Subscribe to RSS
DOI: 10.1055/a-1869-1772
Treatment in Certified Breast Cancer Centers Improves Chances of Survival of Patients with Breast Cancer
Evidence Based on Health Care Data from the WiZen Study Article in several languages: English | deutschAuthors
Clinical Trial: Registration number (trial ID): NCT04334239, Trial registry: ClinicalTrials.gov, Type of Study:

Abstract
Introduction
Certified breast cancer centers offer specific quality standards in terms of their structure, diagnostic and treatment approaches with regards to breast surgery, drug-based cancer therapy, radiotherapy, and psychosocial support. Such centers aim to improve treatment outcomes of breast cancer patients. The question investigated here was whether patients with primary breast cancer have a longer overall survival if they are treated in a certified breast cancer center compared to treatment outside these centers.
Methods
We used patient-specific data (demographics, diagnoses, treatments) obtained from data held by mandatory health insurance companies (gesetzliche Krankenversicherung, GKV) and clinical cancer registries (KKR) for the period 2009–2017 as well as hospital characteristics recorded in standardized quality reports. Using multivariable Cox regression analysis, we investigated differences in survival between patients treated in hospitals certified as breast cancers centers by the German Cancer Society (DKG) and patients treated in hospitals which had not been certified by the DKG.
Results
The sample population consisted of 143720 (GKV data) and 59780 (KKR data) patients with breast cancer, who were treated in 1010 hospitals across Germany (280 DKG-certified, 730 not DKG-certified). 63.5% (GKV data) and 66.7% (KKR data) of patients, respectively, were treated in DKG-certified breast cancer centers. Cox regression analysis for overall survival which included patient and hospital characteristics found a significantly lower mortality risk for patients treated in DKG-certified breast cancer centers (GKV data: HR = 0.77, 95% CI = 0.74–0.81; KKR data: HR = 0.88, 95% CI = 0.85–0.92). This result remained stable even after several sensitivity analyses including stratified estimates for subgroups of patients and hospitals. The effect was even more pronounced for recurrence-free survival (KKR data: HR = 0.78, 95% CI = 0.74–0.82).
Conclusions
Patients who are treated by an interdisciplinary team in a DKG-certified breast cancer had clear and statistically significantly better survival rates. Certification is therefore an effective means of improving the quality of care, and more patients should be treated in certified breast cancer centers.
Keywords
breast cancer - certification - outcome quality - health care research - health care-related dataIntroduction
Breast cancer is the most common cancer affecting women in Germany. According to the Robert Koch Institute, 71375 new cases with disease were recorded in 2019 (ICD-10 C50 Malignant neoplasm of breast), and the annual standardized incidence rate (per 100000 persons, ESR) was 114.6 for women and 1.2 for men [1]. In addition, around 6000 new cases of carcinoma in situ (DCIS) are diagnosed every year. This means that almost every 8th woman will develop breast cancer in her lifetime. The outcomes for this very large population are therefore highly relevant for the overall population, both economically and in terms of health-care policies. The current 5-year overall survival rate is 88% for women and 84% for men [2]. Mortality rates of breast cancer patients have decreased continuously since 1990, especially for women between the ages of 55 and 69 years [2]. This is also the age group who experienced the introduction of comprehensive mammography screening, which has led to fewer advanced tumors and more small tumors and carcinomas in situ being detected compared to the era before general screening [2].
Advances in breast cancer therapy have meant that the chances of long-term survival have increased significantly. The last decade, in particular, has seen the introduction of personalized targeted multimodal therapies which take account of distinct tumor biologies. The choice of systemic therapy used to treat breast cancer depends on the intrinsic subtype. HER2-neu receptor status, (steroid) hormone receptor status, grading and even the proliferation marker Ki-67 are important factors when choosing an individualized therapeutic approach. Prognostic and predictive factors determine the choice of therapy. In addition to tumor biology, the stage of disease is highly relevant for survival. There has been significant progress not just in the treatment of early breast cancer but also in the treatment of metastatic disease. Targeted therapies often allow disease to become chronic. In addition to prolonging survival, the goal is also to improve patients’ quality of life by offering therapies which patients tolerate well.
In Germany, certification programs were set up to implement the goals of the National Cancer Plan. The concept was that cancer patients would receive high-quality evidence-based therapy in accordance with current guidelines which would improve patient survival. In Germany, organ-specific certification programs are mainly run by the German Cancer Society (Deutsche Krebsgesellschaft e. V., DKG). Centers can be DKG-certified irrespective of whether they are also ISO-certified (e.g., DIN EN ISO 9001), and the two certification types should not be confused, as ISO does not evaluate content-related oncological quality parameters. The DKG introduced certification of breast cancer centers in 2003 [3]. There are currently 248 DKG-certified breast cancer centers in Germany [4]. Earlier studies reported varying results with regards to the outcomes of patients treated in certified breast cancer centers compared to treatment in non-certified hospitals [5] [6] [7]. But these early publications had certain limitations such as regional restrictions, limited time frames, and low numbers of cases.
The analysis we present here investigated differences in the survival of patients treated in DKG-certified breast cancer centers compared to patients cared for in non-certified hospitals in a large patient population. It was hypothesized that patients would benefit from treatment in certified centers.
