

Subscribe to RSS
DOI: 10.1055/a-2175-3215
Comparing Three-dimensional and Two-dimensional Preoperative Planning for Lumbar Transpedicular Screw Placement: A Retrospective Study
Authors
Funding None.


Abstract
Background Transpedicular screw (TPS) misplacement is still a nightmare for spine surgeons. Preoperative planning is one of the methods that a surgeon could use to minimize this complication. This study aims to compare the efficacy of three-dimensional (3D) and two-dimensional (2D) preoperative planning in posterior lumbar TPSs placement performed using the freehand technique.
Patients and Methods Patients who underwent posterior TPSs placement for degenerative lumbar spondylolisthesis or spinal stenosis using the freehand technique between November 2021 and October 2022 were evaluated retrospectively. In total, 33 and 30 patients who met the inclusion criteria were consecutively operated on with preoperative 2D and 3D planning, respectively. The patients were divided into the 2D preoperative planning group (2DG) and 3D preoperative planning group (3DG) and the two groups were compared.
Results Sixty-three patients were operated during the study period. There was no significant difference between the groups regarding blood transfusion, operation time, and radiation exposure. Although the accuracy of TPSs positioning was 94.2 and 96.5% in the 2DG and 3DG, respectively, the difference between the groups was not statistically significant. The upper facet joint violation rate was 12.8% (n = 20) in the 2DG versus 3.5% (n = 5) in the 3DG (p = 0.006). All L4 TPSs were inserted with their standard entry points without any modification (p < 0.0001; relative/risk ratio = 0.64). The modification rate was higher in L1, L2, and L5 TPSs (p < 0.0001; χ 2 = 24.7).
Conclusion For patients with degenerative lumbar diseases, 3D preoperative planning in posterior lumbar instrumentation surgeries performed with the freehand technique decreased the upper facet joint violation rate.
Keywords
transpedicular screws - lumbar spine - three-dimensional measurement accuracy - software - facet joint violationIntroduction
Posterior pedicle screw instrumentation is still a standard surgical procedure to stabilize the instability caused by several diseases and accidents such as trauma, deformity, tumor, infection, and degenerative diseases. Although most individuals have the same lumbar anatomy rich in neural, vascular, and visceral structures, some patients have anatomical variants. In such cases, these structures can be damaged by misplacements of the transpedicular screws (TPSs).[1] [2] Neurologic complication rates in posterior pedicle screw instrumentation vary between 0.6 and 11%.[3] In addition, the pedicle damage may weaken the bony structure and stabilization of the instrumentation.[1] [4] Preoperative planning is one of the methods that a surgeon could use to minimize misplacement.[1] [2] [4] For this purpose, fluoroscopy, computed tomography (CT) navigation, and robotic systems have been developed to improve screw placement accuracy.[1] [4]
The freehand technique is the most commonly used technique to insert TPS, which has several advantages over other techniques, such as being more practical, having no additional cost, and less radiation exposure. In the freehand technique, the screw is inserted using anatomical landmarks. In patients with degenerative spinal diseases or anatomical variants, who constitute the majority of cases needing pedicle screw placement, it may be difficult to recognize the anatomical landmarks in the posterior elements to determine the pedicle entry point.[5] Since the vertebral anatomical structure of each patient is different, it is not possible to standardize the ideal screw trajectory.[6] Failure to determine the appropriate entry point and angulation may cause pedicle breach and upper facet joint violation. According to the literature, the average rate of appropriate screw placement is 93.1% in screws placed with the freehand technique.[7]
Several studies have demonstrated that determining the entry sites and pedicle angles by preoperative modeling with three-dimensional (3D) CT-based reconstruction can counteract a few drawbacks of the freehand technique.[8] [9] [10] [11] Our hypothesis states that 3D, when compared to two-dimensional (2D), preoperative planning for patients with degenerative spinal diseases can reduce the complication of TPS misplacement. In this study, the authors aimed to compare 3D and 2D preoperative planning in posterior lumbar TPSs placement performed using the freehand technique regarding the demographic and clinical characteristics, upper facet joint violation, pedicle breach, and blood transfusion.
Patients and Methods
Patient Groups and Criteria
This comparative retrospective study was approved by the ethical committee of Atlas University (AU) on November 8, 2022, under decision number: E-22686390-050.99-21531. Patients who underwent posterior lumbar instrumentation for lumbar degenerative diseases at the hospital setting from November 2021 to October 2022 were enrolled.
The inclusion criteria were (1) radiological diagnoses of degenerative diseases (i.e., lumbar degenerative spondylolisthesis or spinal stenosis) by dynamic X-rays, CT, and magnetic resonance imaging (MRI), (2) undergoing posterior instrumentation placement for the first time, (3) no age restriction, although degenerative diseases usually develop in middle-aged and elderly population, (4) underwentsurgery with 2D or 3D preoperative planning, and (5) consent to participate in the study and surgical procedure.
The surgical criteria were one or more of the following: (1) back and/or leg pain with or without refractory radiculopathy, (2) no response to 12 weeks of conservative treatment,[12] (3) presence of advanced neurologic deficits (sensory disturbance-induced ataxia gait or function restriction, motor deficits with strength grade ≤2/5, or urinary incontinence[13]), and (4) patient's preference.
The exclusion criteria were (1) another type of spondylolisthesis (congenital, traumatic, iatrogenic, isthmic, or pathologic), (2) malformations that needed correction by surgeries such as hemivertebrae, kyphosis, or scoliosis, (3) advanced osteoporosis with T-score less than −2.5 (3D reconstruction does not yield good outcomes in such patients), (4) specific neurological diseases, (5) unavailable pre- or postoperative X-rays, CT, or MRI, (6) rejection to participate, (7) surgeries extending to the thoracic or sacral regions, and (8) metabolic bone disease, inflammatory arthritis, or other rheumatologic diseases ([Fig. 1]).
