyps, but there are no reports about its potential efficacy for nonlifting polyps [7]. The aim of the current study was to evaluate the clinical efficacy and safety of EMR-C for fibrotic colorectal polyps.
Methods
Patients
This was a multicenter prospective cohort study of patients treated with EMR-C for nonlifting colorectal polyps. Patients were treated in two university and three regional centers in the Netherlands between May 2016 and September 2018. Inclusion criteria were polyps with nonlifting category ≥ 2 according to the Kato classification [8], without suspicion of submucosal invasion based on optical diagnosis or previous histology.
All patients signed informed consent. The study was approved by the Ethics Committee at the University Medical Centre Utrecht (reference number 17/179).
EMR-C technique
All endoscopic procedures were conducted by endoscopists with significant experience in colorectal EMR (≥ 50 procedures performed). Endoscopes with a working channel diameter of at least 3.2 mm were used to generate sufficient suction. A transparent soft cap (Olympus, straight, 12.4–14 mm – Olympus, Tokyo, Japan; or US Endoscopy, straight, 12.6–13.2 mm – US Endoscopy, Mentor, Ohio, USA), already used routinely in advanced EMR procedures, was positioned extending approximately 4 mm beyond the distal end of the endoscope. Polyp and target sizes were estimated by comparison with an open snare of known size. A 10- or 20-mm stiff round braided snare (Captivator snare; Boston Scientific, Marlborough, Massachusetts, USA) or 10–15-mm monofilament snare (Monofil; Medwork, Cleveland, Ohio, USA) was used. Standard EMR-C was performed ([Video 1]; see also Appendix 1 s in the online-only Supplementary material). Residual adenomatous tissue was treated with cold avulsion and/or ablation, using either argon plasma coagulation (APC; variable power and flow settings) or snare tip soft coagulation (STSC; 80 W, Effect 4). Adjuvant treatment using either APC or STSC was applied at the discretion of the endoscopist. The resection site was carefully examined for muscle injury but was not routinely clipped.
Follow-up endoscopy was routinely scheduled for 6 months after resection, but the interval could be prolonged by the treating physician. The scar was assessed for macroscopic features of recurrent adenoma using high-definition white light and narrow-band imaging by dedicated endoscopists. If recurrence was suspected, the lesion was removed and sent for histological confirmation. In cases of high certainty of absence of recurrence, no biopsies were taken.
Video 1 Two examples of cap-assisted endoscopic mucosal resection (EMR-C): first, EMR-C of a severely fibrotic nonlifting residual adenomatous island of 10 mm in the descending colon, complicated by intraprocedural bleeding; second, a 12-mm recurrent adenoma in the ascending colon resected by EMR-C in a piecemeal fashion.
Study outcomes
The primary outcome of the study was the rate of adenoma recurrence at first follow-up colonoscopy. The presence of recurrence was based on an endoscopic diagnosis of recurrent adenoma with histological confirmation.
Secondary outcomes were technical success and the occurrence of adverse events. Technical success was defined as macroscopic complete resection of the polyp after EMR-C, including adjunctive treatment if applied. The occurrence of deep mural injury (DMI) was considered the most relevant intraprocedural adverse event and was assessed according to the Sydney classification [9]. Delayed bleeding was defined as post-procedure bleeding that required reintervention, emergency department visit, or hospitalization [10].
Statistical analysis
Baseline and procedural characteristics were analyzed using standard descriptive statistics. Logistic univariable analysis and stepwise logistic regression analysis were performed to determine factors associated with recurrent adenoma. Statistical analysis was performed using SPSS version 25 (IBM Corp., Armonk, New York, USA).
Results
A total of 70 nonlifting polyps were resected by EMR-C in 70 patients (mean age 69.5 years, standard deviation 8.8; 65.7 % men). The most common cause of nonlifting was recurrent or residual adenoma (n = 51) ( [Table 1]). Median entire polyp size was 25 mm (interquartile range [IQR] 15–40 mm) and median size of the nonlifting target area was 15 mm (IQR 10–20 mm).