Material and Methods
WiZen study
The cohort study on the effectiveness of care in certified cancer centers (German title: Wirksamkeit der Versorgung in onkologischen Zentren, WiZen) examined whether treatment in DKG-certified cancer centers offered benefits with regards to the survival of patients with different malignancies compared to patients treated in non-DKG-certified hospitals in Germany. The project received financial support from the Innovation Fund of the German Federal Joint Committee (grant no. 01VSF17020). The study evaluated patients with breast cancer, colorectal cancer, pancreatic cancer, lung cancer, prostate cancer, tumors of the head and neck, brain tumors and gynecological tumors. The results for breast cancer patients are presented below.
Data base
The used data were obtained, firstly, from the anonymized billing data of mandatory health insurance companies (GKV) collected across all of Germany for persons insured with the AOK in the period 2006–2017 and were provided by the Scientific Institute of the AOK (Wissenschaftliches Institut der AOK, WIdO). Performance data and master data from the subsets “master data of insured persons” in accordance with Sec. 284 SGB V, “outpatient care” (Sec. 295 SGB V), “inpatient care” (Sec. 301 SGB V) and “computerized physician order entries” (Sec. 300 Para. 1 SGB V) were brought together for analysis. A phase without diagnoses from 2006–2008 was used to determine the cancer incidence, leaving the period from 2009–2017 for analysis.
Anonymized data were also obtained from clinical cancer registries (KKR) in Brandenburg, Dresden, Erfurt, and Regensburg. The pooled datasets included initial diagnoses made in the period 2006–2017 as well as personal information and disease-specific data. To allow these data to be compared with the results of the analysis of the GKV data, the evaluated cohort was limited to the diagnostic years from 2009 to 2017.
Structural characteristics of hospitals obtained from publicly available structured quality reports in accordance with Sec. 136 SGB V and data on the DKG-certification of hospitals including the date of certification were used in addition to the data from the GKV and the KKR. The intervention group for the results presented here consists of patients treated in centers certified by the German Cancer Society (centers for specific cancer types and oncological centers).
Data were anonymized at patient and hospital levels, and data transfers were encrypted. The pseudonymization at both levels was carried out by the WIdO and the cancer registries which provided data, and the subsequent evaluations were carried out in the Center for Evidence-based Health Care (ZEGV) of Hochschulmedizin Dresden and the Regensburg Tumor Center (TZR) of the Center for Quality Assurance and Care Research of Regensburg University. The WiZen study was approved by the Ethics Commission of the TU Dresden (reference number: EK95022019) and was registered with ClinicalTrials.gov (ID: NCT04334239). Data processing and data analysis was done in accordance with the Declaration of Helsinki and the General Data Protection Regulation of the European Union.
Inclusion and exclusion criteria
Patients who were at least 18 years of age at diagnosis and who received an initial diagnosis of breast cancer (ICD-10-GM: C50, D05; cf. [8]) in the years 2009–2017 were included in the study. The choice of ICD-10 numbers was decided by a panel of clinical experts. Patients whose date of initial diagnosis was identical with their death date and patients where information on confounders was lacking or implausible were excluded. When reviewing the GKV data, patients who were not continuously insured by the AOK or who did not have an inpatient primary diagnosis (ICD-10-GM) of the investigated entity or who had an index treatment in a hospital within one year before the hospital received DKG certification were excluded. An index treatment was defined as the first entity-specific inpatient treatment for a primary or secondary diagnosis of the respective entity.
Endpoints
Primary endpoint was the overall survival time from the date of the index treatment (for GKV data) or initial diagnosis (for KKR data). The date of initial diagnosis was the date of the first histological confirmation of disease, excluding diagnoses which were registered as recurrences (KKR). Survival times of patients without a death date or with a death date after 2017 were treated as right censored data up until the end of the observation period on 31 December 2017. If the last known dataset for a patient with no death date in the KKR data included the information that the patient was still alive at the end of 2017, this was used for right censoring. Mean follow-up time was estimated using the reverse Kaplan-Meier method [9].
Relocations of patients did not affect the completeness of the GKV data as these data are collected nationally. With regards to the cancer registries, when a patient moves from one catchment area into the catchment area of another registry, the patient’s clinical data is transferred to the other registry as part of the general exchange of data between registries.
Recurrence-free survival was another endpoint. Other events in addition to death were local, regional, and distant metastatic recurrence. If events occurred in succession, the first recurrence event was used. Clear identification of recurrence events was only possible for KKR data, meaning that recurrence-free survival was only calculated for KKR data.
Intervention
An intervention was defined as treatment in a DKG-certified center. Patients whose initial treatment was carried out in a center which was already certified at the time of treatment were defined as the intervention group and patients treated in a non-certified hospital were the control group. This constituted so-called complex intervention [10]. The date of initial treatment, if recorded, was defined as the date of resection for the primary diagnosis of the respective entity, otherwise it was the date of the patient’s first stay in hospital. For the KKR data, the DKG certification status of the treating hospital at the time of the initial diagnosis was used if the code of the institution had been recorded. Otherwise, we used the case-related variable “treatment in center yes” used by all the registries, which is used in audit evaluations provided by the registries on regularly collected performance indicators. For hospitals groups and hospitals spread across several locations, all hospitals/locations were given the status of DKG-certified center if one of the institutes had the status, as it was not possible to directly assign the certification status to a specific institution.