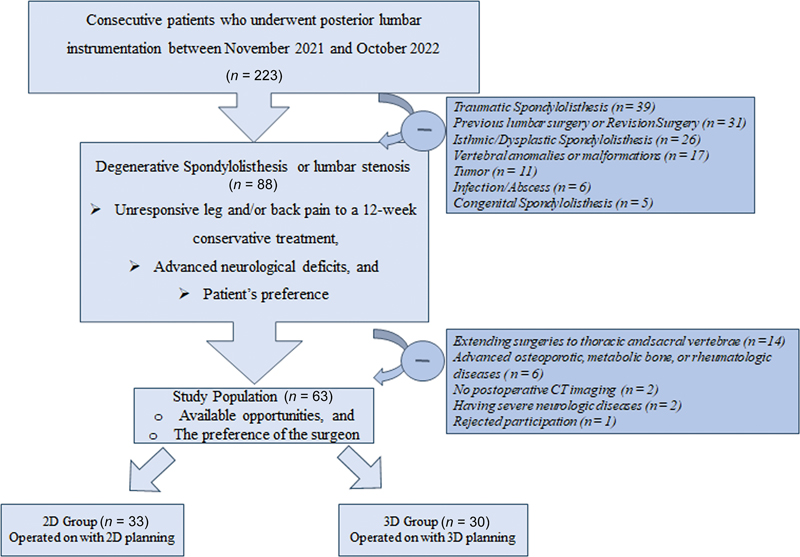
Patients were divided into two groups: 2D preoperative planning group (2DG) and 3D preoperative planning group (3DG). Preoperative 3D planning was dependent on availability of opportunities and surgeon preference. Both groups were evaluated for demographic and clinical characteristics, upper facet joint violation, pedicle breach, and blood transfusion.
Radiological Evaluation
To emphasize the diagnosis, preoperative dynamic, lateral, and standing anteroposterior (AP) radiographs—sagittal and axial T1- and T2-weighted short-tau inversion recovery and T2-weighted fast spin echo MRI were obtained from all the patients. To evaluate the possibility of osteoporosis, bone mineral densitometry T-score was obtained preoperatively using dual-energy X-ray absorptiometry in all the patients. The densitometric measurements were taken at the femoral neck and L1–L4, L1, L2, L3, and L4 in an AP projection using iDXA, a high-performance compact equipment of the General Electric.[14] [15] All the patients underwent preoperative and postoperative lumbar CT scans with 0.625-mm-thick slices.
For the 3DG, preoperative thinly sliced CT scans were used for the evaluation of bone structure, degenerative changes, and 3D reconstruction for preoperative planning. The obtained data were rendered with 3D Slicer, version 4.10.2 (Surgical Planning Laboratory, Harvard University, Boston, Massachusetts, United States). The mesh mixer program (version 3.5.474; Autodesk, Inc., San Rafael, California, United States) was used for preoperative planning by appropriately placing the screw, rod, and interconnections on the 3D spine. For the 2DG, the preoperative planning was done using only thinly sliced CT scans.
The classification system of Babu et al[16] and Gertzbein and Robbins[17] was used to evaluate the radiological outcomes by assessing pedicle breach and upper facet violation using the measurements on postoperative thinly sliced CT scans. Facet joint violation was graded as follows: grade 0, screw not in the facet joint and did not violate the facet joint; grade 1, screw in the lateral facet but not in the articular facet; grade 2, screw penetrated the facet joint ≤1 mm; grade 3, screw advanced within the facet joint surface. Breach was classified as follows: grade A, no breach; grade B, breach < 2 mm; Grades C and D, breach < 4 and 6 mm, respectively; Grade E, breach > 6 mm.
Surgical Procedures
Two surgeons (H.D. and A.O.M.) performed all the surgeries. According to their preoperative clinical symptoms and preoperative MRI, the patients underwent lumbar laminectomy, placement of the TPSs, and transforaminal lumbar interbody fusion (TLIF) via the classic open posterior approach. Indications for TLIF include multiple disk herniation, spinal canal stenosis (<5 mm), lateral recess stenosis (<2 mm), tropism, and/or bilaterally impaired facet joints.[12] [14] [15]
Two-dimensional Preoperative Planning Group
2D preoperative planning with lumbar CT was performed. Under general anesthesia, the patient was placed in a prone position at the operation table. C-arm fluoroscopy was used to determine the operating level. A classic midline incision was made. After subperiosteal stripping of the muscles, the posterior elements were exposed so that the beginning of the transverse process was visible. The intersection of the vertical line passing through the outer lateral edge of the facet and the horizontal line passing through the middle of the transverse process, that is, the standard entry point (SEP), was determined and confirmed by C-arm fluoroscopy. The entry point was trimmed using a rongeur. A control probe was used to control the four walls of the entry. According to the pedicle dimensions, an appropriate-sized TPS was placed with the planned angles regarding the preoperative CT scans. Finally, the TPS positioning was confirmed by AP and lateral fluoroscopy.
Three-dimensional Preoperative Planning Group
Preoperative planning was done by determining the SEP on 3D images ([Figs. 2A] and [3A]). In cases where the SEP was not suitable, a different entry point and angle were used ([Figs. 2B–D] and [3B–D]). This information and images were stored for use in surgery. Under general anesthesia, the patient was placed in a prone position at the operation table. The C-arm fluoroscopy was used to determine the operating level. A classic midline incision was made. After subperiosteal stripping of the muscles, the posterior elements were exposed so that the beginning of the transverse process was visible. The entry point was determined using the images previously obtained in 3D reconstruction ([Fig. 4]) and trimmed using a rongeur. According to the pedicle dimensions, an appropriate-sized TPS was placed using the preplanned angles. Finally, the TPS positioning was confirmed by AP and lateral fluoroscopy.



Clinical and Functional Outcomes
To assess the clinical and functional outcomes, the Oswestry Disability Index (ODI) and visual analog scale (VAS) scores for low back pain and leg pain were utilized at different time points (preoperatively; postoperative day 1, week 3, months 3 and 12, and last visit).