|
Characteristic |
Total (n = 70) |
|
Age, mean (SD), years |
69.5 (8.8) |
|
Male sex, n (%) |
46 (65.7) |
|
Polyp size, median (IQR), mm |
25 (15–40) |
|
Size of nonlifting lesion (target), median (IQR), mm |
15 (10–20) |
|
Target lesion size category, n (%) |
|
|
16 (22.9) |
|
28 (40.0) |
|
26 (37.1) |
|
Polyp location, n (%) |
|
|
13 (18.6) |
|
3 (4.3) |
|
24 (34.3) |
|
8 (11.4) |
|
2 (2.9) |
|
5 (7.1) |
|
14 (20.0) |
|
1 (1.4) |
|
Location[1], n (%) |
|
|
49 (70.0) |
|
21 (30.0) |
|
Granularity, n (%) |
|
|
41 (58.6) |
|
29 (41.4) |
|
Histology, n (%) |
|
|
26 (37.1) |
|
29 (41.4) |
|
5 (7.1) |
|
3 (4.3) |
|
4 (5.7) |
|
3 (4.3) |
|
Dysplasia, n (%) |
|
|
2 (2.9) |
|
46 (65.7) |
|
10 (14.3) |
|
5 (7.1) |
|
4 (5.7) |
|
3 (4.3) |
|
Nonlifting target area, n (%) |
|
|
35 (50.0) |
|
35 (50.0) |
|
Paris classification |
|
|
15 (21.4) |
|
48 (68.6) |
|
5 (7.1) |
|
2 (2.9) |
|
Level of nonlifting, n (%) |
|
|
6 (8.6) |
|
24 (34.3) |
|
39 (55.7) |
|
Reason for nonlifting, n (%) |
|
|
51 (72.9) |
|
8 (11.4) |
|
5 (7.1) |
|
6 (8.6) |
|
Previous treatment[2], n (%) |
|
|
49 (70) |
|
1 (1.4) |
|
48 (68.6) |
|
16 (22.9) |
|
18 (25.7) |
SD, standard deviation; IQR, interquartile range.
1 Location: proximal colon is defined as to the splenic flexure. Distal colon is starting from the descending colon.
2 n = 51; patients could have undergone more than one previous treatment.
Technical and clinical outcomes
Macroscopic complete removal of polyp tissue was achieved in nearly all patients (n = 68; 97.1 %) ( [Fig.1], [Fig.2]). In 47 patients (67.1 %) this was accomplished by EMR-C alone. Adjunctive treatment was performed in the remaining 21 patients using cold avulsion (n = 8), ablation (n = 6), or a combination of both (n = 7). In two cases, the residual tissue was too rigid to be suctioned into the cap and both cases were deemed noncandidates for adjunctive treatment. These patients were managed by surgery, and both showed a T2 adenocarcinoma in final histology (Table 1 s).


Adjuvant therapy was applied in nearly all patients (n = 65), including ablation of the margins (n = 63) and/or of the fibrotic resection site (n = 33). After complete removal, benign histology was reported in 66 /68 cases (97.1 %). Unexpectedly, invasive cancer was found in two patients (Table 1 s).
Follow-up
Endoscopic surveillance was performed in all 66 patients with benign histology. At the first surveillance at 6 months (IQR 6–10 months), recurrent adenoma was found in 13 patients (19.7 %), including 3 patients with malignant recurrence. The recurrence rate was similar between polyps completely removed by EMR-C alone (19.6 %) and those treated adjunctively (20.0 %). Target lesion size was the only factor significantly associated with recurrent adenoma at follow-up (odds ratio 1.09, 95 % confidence interval 1.01–1.17; P = 0.03) (Table 2 s). Recurrence was diagnosed in 6.7 %, 14.3 %, and 34.8 % after EMR-C for target lesions of < 10 mm (1/15), 10–19 mm (4/28), and ≥ 20 mm (8/23), respectively. Recurrence was successfully treated endoscopically in all 10 cases with benign histology by means of subsequent EMR-C combined with ablative therapy (n = 8), ablative therapy only (n = 1), and endoscopic full-thickness resection (n = 1). Second follow-up information was available for eight patients and was negative for recurrent adenoma in six.
Adverse events
DMI related to EMR-C occurred in six patients (8.8 %), including one transmural perforation (DMI IV), four target signs (DMI III), and one DMI type II, all located in the proximal colon. All DMIs were successfully treated with through-the-scope clips, without the need for surgery (Fig. 1 s). No delayed perforations were encountered. Delayed bleeding occurred in six patients (8.8 %) and could be managed endoscopically or was self-limiting.