Risk adjustment
Age group, sex, year of diagnosis or of index treatment and severity of disease were included in the risk adjustment of estimated center effects on patients as they were considered influencing variables. For the GKV data, disease severity was operationalized using the variables “distant metastasis,” “additional oncological disease” and “comorbidities.” For the KKR data, disease severity was operationalized using the following variables: invasive carcinoma vs. carcinoma in situ, stage (UICC), grading, lymph node/vascular invasion, hormone and HER2/neu receptor status. The entity-specific choice of comorbidities was done based on the comorbidities defined by Elixhauser et al. [11] and clinical expertise. For the GKV data, hospitals were classified according to number of beds, function as a university hospital and/or teaching hospital as well as the hospitals’ funding bodies in structured quality reports. Different models with gradually increasing numbers of variables were created. Only completely adjusted models (i.e., including all possible variables) are presented here. A complete overview of all risk adjustment variants is provided in the final report [8].
Statistical evaluation
To estimate center effects while taking the effects of possible explanatory variables/confounders into account, overall survival was modelled using multivariable Cox regression analysis and the calculated hazard ratios including 95% confidence intervals were recorded. By including a random effect for hospitals when using the GKV data, the Cox models also showed possible correlations for patient outcomes in hospitals [12]. These models are referred to as shared frailty Cox models.
Results
Description of investigated population
The sample consisted of 143720 (GKV data) or 59780 (KKR data) patients with breast cancer, who were treated in 1010 hospitals (280 DKG-certified cancer centers, 730 not DKG-certified centers). 63.5% (n = 91269, GKV data) or 66.7% (n = 39859, KKR data) of patients were treated in DKG-certified breast cancer centers ([Table 1], [Fig. 1]). No significant difference was found between certified and non-certified institutions with regards to patient characteristics (age, sex, clinical characteristics). However, the percentage of unknown values in the records of the KKR for certified centers was consistently lower than for non-certified institutions. Larger institutions were more likely to be certified than small hospitals. When considering whether DKG-certified institutions offer a possible survival benefit, the different characteristics of the hospitals also need to be considered.

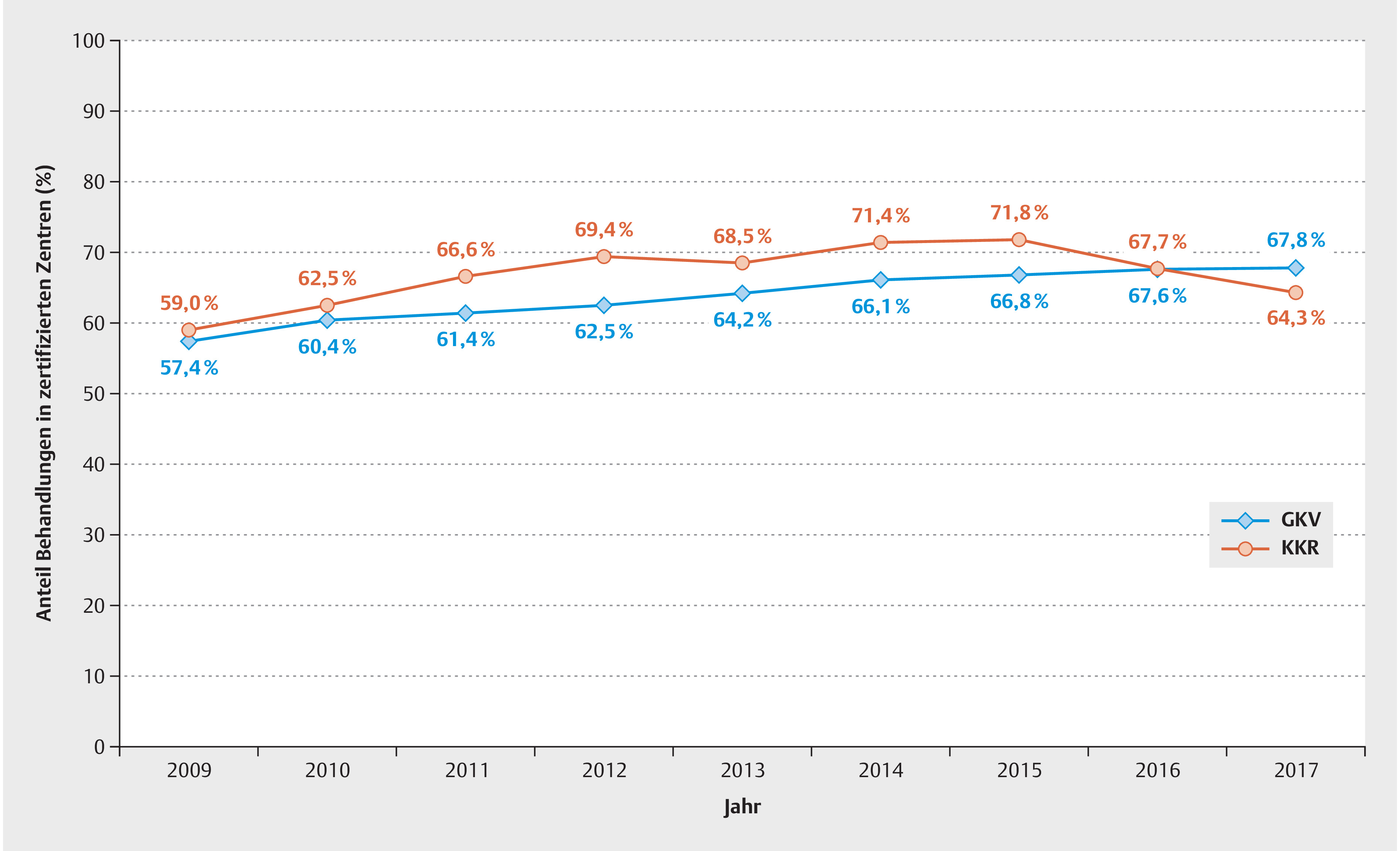
The percentage of patients with breast cancer treated in DKG-certified centers in the period 2009 to 2017 increased from 57.4% to 67.8% (GKV data) or from 59.0% to 64.4% (KKR data, [Fig. 2]).