Statistical Analysis
Data analyses were performed using the Number Cruncher Statistical System 2007 (Kaysville, Utah, United States) program. Descriptive statistics were given as mean ± standard deviation, median, frequency, percentage, and ranges. The conformity of the quantitative data to normal distribution was tested using the Shapiro–Wilk test and graphical methods. The Mann–Whitney U test was used to compare the quantitative variables without normal distribution between the two groups. Pearson's chi-square test, Fisher's exact test, and Fisher–Freeman–Halton exact test were used to compare the qualitative data. To compare the pre- and postoperative functional improvement and pain intensity evaluation in the same patients, paired samples t-test was used. A p-value <0.05 was considered statistically significant. All tests were two-tailed. For categorical data, p-values were given with a hazard ratio (HR) or relative/risk ratio (RR) along with the corresponding 95% confidence intervals. For normally distributed data, Pearson's correlation analysis was used to evaluate the correlations between the variables (inserted screws into the upper lumbar vertebrae) and scales (pedicle breach and upper facet joint violation). For this purpose, we considered L1 and L2 as upper lumbar vertebrae.[12]
Results
A total of 63 patients (24 males and 39 females) who met the study criteria were operated on consecutively during the study period. In the 2DG, 156 TPSs were placed in 33 patients. In the 3DG, 144 TPSs were placed in 30 patients. The mean age of the studied sample was 57.9 ± 12.1 years (range: 49.5–87 years). The demographic and clinical characteristics are given in [Table 1]. Between-group comparisons regarding sex, age, body mass index, duration of surgery and radiation exposure, and amount of blood transfusion showed no statistically significant differences (p > 0.05; [Table 2]). The mean pre- and postoperative ODI scores were 62.4 ± 7.5 (range: 52–76) and 18.8 ± 4.8 (range: 8–26), respectively (p < 0.0001; t = 35.3). The average preoperative VAS scores were 8.1 ± 1.2 (range: 3–9) for back pain and 7.8 ± 1.3 (range: 3–9) for leg pain, and the average postoperative VAS scores at the last follow-up visit were 2.1 ± 0.4 (range: 0–4) for back pain and 1.8 ± 0.3 (range: 0–3) for leg pain (p < 0.0001; t = 37.65 and p < 0.0001; t = 35.7, respectively). Between-group comparisons regarding postoperative patient satisfaction, clinical outcomes, and functional improvements showed there were no statistically significant differences (p > 0.05; [Table 2]). No significant difference was found between the surgeons' outcomes (p > 0.05).
|
Variable |
N (%) |
Mean ± SD |
Median (range) |
|---|---|---|---|
|
Number of the patients |
63 (100.0%) |
– |
– |
|
Sex (M/F) |
24/39 (38.1%) |
– |
– |
|
Age (y) |
– |
57.9 ± 12.1 |
57 (30–87) |
|
BMI (kg/m2) |
– |
26.7 ± 2.5 |
26.9 (21–34) |
|
Symptoms' duration (mo) |
– |
68.3 ± 169.8 |
78 (12–360) |
|
Presenting symptoms |
|||
|
• Leg pain |
63 (100.0%) |
– |
– |
|
• Low back pain |
52 (82.5%) |
– |
– |
|
• Impairment of sensation |
43 (68.3%) |
– |
– |
|
• Weakness |
29 (46.0%) |
– |
– |
|
• Neuropathic pain |
17 (27.0%) |
– |
– |
|
• Sphincter dysfunction[a] |
6 (9.5%) |
– |
– |
|
Clinical findings |
|||
|
• Sensation deficits (+) |
45 (71.4%) |
– |
– |
|
• Motor deficits (+) |
30 (47.6%) |
– |
– |
|
• Gait difficulties |
16 (25.4%) |
– |
– |
|
• Sphincter dysfunction |
6 (9.5%) |
– |
– |
|
• Atrophy |
4 (6.3%) |
– |
– |
|
• No findings |
16 (25.4%) |
– |
– |
|
Duration of anesthesia (min) |
– |
181.8 ± 29.2 |
174.5 (75–283) |
|
Duration of surgery (min) |
– |
154.5 ± 22.6 |
148.5 (60–248) |
|
Duration of radiation exposure (s) |
– |
18.4 ± 5.4 |
18 (12–36) |
|
Mean LOS (d) |
– |
1.6 ± 1.1 |
2.5 (1–7) |
|
Mean IP blood loss (mL) |
– |
390.3 ± 138.8 |
405 (180–1500) |
|
Operated segments and levels (87 segments) |
|||
|
• Single segment (i.e., two vertebrae) |
47 pts (74.6%) |
– |
– |
|
• Two segments (i.e., three vertebrae) |
10 pts (15.9%) |
– |
– |
|
• Three segments (i.e., four vertebrae) |
4 pts (6.3%) |
– |
– |
|
• Four segments (i.e., five vertebrae) |
2 pts (3.2%) |
– |
– |
Abbreviations: BMI, body mass index; IP, intraoperative; LOS, length of postoperative hospitalization; pts: patients; SD, standard deviation.
a Some of these patients presented with urge incontinence.