Discussion
Nonlifting increases the complexity of EMR for benign colorectal polyps and is associated with higher rates of incomplete resection, recurrence, and adverse events [2] [3]. This is the first study to evaluate EMR-C for nonlifting polyps. We demonstrated that by incorporating EMR-C in the management of relatively large fibrotic areas, complete removal can be accomplished in 67.1 % with EMR-C alone and in nearly all patients when also applying adjunctive treatment. Although the recurrence rate was still 19.7 % at first follow-up, complete clearance was usually reached by repeat endoscopic therapy.
Endoscopic avulsion techniques such as hot or cold avulsion with snare tip coagulation (CAST) have been proposed as simple and effective techniques for treatment of nonlifting polyps [6] [11]. However, hot avulsion has been reported for relatively small areas with a mean of only 4.4 mm (range 1–15 mm) [6]. EMR-C is capable of excising larger pieces with the potential of achieving a complete resection with less fragmentation and, consequently, improved histological assessment. Incomplete EMR-C occurred in almost one-third of procedures, but residual adenoma was still easily managed by avulsion techniques. Another major advantage of EMR-C is that it requires only minimal adjustment to the standard lift-and-cut EMR technique. Advanced resection techniques, such as endoscopic submucosal dissection or endoscopic full-thickness resection, have also been suggested as salvage treatment [12] [13], but these require specific expertise.
EMR-C resulted in a recurrence rate of 19.7 % after the first round of treatment. Similar recurrence rates have been described after CAST, hot avulsion, APC, and underwater EMR for recurrent or nonlifting polyps: 15.2 %–27.5 %, 15 %, 59.3 %, and 10 %, respectively [6] [11] [14] [15]. However, these data only come from nonrandomized studies, which makes it impossible to compare outcomes. The size of residual polyp tissue treated by EMR-C in our cohort was relatively large (median size of 15 mm) and severe fibrosis (Kato III/IV nonlifting) was present in the majority of cases. The size of the nonlifting area in particular seems to raise the level of difficulty, as this was significantly associated with recurrent adenoma at follow-up.
EMR-C performed by experienced endoscopists can be considered a relatively safe technique for nonlifting polyps, with advanced DMI type (III–V) occurring in 7.4 %, none of which required surgery. This incidence is similar to other techniques for nonlifting polyps, such as CAST, which is associated with an advanced DMI risk of 5.3 % [11]. It also compares favorably to a 16.7 % perforation risk of endoscopic submucosal dissection for polyps with severe fibrosis [13]. A possible explanation for the relatively low perforation risk of EMR-C could be the limited cap depth of only 4 mm combined with a more rigid colorectal wall due to extensive submucosal fibrosis.
A major limitation of our study is the frequent application of adjuvant and adjunctive therapy, which makes the exact influence of EMR-C on recurrence difficult to determine. Second, EMR-C was performed by endoscopists with significant skill in interventional endoscopy. However, we believe that this technique can also be mastered relatively easily by less experienced endoscopists.
In conclusion, EMR-C was capable of resecting benign nonlifting polyp tissue, although complete removal required repeated intervention in some cases.
Competing interests
Paul Didden, Leon Moons and Frank Vleggaar declare that they were employed as consultants for Boston Scientific in the past 3 years.
-
References
- 1 Ferlitsch M, Moss A, Hassan C. et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017; 49: 270-297
- 2 Moss A, Williams SJ, Hourigan LF. et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 2015; 64: 57-65
- 3 Kim HG, Thosani N, Banerjee S. et al. Effect of prior biopsy sampling, tattoo placement, and snare sampling on endoscopic resection of large nonpedunculated colorectal lesions. Gastrointest Endosc 2015; 81: 204-213
- 4 Burgess NG, Hourigan LF, Zanati SA. et al. Risk stratification for covert invasive cancer among patients referred for colonic endoscopic mucosal resection: a large multicenter cohort. Gastroenterology 2017; 153: 732-742
- 5 D’Amico F, Amato A, Iannone A. et al. Risk of covert submucosal cancer in patients with granular mixed laterally spreading tumors. Clin Gastroenterol Hepatol 2021; 19: 1395-1401