Overall survival
The mean follow-up time for the total patient population was 3.4 years (median 3.1). The mean follow-up time was 3.5 years (median 3.2) for the cohort of patients treated in DKG-certified centers and 3.2 years (median 2.8) for the cohort of patients treated in hospitals which were not DKG-certified.
For both data sources, the unadjusted overall survival rate of patients with breast cancer treated in a certified center was significantly higher than the rates of patients who did not have an index treatment in a certified center ([Fig. 3]; GKV patients treated in a certified center: 5-year survival rate = 85.5%, 95% CI = [85.2%–85.7%] compared to patients not treated in a certified center: rate = 80.6%, 95% CI = [80.2%–80.9%]; KKR: 5-year survival rate = 79.0% [78.4%–79.6%] vs. 73.7% [72.7%–74.7%].

Point estimate values including the confidence intervals of the adjusted hazard ratios for center effects on overall survival were less than 1 for both the GKV data and the KKR data ([Table 2]; GKV: HR = 0.77, 95% CI = [0.74–0.81]; KKR: HR = 0.88, 95% CI = [0.85–0.92]). This means that there were significant survival benefits for patients treated in DKG-certified centers for both cohorts (GKV data: 23%; KKR data: 12%).
A stratified analysis which took account of the number of beds in the respective institution (1–299, 300–499, 500–999, 1000+) was carried out for the GKV data to test for possible effect modifications caused by the size of the treating hospital ([Table 2]). With the exception of the group of hospitals with 1–299 beds, the 95% confidence intervals of the estimated hazard ratios for center status overlapped; however, all point estimate values were less than 1 and a possible effect modification did not interfere with the basic statement. The KKR data were additionally analyzed to identify whether certification effects depended on disease severity (UICC stage) and whether the events for overall survival also translated to recurrence-free survival. The survival benefit from receiving treatment in a certified center was found to be more significant for patients with locally limited disease and locally advanced disease (I-III) compared to patients with advanced stage IV disease. A significant survival benefit was found for patients with stage I-III disease (HR = 0.89; 95% CI = [0.85–0.93]) but not for stage IV patients with primary distant metastatic disease (HR = 1.02; 95% CI = [0.94–1.11]).
Recurrence-free survival
Recurrence-free survival was investigated in patients with R0 resection who did not have primary distant metastasis using the KKR data. The observed effects were even more significant than those identified for overall survival (HR = 0.78; 95% CI = [0.74–0.82]). Subgroup analysis of the KKR data showed comparable estimators for overall survival for the patient cohort which included both patients for whom data on their stage of disease was lacking and patients for whom data about disease severity was available. Additional analysis results for all model specifications are available in the final report of the WiZen study [8].
Subgroup analysis
The estimation results of the GKV data remained robust to stratifications based on sex (male/female), other oncological diseases (yes/no), single hospital/hospital group, distant metastasis (yes/no), tumor resection (yes/no) and number of hospital beds (< 500/ >= 500) (online supplement Table S1). The significant survival benefit observed for the KKR cohort was confirmed in most subgroup analyses, except for those patients who were male, patients diagnosed before the age of 50, patients with stage IV disease or negative hormone receptor status and positive HER2/neu receptor status ([Table 2], online supplement Table S1). The certification effect was even more pronounced for DKG-certified centers which had been certified for longer: while the estimated HR for breast cancer centers certified for less than one year was 0.82 (95% CI = [0.75–0.89]), the HR for centers certified for 5 or more years was 0.74 (95% CI = [0.71–0.78]) (online supplement Table S2).
Discussion
The aim of the National Cancer Plan introduced in 2008 was to develop cancer screening and patient orientation further to optimize oncological care structures and associated quality assurance measures. Previously, only regional analyses on breast cancer were available for Germany. These regional studies suggested that treatment in DKG-certified hospitals could be associated with a survival benefit [13]. In certified institutions, structural and content-related parameters are regularly evaluated and quality indicators are reviewed. The goal is to provide specialized interdisciplinary quality-oriented therapy based on current guidelines which also offers patients the option of participating in studies. Annual certification is associated with high personnel and financial costs [14] [15]; it is therefore important to have reproducible data showing that this expenditure is justified and that the benefit is reflected in longer overall survival rates.