|
Variable |
2DG |
3DG |
Statistics |
|---|---|---|---|
|
Number of the patients |
33 (52.4%) |
30 (47.6%) |
– |
|
Sex (M/F) |
23/10 (67.7%) |
16/14 (53.3%) |
p = 0.18; χ 2 = 1.78[a] |
|
Age (y) |
58.3 ± 12.7 [58; 50–79] |
57.3 ± 11.6 [55.5; 49.5–87] |
p = 0.75; t = 0.325[b] |
|
BMI (kg/m2) |
26.6 ± 2.8 [26.5; 21–34] |
26.9 ± 2.2 [27.0; 23–31.2] |
p = 0.58; t = 0.47[b] |
|
T-score |
–1.6 ± 0.7 [–1.5; –2.2 to –0.4] |
–1.8 ± 0.6 [–1.6; –2.3 to –0.6] |
p = 0.23; t = 1.21[b] |
|
Duration of anesthesia (min) |
178.4 ± 24.8 [165.5; 75–265] |
184.7 ± 34.2 [190; 110–285] |
p = 0.40; t = 0.843[b] |
|
Duration of surgery (min) |
151.2 ± 18.4 [145; 60–220] |
157.9 ± 27.2 [154; 82–248] |
p = 0.25; t = 1.15[b] |
|
Duration of radiation exposure (s) |
18.2 ± 4.3 [17; 12–36] |
18.6 ± 5.3 [18; 12–36] |
p = 0.74; t = 0.33[b] |
|
Mean LOS (d) |
1.4 ± 1.1 [2.5; 1–7] |
1.8 ± 1.0 [2; 1–5] |
p = 0.14; t = 1.505[b] |
|
Mean IP blood loss (mL) |
370 ± 128.4 [380; 180–900] |
410 ± 155.2 [405; 280–1500] |
p = 0.27; Z = - 1.11[c] |
|
Amount of blood transfusion (mL)[d] |
630 ± 232.4 [450; 450–900] |
630 ± 314.6 [450; 450–1350] |
p = 0.85; Z = - 0.16[c] |
|
Preoperative ODI |
63.2 ± 7.9 [61; 52–76] |
61.6 ± 7.2 [62; 54–74] |
p = 0.41; t = 0.837[b] |
|
Postoperative last-visit ODI |
19.6 ± 4.9 [20; 8–26] |
18.2 ± 3.7 [18; 10–24] |
p = 0.21; t = 1.27[b] |
|
Preoperative back VAS |
8.2 ± 1.3 [6.5; 3–9] |
7.9 ± 1.0 [7; 4–8] |
p = 0.31; t = 1.02[b] |
|
Postoperative last-visit back VAS |
2.2 ± 0.3 [2.5; 2–4] |
2.1 ± 0.6 [2; 0–4] |
p = 0.4; t = 0.848[b] |
|
Preoperative leg VAS |
7.9 ± 1.4 [6; 3–9] |
7.6 ± 1.0 [5; 4–8] |
p = 0.34; t = 0.97[b] |
|
Postoperative last-visit leg VAS |
1.9 ± 0.4 [2.5; 0–3] |
1.8 ± 0.3 [2; 0–3] |
p = 0.27; t = 1.11[b] |
Abbreviations: 2DG, group of patients who were operated on with 2D planning; 3DG, group of patients who were operated on with 3D planning; BMI, body mass index; IP, intraoperative; LOS, the length of postoperative hospitalization; ODI, Oswestry disability index; VAS, visual analog scale.
Note: In the table, the values are given as mean ± standard deviation [median; range].
a Pearson's chi-squared test.
b Unpaired t-test.
c Mann–Whitney U test.
d Only 10 patients in each group received blood transfusion; therefore, the comparison was only between these patients.
Although lesser pedicle breach was detected in the 3DG than in the 2DG and the accuracy of TPS positioning was 94.2 and 96.5% in the 2DG and 3DG, respectively; the differences were significant (p = 0.42; HR = 1.6 [0.57–4.84] and p = 0.42; RR = 0.98 [0.93–1.03]) retrospectively ([Table 3]). However, upper facet joint violation was significantly less common in the 3DG. The rate of upper facet joint violation was 12.8% (n = 20) in the 2DG versus 3.5% (n = 5) in the 3DG (p = 0.006; χ 2 = 8.57; [Table 4]). The screws inserted into the upper lumbar vertebrae (L1 and L2) were associated with pedicle breach (p = 0.0001; RR = 0.12 [0.05–0.33]; r = −0.28) and upper facet joint violation (p < 0.0001; RR = 0.13 [0.06–0.26]; r = −0.36).
|
Pedicle breach |
2DG (n = 156) |
3DG (n = 144) |
Statistics |
||
|---|---|---|---|---|---|
|
Total screws |
9 (5.8%) |
5 (3.5%) |
p = 0.345; χ 2 = 0.89[a] |
||
|
Grade A (no breach) |
HD (85/88) |
AOM (62/68) |
HD (94/96) |
AOM (45/48) |
For 2DG: p = 0.18; OR = 0.37 (0.09–1.52)[b] For 3DG: p = 0.32; OR = 0.32 (0.05–1.98)[b] |
|
L1 |
1 |
3 |
4 |
1 |
For 2DG: p = 0.31; OR = 0.23 (0.03–2.31)[b] For 3DG: p = 0.67; OR = 1.96 (0.21–18.0)[b] |
|
L2 |
7 |
6 |
7 |
5 |
For 2DG: p = 0.77; OR = 0.84 (0.27–2.63)[b] For 3DG: p = 0.52; OR = 0.64 (0.21–2.15)[b] |
|
L3 |
21 |
10 |
20 |
8 |
For 2DG: p = 0.23; OR = 1.71 (0.74–3.94)[b] For 3DG: p = 0.66; OR = 1.25 (0.5–3.11)[b] |
|
L4 |
34 |
24 |
38 |
16 |
For 2DG: p = 1.0; OR = 1.06 (0.54–2.06)[b] For 3DG: p = 0.71; OR = 1.23 (0.59–2.57)[b] |
|
L5 |
22 |
19 |
25 |
15 |
For 2DG: p = 0.58; OR = 0.79 (0.38–1.63)[b] For 3DG: p = 0.43; OR = 0.72 (0.34–1.57)[b] |
|
Grade B (<2 mm) |
8 (88.9%) |
5 (100%) |
p = 0.58; HR = 1.49 (0.5–4.44)[b] |
||
|
L1 |
1 |
0 |
0 |
1 |
For 2DG: p = 0.4; OR = ∞[b] For 3DG: p = 0.33; OR = ∞[b] |
|
L2 |
1 |
2 |
1 |
1 |
For 2DG: p = 1.0; OR = 0.43 (0.03–5.99)[b] For 3DG: p = 1.0; OR = 0.71 (0.04–14.35)[b] |
|
L3 |
1 |
0 |
0 |
0 |
For both groups: p = 1. 0; OR = ∞[b] |
|
L4 |
0 |
0 |
0 |
0 |
For both groups: p = 1. 0; OR = ∞[b] |
|
L5 |
0 |
3 |
1 |
1 |
For 2DG: p = 0.23; OR = ∞[b] For 3DG: p = 1.0; OR = 0.6 (0.04–10.35)[b] |
|
Grade C (2 to <4 mm) |
1 (11.1%) |
0 |
p = 1.0; HR = ∞ [b] |
||
|
L1[c] |
0 |
1 |
0 |
0 |
For 2DG: p = 1.0; OR = ∞[b] For 3DG: p = 0.43; OR = 0.72 (0.34–1.57)[b] |
Abbreviations: 2DG, group of patients who were operated on with 2D planning; 3DG, group of patients who were operated on with 3D planning; HD and AOM are the neurosurgeons who attended all surgeries; HR, hazard ratio; N, number of screws; OR, odds ratio.