- 6 Veerappan SG, Ormonde D, Yusoff IF. et al. Hot avulsion: a modification of an existing technique for management of nonlifting areas of a polyp (with video). Gastrointest Endosc 2014; 80: 884-888
- 7 Kashani A, Lo SK, Jamil LH. Cap-assisted endoscopic mucosal resection is highly effective for nonpedunculated colorectal lesions. J Clin Gastroenterol 2016; 50: 163-168
- 8 Kato H, Haga S, Endo S. et al. Lifting of lesions during endoscopic mucosal resection (EMR) of early colorectal cancer: implications for the assessment of resectability. Endoscopy 2001; 33: 568-573
- 9 Burgess NG, Bassan MS, McLeod D. et al. Deep mural injury and perforation after colonic endoscopic mucosal resection: a new classification and analysis of risk factors. Gut 2017; 66: 1779-1789
- 10 Burgess NG, Metz AJ, Williams SJ. et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol 2014; 12: 651-661
- 11 Tate DJ, Bahin FF, Desomer L. et al. Cold-forceps avulsion with adjuvant snare-tip soft coagulation (CAST) is an effective and safe strategy for the management of non-lifting large laterally spreading colonic lesions. Endoscopy 2018; 50: 52-62
- 12 Schmidt A, Beyna T, Schumacher B. et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018; 67: 1280-1289
- 13 Tanaka H, Oka S, Tanaka S. et al. Salvage endoscopic submucosal dissection for local residual/recurrent colorectal tumor after endoscopic resection: large multicenter 10-year study. Dig Endosc 2021; 33: 608-615
- 14 Holmes I, Kim HG, Yang DH. et al. Avulsion is superior to argon plasma coagulation for treatment of visible residual neoplasia during EMR of colorectal polyps (with videos). Gastrointest Endosc 2016; 84: 822-829
- 15 Kim HG, Thosani N, Banerjee S. et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video). Gastrointest Endosc 2014; 80: 1094-1102
Corresponding author
Publication History
Received: 12 November 2020
Accepted after revision: 03 July 2021
Article published online:
14 September 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Ferlitsch M, Moss A, Hassan C. et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017; 49: 270-297
- 2 Moss A, Williams SJ, Hourigan LF. et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 2015; 64: 57-65
- 3 Kim HG, Thosani N, Banerjee S. et al. Effect of prior biopsy sampling, tattoo placement, and snare sampling on endoscopic resection of large nonpedunculated colorectal lesions. Gastrointest Endosc 2015; 81: 204-213
- 4 Burgess NG, Hourigan LF, Zanati SA. et al. Risk stratification for covert invasive cancer among patients referred for colonic endoscopic mucosal resection: a large multicenter cohort. Gastroenterology 2017; 153: 732-742
- 5 D’Amico F, Amato A, Iannone A. et al. Risk of covert submucosal cancer in patients with granular mixed laterally spreading tumors. Clin Gastroenterol Hepatol 2021; 19: 1395-1401
- 6 Veerappan SG, Ormonde D, Yusoff IF. et al. Hot avulsion: a modification of an existing technique for management of nonlifting areas of a polyp (with video). Gastrointest Endosc 2014; 80: 884-888
- 7 Kashani A, Lo SK, Jamil LH. Cap-assisted endoscopic mucosal resection is highly effective for nonpedunculated colorectal lesions. J Clin Gastroenterol 2016; 50: 163-168
- 8 Kato H, Haga S, Endo S. et al. Lifting of lesions during endoscopic mucosal resection (EMR) of early colorectal cancer: implications for the assessment of resectability. Endoscopy 2001; 33: 568-573
- 9 Burgess NG, Bassan MS, McLeod D. et al. Deep mural injury and perforation after colonic endoscopic mucosal resection: a new classification and analysis of risk factors. Gut 2017; 66: 1779-1789
- 10 Burgess NG, Metz AJ, Williams SJ. et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol 2014; 12: 651-661
- 11 Tate DJ, Bahin FF, Desomer L. et al. Cold-forceps avulsion with adjuvant snare-tip soft coagulation (CAST) is an effective and safe strategy for the management of non-lifting large laterally spreading colonic lesions. Endoscopy 2018; 50: 52-62
- 12 Schmidt A, Beyna T, Schumacher B. et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018; 67: 1280-1289
- 13 Tanaka H, Oka S, Tanaka S. et al. Salvage endoscopic submucosal dissection for local residual/recurrent colorectal tumor after endoscopic resection: large multicenter 10-year study. Dig Endosc 2021; 33: 608-615
- 14 Holmes I, Kim HG, Yang DH. et al. Avulsion is superior to argon plasma coagulation for treatment of visible residual neoplasia during EMR of colorectal polyps (with videos). Gastrointest Endosc 2016; 84: 822-829
- 15 Kim HG, Thosani N, Banerjee S. et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video). Gastrointest Endosc 2014; 80: 1094-1102