A recent review showed that guideline-based therapies and the implementation of consensus recommendations leads to better survival rates for breast cancer patients [16]. Overall, a higher percentage of patients with breast cancer are treated in DKG-certified centers than patients with other oncological entities [8] [17].
This analysis used large data volumes to provide a representative evaluation of the treatment situation in Germany. Our study showed that, according to the KKR data, information on patients’ hormone receptor status (in 19.0%) and HER2-neu status (in 12.1%) were more likely to be missing if patients were treated in non-DKG-certified hospitals compared to DKG-certified centers. If the reported figures represent actual diagnostic workups, then they are inacceptable because when information about these predictive parameters is missing it is impossible to provide the optimal therapy.
The treatment of breast cancer is becoming ever more complex; many factors already need to be considered during the initial diagnosis in a non-metastatic situation to ensure that the chosen therapy is the optimal choice for the patient. Tumor size, lymph node status, grading and proliferation marker Ki-67 all play a role in decision-making in addition to (steroid) hormone receptor status and HER2/neu receptor status. When early-stage breast cancer is initially diagnosed, a decision will have to be taken on whether primary treatment should consist of surgery followed by adjuvant therapy or whether – if chemotherapy is indicated – it should be carried out as neoadjuvant therapy or whether endocrine therapy is sufficient and chemotherapy not required as the hormone receptor-positive patient is low risk. Patients who are HER2/neu-positive should receive anti-HER2-targeted therapy in addition to chemotherapy [18]. Additional immune therapy should be considered for cases with early high-risk triple negative breast cancer [19]. There are strong indications that new treatment options are implemented relatively quickly in DKG-certified centers once they have been included in the S3-guideline on breast cancer (e.g., trastuzumab for patients who are HER2-positive). Further analyses of data from breast cancer centers could show that the improved study outcomes in terms of pathological complete remission after neoadjuvant therapy for HER2-positive and triple negative breast cancers can be reproduced in routine treatment [20] [21].
Our analysis confirmed a significant certification effect for hormone receptor-positive and HER2/neu-negative breast cancer but not for patients who were HER2/neu-positive.
In addition to making the right diagnosis, the care of patients and management of potential toxicities is decisive. This is why further training in drug-based tumor therapies and specialist training in gynecological oncology was added to the advanced training of gynecologists in 2005 [20]. Specialist training in gynecological oncology does not only focus on surgical expertise but also on providing a detailed knowledge of systemic therapies with the aim of improving patient care [20].
Our analysis was able to show that overall survival of breast cancer patients treated in DKG-certified centers was significantly longer, demonstrating that the significant expenditure associated with certification is beneficial for patients. It is well known that certification entails additional costs because of the need to adapt structures and processes and carry out audits [22] [23]. But the additional costs associated with certification can also yield economic benefits as was shown by Cheng et al. in their cost-effectiveness analysis (CEA) for bowel cancer [24].
It is also worth pointing out that the quality of treatment provided even in certified centers is continually improving. This is made evident by the fact that survival benefits increased, the longer the center had been DKG certified.
Limitations and strengths
Selectivity of the analyzed cohort was low as documenting GKV billing data is governed by legal regulations and recording KKR data has been compulsory since the German law on cancer screening and registration (Krebsfrüherkennungs- und -registergesetz, KFRG) came into effect. Even before the KFRG was passed, KKR data were almost complete. Both data sources included extensive patient-specific risk factors such as comorbidities or information about disease severity. Characteristics of the treating hospitals were included in the analysis of the GKV data. Unfortunately, some of the influencing variables were only available for one of the data sources, and no information was available about socioeconomic status. Most of the information about certification was provided directly by the DKG and is therefore highly valid for the question investigated here. As the German federal state of North Rhine-Westphalia uses a different certification system, known as Äkzert, to certify breast cancer centers, data from North Rhine-Westphalia could not be used because the definitions and approaches differed from those used for DKG certification. This analysis still used data from all German federal states (which included 21843 patients who were resident in North Rhine-Westphalia; for more details, see the WiZen final report [8]). It can therefore be assumed that the estimates shown here may even underestimate the certification effect.
As patient volumes (i.e., the number of cases receiving relevant treatment per hospital) can have an impact on relevant outcomes such as survival [21] [25] [26] and a minimum patient volume is required for DKG certification, some of the results presented here could be ascribed to volume effects. As the GKV data were obtained from a single health insurance provider and not all patients included in the KKR could be assigned to a specific main treating hospital, it was not possible to quantify the total volume of patients in the various treating hospitals and include this in the analysis. Extending the DKG certification status of individual hospitals to the entire group of hospitals may even result in a conservative (i.e., low in absolute numbers) estimate of the center effect.
The difference in the strength of the center effect between the two data sources was evident despite adjustment for several confounders. This could be due to differences in the analyzed populations, hospitals, and data generation or to natural variation. The fact that both data sources qualitatively showed a statistically significant effect strengthens the robustness of the deduced inference of a survival benefit for patients treated in DKG-certified centers.