a Pearson's chi-squared test.
b Fisher's exact test. HR/OR values were given with the corresponding 95% confidence intervals.
c There were no other screws.
|
Upper facet violation |
2DG (n = 156) |
3DG (n = 144) |
Statistics |
||
|---|---|---|---|---|---|
|
Total screws |
20 (12.8%) |
5 (3.5%) |
|||
|
No violation |
HD (81/88) |
AOM (55/68) |
HD (94/96) |
AOM (45/48) |
For 2DG: p = 0.053; OR = 0.37 (0.14–0.98)[c] For 3DG: p = 0.33; OR = 0.32 (0.05–1.98)[c] |
|
L1 |
0 |
2 |
4 |
1 |
For 2DG: p = 0.47; OR = ∞[c] For 3DG: p = 0.33; OR = ∞[c] |
|
L2 |
6 |
3 |
6 |
6 |
For 2DG: p = 0.31; OR = 0.2 (0.02–1.71)[c] For 3DG: p = 0.47; OR = ∞[c] |
|
L3 |
21 |
8 |
20 |
7 |
For 2DG: p = 0.22; OR = 0.19 (0.02–2.4)[c] For 3DG: p = 0.29; OR = ∞[c] |
|
L4 |
34 |
24 |
38 |
16 |
For 2DG: p = 1.0; OR = ∞[c] For 3DG: p = 1.0; OR = ∞[c] |
|
L5 |
20 |
18 |
26 |
15 |
For 2DG: p = 0.66; OR = 0.48 (0.07–2.76)[c] For 3DG: p = 0.38; OR = ∞[c] |
|
Grade 1 |
10 (50%) |
3 (60%) |
p = 0.085; HR = 3.24 (0.91–11.54)[b] |
||
|
L1 |
1 |
0 |
0 |
0 |
For 2DG: p = 0.33; OR = ∞[c] For 3DG: p = 1.0; OR = ∞[c] |
|
L2 |
0 |
2 |
1 |
0 |
For both groups: p = 1. 0; OR = ∞[c] |
|
L3 |
1 |
2 |
0 |
1 |
For 2DG: p = 0.22; OR = 0.2 (0.02–2.4)[c] For 3DG: p = 0.29; OR = ∞[c] |
|
L4 |
0 |
0 |
0 |
0 |
For both groups: p = 1.0; OR = ∞[c] |
|
L5 |
1 |
3 |
0 |
1 |
For 2DG: p = 0.61; OR = 0.3 (0.03–3.15)[c] For 3DG: p = 0.38; OR = ∞[c] |
|
Grade 2 |
8 (40%) |
2 (40%) |
p = 0.10; HR = 3.92 (0.85–18.12)[b] |
||
|
L1 |
1 |
1 |
0 |
1 |
For 2DG: p = 1.0; OR = ∞ [c] For 3DG: p = 0.33; OR = ∞[c] |
|
L2 |
2 |
2 |
1 |
0 |
For 2DG: p = 1.0; OR = 0.5 (0.05–5.51)[c] For 3DG: p = 1.0; OR = ∞[c] |
|
L3 |
0 |
0 |
0 |
0 |
For both groups: p = 1.0; OR = ∞[c] |
|
L4 |
0 |
0 |
0 |
0 |
For both groups: p = 1.0; OR = ∞[c] |
|
L5 |
1 |
1 |
0 |
0 |
For 2DG: p = 1.0; OR = 0.9 (0.05–15.47)[c] For 3DG: p = 1.0; OR = ∞[c] |
|
Grade 3 |
2 (10%) |
0 |
p = 0.25; HR = ∞[b] |
||
|
L1[d] |
0 |
1 |
0 |
0 |
For both groups: p = 1.0; OR = ∞[c] |
|
L2[d] |
0 |
1 |
0 |
0 |
For 2DG: p = 0.4; OR = ∞[c] For 3DG: p = 1.0; OR = ∞[c] |
Abbreviations: 2DG, group of patients who were operated on with 2D planning; 3DG, group of patients who were operated on with 3D planning; HD and AOM are the neurosurgeons who attended all surgeries; HR, hazard ratio; N, number of screws; OR, odds ratio.
a Statistically significant at p < 0.05.
b Pearson's chi-squared test.
c Fisher's exact test. HR/OR values were given with the corresponding 95% confidence intervals.
d There were no other screws.
In the 3DG, the SEP was found to be optimal in 112 of the 144 screws; the entry point was found to be nonoptimal in 32 screws, and a different entry point was determined using 3D planning. A statistically significant difference was found between the accuracy rate of TPS positioning where the classic SEPs were used and the accuracy rate of TPS positing where different entry points were determined by 3D planning (p < 0.0001; χ 2 = 24.7). The modification rate was higher at L1, L2, and L5 (p < 0.0001; RR = 0.64 [0.55–0.75]; [Table 5]). No significant complications such as deep infection, neurologic deficit, or revision surgery for misplaced screws were recorded.
|
Vertebra (N; %) |
TPSs with suitable SEPs |
Changed entry points utilizing 3D[*] |
Distance between SEPs and changed entry points (mm)[**] and scroll direction |
Statistics |
|---|---|---|---|---|
|
Total (144; 100%) |
112 (77.8%) |
32 (22.2%) |
1.4 ± 0.4 [1.8; 1–3.5]; caudal/ lateral |
– |
|
L1 (6; 4.2%) |
2 (33.3%) |
4 (66.7%) |
2.5 ± 0.4 [2.0; 2–3]; caudal |
|
|
L2 (14; 9.7%) |
8 (57.1%) |
6 (42.9%) |
2.5 ± 0.3 [2.5; 2–3.5]; caudal |
|
|
L3 (28; 19.4%) |
22 (78.6%) |
6 (21.4%) |
1.5 ± 0.3 [1.7; 1–3]; caudal |
|
|
L4 (54; 37.5%) |
54 (100%) |
0 |
0 |
|
|
L5 (42; 29.2%) |
26 (61.9%) |
16 (38.1%) |
2 ± 0.4 [2.5; 2–2.5]; lateral |
Abbreviations: N, number of screws; TPSs, transpedicular screws; SEP, standard entry point; 3D, three-dimension; 3DG, group of patients who were operated on with three-dimensional planning.
a Fisher exact test. RR-values were given with the corresponding 95% CIs.
* SEP was found to be non-optimal in 32 screws and a different entry point was determined using 3D planning.
** The values are given as mean ± standard deviation [median; range].
*** p < 0.05 statistically significant.
Discussion
Posterior fixation with TPSs is a common procedure in spinal surgery. Planning before stabilization surgery with TPSs is based on radiological examinations such as X-ray, CT, and MRI.[18] The use of neuronavigation systems for spinal fixation with TPSs is still debated due to the high economic cost and long duration of surgery.[18] [19] Recently, lumbar fixation surgeries with TPSs have been performed using the freehand technique accompanied by preoperative 3D CT modeling.[8] [9] [10] [11] [18] [19] Several studies showed that preoperative 3D planning can minimize surgical complications related to anatomical variations.[8] [9] [10] [11] [18] [19] Our results demonstrated that such planning helps achieve more accurate TPS placement with less upper facet violation and lower pedicle breach rates. In our patients, the incidence of pedicle breach and facet violation was higher in the upper lumbar regions. This was also the region where the entry point was modified the most using 3D planning. We believe this to be a major advantage of 3D planning.
Ever since Radermacher et al[20] introduced 3D planning in spinal fusion surgeries in 1998, several authors have tried utilizing the same technique due to its high accuracy. However, creating 3D-printed templates is laborious and time-consuming.[18] [19] [21] A recent study by Chaudhary et al[9] used preoperative 3D planning in 25 pediatric patients with craniovertebral anomalies. The authors observed that more anatomical details can be obtained with 3D planning than with 2D evaluation. According to them, open-source software, such as Horos, can be advantageous when accessing systems related to image planning is difficult or expensive. In the present study, pedicle breach was lower and the accuracy of TPS positioning was higher in the 3DG; however, the differences did not reach significant levels.
Ozaki et al[10] retrospectively reviewed their 28 patients who received 3D planning for spinal fixation with TPSs. They observed that screw misplacement rate was lower in the 3D planning group than in those treated with classical techniques. In their retrospective study, Penner et al[11] reported that 328 screws were placed successfully with preoperative 3D planning in 82 patients. They claimed that preoperative 3D planning had the same accuracy as navigation systems in determining the pedicle entry point and direction.[11] In this study, preoperative 3D planning resulted in more accurate TPS placement and less radiation exposure. However, the duration of surgery was shorter in the 2DG but the difference was not statistically significant.
In spinal instrumentation surgeries, preserving the upper facet joint is very important to avoid lumbar adjacent segment disease (LASD).[22] Anatomical disruption, upper facet joint violation, discal degeneration, and changes in intradiscal pressure, although unproven, are assumed to be the risk factors for LASD.[22] [23] Archavlis et al[8] reported a lower upper facet violation rate in patients who received 3D preoperative planning. Our results were in-line with the literature.
In 2D planning, the determination of the entry point and angle is done separately in axial and sagittal sequences. However, in 3D planning, axial–sagittal shifting can be done simultaneously, the pedicle entry point can be moved laterally and inferiorly, the medial and sagittal angles can be increased, and adjustments can be made according to the pedicle and upper facet position. In this study, we first tested the SEP in 3D planning. The SEP was not optimal in some vertebral segments. For example, in terms of pedicle breach, it was thought that it would be appropriate to shift the entry points of 16 TPSs from 2 to 2.5 mm laterally in the axial plane from the SEP in the L5 vertebra. Otherwise, there was risk of breach in the medial pedicle surface away from the midpedicle trajectory. However, the lateral shift in the upper vertebrae during 3D planning required a high degree of medial angulation. Therefore, it was believed that shifting the entry point caudally might be safer and more practical. Upper facet violation was avoided by moving the entry point 2 to 3 mm caudal in four screws at L1 and 2 to 3.5 mm in six screws at L2 and by making more cranial angulation on sagittal plane angulation. Similar results have been reported in previously published studies.[9] [10] [11]
Preoperative 3D planning can help especially in the cases where intraoperative fluoroscopy images cannot be obtained in relation to anatomical variation, advanced degeneration, obesity, etc.[5] Moreover, we believe that preoperative 3D planning can help spine surgery trainees and new spine surgeons to minimize TPS positioning-related complications. 3D planning is better for the surgeon to conceptualize the anatomy more accurately than conventional planning, and the pedicle accuracy rate has been improved by revealing the angular differences between the right and left pedicle in many patients.[2] Therefore, in this study, we tried to homogenize the groups and recruited patients with degenerative lumbar spinal diseases who generally have an unusual anatomy.