Overall, care should be taken before making any causal interpretations of the findings. On the one hand, certification status represents a complex arrangement of interventions at the level of the treating institutions which are difficult to quantify. On the other hand, it was not possible to randomize the cohort due to the structure of the certification system and the use of secondary data/data from cancer registries. It was nevertheless possible to carry out a valid examination of the effect of DKG certification by using different data sources and including relevant patient data, tumor characteristics, and hospital features in the risk adjustment. This minimized the risk of bias and allowed the certification effect to be compared across different types of cancers.
Conclusion
Our analysis provides robust evidence that patients treated in DKG-certified breast cancer centers have better survival rates. There are many reasons for the longer overall survival rates. It can be assumed that certified centers are more likely to offer individualized and guideline-based therapies as well as the option of early access to innovative therapies [20] [21].
Online Supplement
-
Supplement Table S1: Sensitivity analysis – hazard ratio for the adjusted certification effect for subgroups according to the basic data.
-
Supplement Table S2: Sensitivity analysis – ratio for the adjusted certification effect according to how long the institution has been certified (GKV data).
Conflict of Interest
OS, VB, CB and JS work in a university hospital with certified cancer centers, and MR previously also worked there. In addition, they received grants from the Innovation Fund of the Federal Joint Committee when carrying out the study. Independently of this study, JS received institutional grants for investigator-initiated research from the G-BA, the BMG, BMBF, the EU, the German Federal State of Saxony, Novartis, Sanofi, ALK and Pfizer. He also took part in Advisory Board Meetings as a paid consultant for Sanofi, Lilly and the ALK. Independently of this study, OS was a paid consultant for Novartis. He is also a member of the certification committee “Skin Cancer Centers” of the German Cancer Society and a member of the panel of experts for the project “Research into criteria to evaluate certificates and quality seals in accordance with Sec. 137a para. 3 sentence 2 No. 7 SGB V” for the Institute for Quality Assurance and Transparency in Healthcare (IQTIG). PW heads the DKG-certified Breast and Gynecological Cancer Center at the university hospital of Dresden University of Technology and is an additional member of the Board of Directors of NCT Dresden. PW is receiving institutional grants for investigator-initiated research from the DFG, Krebshilfe, Sächsische Aufbaubank (SAB), Gynäko-Onkologische Forschungsstiftung, Amgen, AstraZeneca, MSD, Novartis, Pfizer, Roche, Clovis, GSK. PW receives honoraria as an Advisory Board member for Amgen, AstraZeneca, MSD, Novartis, Pfizer, Lilly, Roche, Teva, Eisai, Gilead, GSK and Daiichi Sankyo. AS is the speaker for the Certification Committee for Breast Cancer Centers of the DKG and for many years he was the director of gynecological hospitals with certified breast cancer centers. He has had no financially relevant cooperations with industry in the last 4 years. ECI and OO work in a certified breast cancer center, gynecological cancer center and oncological center. OO is a member of the Executive Board of the German Cancer Society, head of the University Cancer Center Regensburg and a member of the Board of Directors of CCC WERA. TL works in a certified breast and gynecological cancer center. TL has received honoraria (lectures/consultancy work/travel costs) from Novartis, Roche, Amgen, GSK, Pfizer, Gilead, Daiichi Sankyo, AstraZeneca, Lilly, Myriad, MSD and Esai. TP is head of a DKG-certified breast and gynecological cancer center. St. Marien Amberg Medical Center is also an oncology center according to the criteria of the DKG. The other authors state that they have no conflict of interest.
Acknowledgement
We would like to thank PD Dr. Simone Wesselmann, PD Dr. Christoph Kowalski (DKG), Carmen Werner, Antje Niedostatek (KKR Dresden), Dr. Paul Strecker (KKR Erfurt) and Dr. Anett Tillack (KKRBB) for providing data and advice.
-
References/Literatur
- 1 Zentrum für Krebsregisterdaten im Robert Koch-Institut. Datenbankabfrage mit Schätzung der Inzidenz, Prävalenz und des Überlebens von Krebs in Deutschland auf Basis der epidemiologischen Landeskrebsregisterdaten.