The retrospective nature of the study, single-center experience, and a relatively small sample size (n = 63) are the limitations of this study. Fluoroscopy was used by different radiological technicians; therefore, we believe that between-group comparison regarding the duration of radiation exposure had a statistical bias. Recruiting patients from the same geographical area is another major limitation of the study. Studies conducted by different surgeons in different centers may provide more reliable outcomes. We believe that this subject needs to be investigated in a larger anatomical study.
Conclusion
For patients with degenerative lumbar diseases, 3D preoperative planning decreased the rate of upper facet joint violation. However, there was no significant difference in pedicle breach in 3D and 2D preoperative planning. The incidence of pedicle breach and facet violation was higher in the upper lumbar levels. This was also the region where the entry point was modified the most. We believe that this is the major advantage of utilizing 3D planning. The freehand technique can be modified with 3D modeling to eliminate the disadvantages such as low accuracy, without negatively affecting its features like practicality, low cost, and short operation time. We believe that preoperative 3D planning will be useful for spine surgery trainers and new spine surgeons as well as it can reduce the revision rates.
Conflict of Interest
None declared.
Ethical Approval
This comparative retrospective study was approved on November 8, 2022, under decision number: E-22686390-050.99-21531, by the medical ethics committee of Atlas University in Istanbul, Turkey.
This study was undertaken at the Department of Neurosurgery, Atlas University—Medicine Hospital.
Informed Consent
Informed consent was obtained from all the participants included in this study.
* Hüseyin Doğu and Anas Abdallah contributed equally to this work and both authors deserve the first name.
** N. Mehmet Elmadağ is a senior coauthor of this study.
-
References
- 1 Lopez CD, Boddapati V, Lee NJ. et al. Three-dimensional printing for preoperative planning and pedicle screw placement in adult spinal deformity: a systematic review. Global Spine J 2021; 11 (06) 936-949
- 2 Dogu H, Ozturk O, Can H. Does three-dimensional preoperative planning improve accuracy of pedicle screw insertion?. Cesk Slov Neurol N 2022; 85: 228-234
- 3 Gautschi OP, Schatlo B, Schaller K, Tessitore E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management: a literature review of 35,630 pedicle screws. Neurosurg Focus 2011; 31 (04) E8
- 4 Matur AV, Palmisciano P, Duah HO, Chilakapati SS, Cheng JS, Adogwa O. Robotic and navigated pedicle screws are safer and more accurate than fluoroscopic freehand screws: a systematic review and meta-analysis. Spine J 2023; 23 (02) 197-208
- 5 Yoshii T, Hirai T, Yamada T. et al. Lumbosacral pedicle screw placement using a fluoroscopic pedicle axis view and a cannulated tapping device. J Orthop Surg Res 2015; 10: 79
- 6 Li HM, Zhang RJ, Shen CL. Accuracy of pedicle screw placement and clinical outcomes of robot-assisted technique versus conventional freehand technique in spine surgery from nine randomized controlled trials: a meta-analysis. Spine 2020; 45 (02) E111-E119
- 7 Perdomo-Pantoja A, Ishida W, Zygourakis C. et al. Accuracy of current techniques for placement of pedicle screws in the spine: a comprehensive systematic review and meta-analysis of 51,161 screws. World Neurosurg 2019; 126: 664-678.e3
- 8 Archavlis E, Ringel F, Kantelhardt S. Maintenance of integrity of upper facet joints during simulated percutaneous pedicle screw insertion using 2D versus 3D planning. J Neurol Surg A Cent Eur Neurosurg 2019; 80 (04) 269-276
- 9 Chaudhary K, Dhawale A, Shah A, Nene A. The technique of using three-dimensional and multiplanar reformatted computed tomography for preoperative planning in pediatric craniovertebral anomalies. N Am Spine Soc J 2021; 7: 100073
- 10 Ozaki T, Yamada K, Nakamura H. Usefulness of preoperative planning by three-dimensional planning software for pedicle screw placement in thoracolumbar surgeries: misplacement rate and associated risk factors . Spine Surg Relat Res 2021; 6 (03) 279-287
- 11 Penner F, Marengo N, Ajello M. et al. Preoperative 3D CT planning for cortical bone trajectory screws: a retrospective radiological cohort study. World Neurosurg 2019; 126: e1468-e1474
- 12 Abdallah A, Emel E, Güler Abdallah B. Factors associated with the recurrence of lumbar disk herniation: biomechanical-radiological and demographic factors. Neurol Res 2022; 44 (09) 830-846
- 13 Abdallah A, Emel E, Abdallah BG, Asiltürk M, Sofuoğlu ÖE. Factors affecting the surgical outcomes of tethered cord syndrome in adults: a retrospective study. Neurosurg Rev 2018; 41 (01) 229-239
- 14 Yeşiltaş S, Abdallah A, Uysal Ö, Yilmaz S, Çinar İ, Karaaslan K. The efficacy of intraoperative freehand erector spinae plane block in lumbar spondylolisthesis: a randomized controlled study. Spine 2021; 46 (17) E902-E910
- 15 Abdallah A, Güler Abdallah B. Factors associated with the recurrence of lumbar disk herniation: non-biomechanical-radiological and intraoperative factors. Neurol Res 2023; 45 (01) 11-27
- 16 Babu R, Park JG, Mehta AI. et al. Comparison of superior-level facet joint violations during open and percutaneous pedicle screw placement. Neurosurgery 2012; 71 (05) 962-970
- 17 Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo. Spine 1990; 15 (01) 11-14
- 18 O'Leary R, Sullivan TB, Bartley CE. et al. How often does the preoperative plan for freehand pedicle screw placement match the actual surgical execution in adolescent idiopathic scoliosis?. Childs Nerv Syst 2022; 38 (10) 1923-1927
- 19 Rawicki N, Dowdell JE, Sandhu HS. Current state of navigation in spine surgery. Ann Transl Med 2021; 9 (01) 85
- 20 Radermacher K, Portheine F, Anton M. et al. Computer assisted orthopaedic surgery with image based individual templates. Clin Orthop Relat Res 1998; (354) 28-38
- 21 Wilcox B, Mobbs RJ, Wu AM, Phan K. Systematic review of 3D printing in spinal surgery: the current state of play. J Spine Surg 2017; 3 (03) 433-443
- 22 Min JH, Jang JS, Lee SH. Comparison of anterior- and posterior-approach instrumented lumbar interbody fusion for spondylolisthesis. J Neurosurg Spine 2007; 7 (01) 21-26
- 23 Radcliff KE, Kepler CK, Jakoi A. et al. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J 2013; 13 (10) 1339-1349
Address for correspondence
Publication History
Received: 22 April 2023
Accepted: 11 September 2023
Accepted Manuscript online:
13 September 2023
Article published online:
19 December 2023
© 2023. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Lopez CD, Boddapati V, Lee NJ. et al. Three-dimensional printing for preoperative planning and pedicle screw placement in adult spinal deformity: a systematic review. Global Spine J 2021; 11 (06) 936-949
- 2 Dogu H, Ozturk O, Can H. Does three-dimensional preoperative planning improve accuracy of pedicle screw insertion?. Cesk Slov Neurol N 2022; 85: 228-234
- 3 Gautschi OP, Schatlo B, Schaller K, Tessitore E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management: a literature review of 35,630 pedicle screws. Neurosurg Focus 2011; 31 (04) E8
- 4 Matur AV, Palmisciano P, Duah HO, Chilakapati SS, Cheng JS, Adogwa O. Robotic and navigated pedicle screws are safer and more accurate than fluoroscopic freehand screws: a systematic review and meta-analysis. Spine J 2023; 23 (02) 197-208
- 5 Yoshii T, Hirai T, Yamada T. et al. Lumbosacral pedicle screw placement using a fluoroscopic pedicle axis view and a cannulated tapping device. J Orthop Surg Res 2015; 10: 79
- 6 Li HM, Zhang RJ, Shen CL. Accuracy of pedicle screw placement and clinical outcomes of robot-assisted technique versus conventional freehand technique in spine surgery from nine randomized controlled trials: a meta-analysis. Spine 2020; 45 (02) E111-E119
- 7 Perdomo-Pantoja A, Ishida W, Zygourakis C. et al. Accuracy of current techniques for placement of pedicle screws in the spine: a comprehensive systematic review and meta-analysis of 51,161 screws. World Neurosurg 2019; 126: 664-678.e3
- 8 Archavlis E, Ringel F, Kantelhardt S. Maintenance of integrity of upper facet joints during simulated percutaneous pedicle screw insertion using 2D versus 3D planning. J Neurol Surg A Cent Eur Neurosurg 2019; 80 (04) 269-276
- 9 Chaudhary K, Dhawale A, Shah A, Nene A. The technique of using three-dimensional and multiplanar reformatted computed tomography for preoperative planning in pediatric craniovertebral anomalies. N Am Spine Soc J 2021; 7: 100073
- 10 Ozaki T, Yamada K, Nakamura H. Usefulness of preoperative planning by three-dimensional planning software for pedicle screw placement in thoracolumbar surgeries: misplacement rate and associated risk factors . Spine Surg Relat Res 2021; 6 (03) 279-287
- 11 Penner F, Marengo N, Ajello M. et al. Preoperative 3D CT planning for cortical bone trajectory screws: a retrospective radiological cohort study. World Neurosurg 2019; 126: e1468-e1474
- 12 Abdallah A, Emel E, Güler Abdallah B. Factors associated with the recurrence of lumbar disk herniation: biomechanical-radiological and demographic factors. Neurol Res 2022; 44 (09) 830-846
- 13 Abdallah A, Emel E, Abdallah BG, Asiltürk M, Sofuoğlu ÖE. Factors affecting the surgical outcomes of tethered cord syndrome in adults: a retrospective study. Neurosurg Rev 2018; 41 (01) 229-239
- 14 Yeşiltaş S, Abdallah A, Uysal Ö, Yilmaz S, Çinar İ, Karaaslan K. The efficacy of intraoperative freehand erector spinae plane block in lumbar spondylolisthesis: a randomized controlled study. Spine 2021; 46 (17) E902-E910
- 15 Abdallah A, Güler Abdallah B. Factors associated with the recurrence of lumbar disk herniation: non-biomechanical-radiological and intraoperative factors. Neurol Res 2023; 45 (01) 11-27
- 16 Babu R, Park JG, Mehta AI. et al. Comparison of superior-level facet joint violations during open and percutaneous pedicle screw placement. Neurosurgery 2012; 71 (05) 962-970
- 17 Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo. Spine 1990; 15 (01) 11-14
- 18 O'Leary R, Sullivan TB, Bartley CE. et al. How often does the preoperative plan for freehand pedicle screw placement match the actual surgical execution in adolescent idiopathic scoliosis?. Childs Nerv Syst 2022; 38 (10) 1923-1927
- 19 Rawicki N, Dowdell JE, Sandhu HS. Current state of navigation in spine surgery. Ann Transl Med 2021; 9 (01) 85
- 20 Radermacher K, Portheine F, Anton M. et al. Computer assisted orthopaedic surgery with image based individual templates. Clin Orthop Relat Res 1998; (354) 28-38
- 21 Wilcox B, Mobbs RJ, Wu AM, Phan K. Systematic review of 3D printing in spinal surgery: the current state of play. J Spine Surg 2017; 3 (03) 433-443
- 22 Min JH, Jang JS, Lee SH. Comparison of anterior- and posterior-approach instrumented lumbar interbody fusion for spondylolisthesis. J Neurosurg Spine 2007; 7 (01) 21-26
- 23 Radcliff KE, Kepler CK, Jakoi A. et al. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J 2013; 13 (10) 1339-1349