- 2 GEKID, ZfKD. Krebs in Deutschland für 2017/2018. Berlin: Robert Koch-Institut; 2021
- 3 Brucker SY, Schumacher C, Sohn C. et al. Benchmarking the quality of breast cancer care in a nationwide voluntary system: the first five-year results (2003–2007) from Germany as a proof of concept. BMC Cancer 2008; 8: 358
- 4 DKG (Deutsche Krebsgesellschaft). Jahresbericht der zertifizierten Brustkrebszentren – Auditjahr 2021/Kennzahlenjahr 2020. Berlin: DKG (Deutsche Krebsgesellschaft); 2022
- 5 Beckmann MW, Brucker C, Hanf V. et al. Quality assured health care in certified breast centers and improvement of the prognosis of breast cancer patients. Onkologie 2011; 34: 362-367
- 6 Schrodi S, Tillack A, Niedostatek A. et al. No Survival Benefit for Patients with Treatment in Certified Breast Centers-A Population-based Evaluation of German Cancer Registry Data. Breast J 2015; 21: 490-500
- 7 Heil J, Gondos A, Rauch G. et al. Outcome analysis of patients with primary breast cancer initially treated at a certified academic breast unit. Breast 2012; 21: 303-308
- 8 Schoffer O, Rößler M, Bierbaum V, Bobeth C, Gerken M, Kleihues-van Tol K, Dröge P, Ruhnke T, Hasselberg A, Günster C, Klinkhammer-Schalke M, Schmitt J. Ergebnisbericht zum Projekt Wirksamkeit der Versorgung in onkologischen Zentren (WiZen). Berlin: Gemeinsamer Bundesausschuss – Innovationsausschuss; 2022. Accessed August 11, 2023 at: https://innovationsfonds.g-ba.de/downloads/beschluss-dokumente/268/2022–10–17_WiZen_Ergebnisbericht.pdf
- 9 Shuster JJ. Median follow-up in clinical trials. J Clin Oncol 1991; 9: 191-192
- 10 Mühlhauser I, Lenz M, Meyer G. Bewertung von komplexen Interventionen: Eine methodische Herausforderung. Dtsch Arztebl Int 2012; 109: 22-23
- 11 Elixhauser A, Steiner C, Harris DR. et al. Comorbidity measures for use with administrative data. Med Care 1998; 36: 8-27
- 12 Balan TA, Putter H. A tutorial on frailty models. Stat Methods Med Res 2020; 29: 3424-3454
- 13 Kreienberg R, Wockel A, Wischnewsky M. Highly significant improvement in guideline adherence, relapse-free and overall survival in breast cancer patients when treated at certified breast cancer centres: An evaluation of 8323 patients. Breast 2018; 40: 54-59
- 14 Beckmann MW, Bani MR, Loehberg CR. et al. Are Certified Breast Centers Cost-Effective?. Breast Care (Basel) 2009; 4: 245-250
- 15 Lux MP, Sell CS, Fasching PA. et al. Time and Resources Needed to Document Patients with Breast Cancer from Primary Diagnosis to Follow-up – Results of a Single-center Study. Geburtshilfe Frauenheilkd 2014; 74: 743-751
- 16 Miller K, Kreis IA, Gannon MR. et al. The association between guideline adherence, age and overall survival among women with non-metastatic breast cancer: A systematic review. Cancer Treat Rev 2022; 104: 102353
- 17 Schmitt J, Klinkhammer-Schalke M, Bierbaum V. et al. Initial Cancer Treatment in Certified Versus Non-Certified Hospitals-Results of the WiZen Comparative Cohort Study. Dtsch Arztebl Int 2023;
- 18 AGO (Arbeitsgemeinschaft Gynäkologische Onkologie). Leitlinien/Empfehlungen – Empfehlungen gynäkologische Onkologie Kommission Mamma. 2022 Accessed August 11, 2023 at: https://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma
- 19 Schmid P, Cortes J, Dent R. et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N Engl J Med 2022; 386: 556-567
- 20 Beckmann MW, Gitsch G, Emons G. et al. Qualification and education in gynecological oncology. Zentralbl Gynakol 2006; 128: 1-4
- 21 Chioreso C, Del Vecchio N, Schweizer ML. et al. Association Between Hospital and Surgeon Volume and Rectal Cancer Surgery Outcomes in Patients With Rectal Cancer Treated Since 2000: Systematic Literature Review and Meta-analysis. Dis Colon Rectum 2018; 61: 1320-1332
- 22 Wagner S, Bani M, Fasching P. et al. Ist ein Brustzentrum finanzierbar? – Berechnung einzelner Leistungen am Beispiel des Universitäts-Brustzentrums Franken (UBF). Geburtshilfe Frauenheilkd 2008; 68: 1178-1183
- 23 Hölterhoff M, Klein R, Anders M, Henkel M, Resnischek C, Riedel W, Vollmer J. Nutzen, Mehraufwand und Finanzierung von Onkologischen Spitzenzentren, Onkologischen Zentren und Organkrebszentren. Berlin/Düsseldorf: Prognos AG; 2017
- 24 Cheng CY, Datzmann T, Hernandez D. et al. Do certified cancer centers provide more cost-effective care? A health economic analysis of colon cancer care in Germany using administrative data. Int J Cancer 2021; 149: 1744-1754
- 25 Comber H, Sharp L, Timmons A. et al. Quality of rectal cancer surgery and its relationship to surgeon and hospital caseload: a population-based study. Colorectal Dis 2012; 14: e692-e700
- 26 Morche J, Mathes T, Pieper D. Relationship between surgeon volume and outcomes: a systematic review of systematic reviews. Syst Rev 2016; 5: 204
Correspondence
Publication History
Received: 14 August 2023
Accepted after revision: 16 November 2023
Article published online:
09 January 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References/Literatur
- 1 Zentrum für Krebsregisterdaten im Robert Koch-Institut. Datenbankabfrage mit Schätzung der Inzidenz, Prävalenz und des Überlebens von Krebs in Deutschland auf Basis der epidemiologischen Landeskrebsregisterdaten.
- 2 GEKID, ZfKD. Krebs in Deutschland für 2017/2018. Berlin: Robert Koch-Institut; 2021
- 3 Brucker SY, Schumacher C, Sohn C. et al. Benchmarking the quality of breast cancer care in a nationwide voluntary system: the first five-year results (2003–2007) from Germany as a proof of concept. BMC Cancer 2008; 8: 358
- 4 DKG (Deutsche Krebsgesellschaft). Jahresbericht der zertifizierten Brustkrebszentren – Auditjahr 2021/Kennzahlenjahr 2020. Berlin: DKG (Deutsche Krebsgesellschaft); 2022
- 5 Beckmann MW, Brucker C, Hanf V. et al. Quality assured health care in certified breast centers and improvement of the prognosis of breast cancer patients. Onkologie 2011; 34: 362-367
- 6 Schrodi S, Tillack A, Niedostatek A. et al. No Survival Benefit for Patients with Treatment in Certified Breast Centers-A Population-based Evaluation of German Cancer Registry Data. Breast J 2015; 21: 490-500
- 7 Heil J, Gondos A, Rauch G. et al. Outcome analysis of patients with primary breast cancer initially treated at a certified academic breast unit. Breast 2012; 21: 303-308
- 8 Schoffer O, Rößler M, Bierbaum V, Bobeth C, Gerken M, Kleihues-van Tol K, Dröge P, Ruhnke T, Hasselberg A, Günster C, Klinkhammer-Schalke M, Schmitt J. Ergebnisbericht zum Projekt Wirksamkeit der Versorgung in onkologischen Zentren (WiZen). Berlin: Gemeinsamer Bundesausschuss – Innovationsausschuss; 2022. Accessed August 11, 2023 at: https://innovationsfonds.g-ba.de/downloads/beschluss-dokumente/268/2022–10–17_WiZen_Ergebnisbericht.pdf
- 9 Shuster JJ. Median follow-up in clinical trials. J Clin Oncol 1991; 9: 191-192
- 10 Mühlhauser I, Lenz M, Meyer G. Bewertung von komplexen Interventionen: Eine methodische Herausforderung. Dtsch Arztebl Int 2012; 109: 22-23
- 11 Elixhauser A, Steiner C, Harris DR. et al. Comorbidity measures for use with administrative data. Med Care 1998; 36: 8-27
- 12 Balan TA, Putter H. A tutorial on frailty models. Stat Methods Med Res 2020; 29: 3424-3454
- 13 Kreienberg R, Wockel A, Wischnewsky M. Highly significant improvement in guideline adherence, relapse-free and overall survival in breast cancer patients when treated at certified breast cancer centres: An evaluation of 8323 patients. Breast 2018; 40: 54-59
- 14 Beckmann MW, Bani MR, Loehberg CR. et al. Are Certified Breast Centers Cost-Effective?. Breast Care (Basel) 2009; 4: 245-250
- 15 Lux MP, Sell CS, Fasching PA. et al. Time and Resources Needed to Document Patients with Breast Cancer from Primary Diagnosis to Follow-up – Results of a Single-center Study. Geburtshilfe Frauenheilkd 2014; 74: 743-751
- 16 Miller K, Kreis IA, Gannon MR. et al. The association between guideline adherence, age and overall survival among women with non-metastatic breast cancer: A systematic review. Cancer Treat Rev 2022; 104: 102353
- 17 Schmitt J, Klinkhammer-Schalke M, Bierbaum V. et al. Initial Cancer Treatment in Certified Versus Non-Certified Hospitals-Results of the WiZen Comparative Cohort Study. Dtsch Arztebl Int 2023;
- 18 AGO (Arbeitsgemeinschaft Gynäkologische Onkologie). Leitlinien/Empfehlungen – Empfehlungen gynäkologische Onkologie Kommission Mamma. 2022 Accessed August 11, 2023 at: https://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma
- 19 Schmid P, Cortes J, Dent R. et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N Engl J Med 2022; 386: 556-567
- 20 Beckmann MW, Gitsch G, Emons G. et al. Qualification and education in gynecological oncology. Zentralbl Gynakol 2006; 128: 1-4
- 21 Chioreso C, Del Vecchio N, Schweizer ML. et al. Association Between Hospital and Surgeon Volume and Rectal Cancer Surgery Outcomes in Patients With Rectal Cancer Treated Since 2000: Systematic Literature Review and Meta-analysis. Dis Colon Rectum 2018; 61: 1320-1332
- 22 Wagner S, Bani M, Fasching P. et al. Ist ein Brustzentrum finanzierbar? – Berechnung einzelner Leistungen am Beispiel des Universitäts-Brustzentrums Franken (UBF). Geburtshilfe Frauenheilkd 2008; 68: 1178-1183
- 23 Hölterhoff M, Klein R, Anders M, Henkel M, Resnischek C, Riedel W, Vollmer J. Nutzen, Mehraufwand und Finanzierung von Onkologischen Spitzenzentren, Onkologischen Zentren und Organkrebszentren. Berlin/Düsseldorf: Prognos AG; 2017
- 24 Cheng CY, Datzmann T, Hernandez D. et al. Do certified cancer centers provide more cost-effective care? A health economic analysis of colon cancer care in Germany using administrative data. Int J Cancer 2021; 149: 1744-1754
- 25 Comber H, Sharp L, Timmons A. et al. Quality of rectal cancer surgery and its relationship to surgeon and hospital caseload: a population-based study. Colorectal Dis 2012; 14: e692-e700
- 26 Morche J, Mathes T, Pieper D. Relationship between surgeon volume and outcomes: a systematic review of systematic reviews. Syst Rev 2016; 5: 204