

Subscribe to RSS
DOI: 10.1055/a-2179-4729
Follicular Unit Excision (FUE) Basics
Authors

Abstract
Follicular unit excision (FUE) has risen to the forefront as the world's most popular hair transplant procedure. However, most writing on this subject has catered to the advanced practitioner. The goal of this article will be to focus on safe planning and decision making along with key technical steps that will guide the beginner surgeon to harvest a graft safely and to harvest the donor area in a uniform way to avoid overharvesting. Topics covered in this article also include instrumentation and decision making between FUE versus linear strip excision.
Keywords
follicular unit excision (FUE) - basics - hybrid punch - oscillating - overharvesting - linear strip excision (LSE)Follicular unit excision (FUE) has become the most popular hair transplant procedure in the world eclipsing linear strip excision (LSE) surgery over the past decade.[1] There have been ongoing advances technologically since 2017 with the introduction of devices with oscillating, hybrid punches (which will be discussed) that have revolutionized FUE[2] by making harvesting far easier and graft quality and survival on par now with LSE procedures.[3] [4] The dark side of the rise of FUE is that it has led to a glut of practitioners who hire technicians to do the harvesting who are often ill trained and in many cases illegal to perform the procedure, which has led to clinical disasters, the worst of which observed is overharvested and decimated donor hair. In tandem with this trend toward nonphysician FUE harvesting has been salespeople who sell the patient a procedure who should never have a procedure because they are too young, too unstable, too advanced in their hair loss, or have compromised donor hair. To perform proper hair surgery requires the prerequisite knowledge to understand the nature and progression of hair loss and how to select safe candidates along with how to counsel patients on appropriate medical therapy to retard and partially reverse the hair loss process. This monograph will be unable to cover this topic in detail but will introduce broad strokes to the subject to help a beginning physician understand some fundamental concepts that will help guide them to further research and inquiry.
Supply and Demand
First and foremost, when I evaluate a prospective patient, I determine their supply and demand.[5] The supply refers to the donor supply of hair usable for current and future transplantation, and the demand refers to the current and projected future hair loss. The problem is that even though I may have sufficient current supply to fix current demand, the supply continues to dwindle due to either removing supply during a transplant and/or progression of hair loss that may encroach on the donor area that was thought initially to be wider and larger than it actually becomes in the future. Similarly, the area of hair loss (demand) may seem limited but with time that area expands and may become an issue where there is insufficient supply to fix it. In short, the supply continues to diminish over time and the demand continues to rise over time. The goal is to predict (always conservatively) that there will be sufficient future supply to fix future demand. That is why during a consultation the first thing I do is to look at the donor area to evaluate what I have to work with as well as the current state of hair loss and to look for signs of future problems, for example, areas of miniaturization or retrograde hair loss (hair loss coming up from the nape of the neck). Obviously, the age of the male patient is also a vital piece of information with ongoing safety every decade older the patient is. The crown is the area of greatest concern for me as far as planning hair restoration because what seemed to be a small area of transplant turns into a much larger area over time that may be hard to camouflage due to the expansion of crown balding. When a crown expands, there is a concurrent increase of demand and also loss of supply, especially concerning FUE since the donor area is much wider than in LSE cases. Of course, medical therapy for hair loss, for example, finasteride and minoxidil, help to retard the advances of hair loss but obviously not entirely so and should not be exclusively relied on as a means to arrest hair loss since they will not.
Deciding between LSE versus FUE
As mentioned, FUE has become the dominant, preferred method for hair transplant surgery today. That being said, I truly believe that FUE is not the right procedure for everyone ([Fig. 1]). As they say, if all you have is a hammer, the world is a nail. There are many problems with FUE that must be considered when evaluating a patient for possible hair surgery. First, the standard way of performing FUE is through shaving the back of the head to afford an easier, straightforward method of harvesting. Although, a nonshaven technique can be employed it can be far more cumbersome and labor intensive not to mention more difficult for the patient to tolerate given the longer times needed to harvest hair. Accordingly, all women and those men with longer hairstyles oftentimes have no benefit with FUE, as superior LSE surgery should leave behind a very hard to detect scar, despite online marketing to the contrary, in experienced surgical hands. Further, FUE must per force go beyond the traditional area of what Unger et al defined as the safe donor area (SDA),[6] which means the hairs that are genetically programmed to be resistant to the effects of dihydrotestosterone (DHT)-mediated hair loss. Therefore, these wider areas of harvesting that must be performed with FUE (which is mandatory in order to avoid overharvesting from taking grafts from too narrow a geographic area) is riskier, especially in younger patients, as the expansion of the crown could eventually cause not only graft loss but also exposure of punctate hypopigmented scars from the harvested area as the crown continues to expand. Anything but the smallest FUE cases (< 250 grafts) require a relatively wider harvesting area with that area progressively wider as the graft count becomes larger during an operative case, for example, a 2,000-graft case or a 3,000-graft case. Accordingly, I think LSE is also the ideal method of approaching a man with more advanced baldness of a Norwood 6 and 7 for the aforementioned reasons but also for another reason. Not only is the SDA much more restricted in these cases causing the risk of exposing scars and losing grafts over time but also because the donor field is geographically smaller, the risk of overharvesting becomes proportionally much greater with FUE, which will be discussed next.

Overharvesting
Unfortunately, I see an overharvested, moth-eaten donor area several times a month from inexperienced practitioners dabbling with FUE. It is one of the most serious complications that I have observed with FUE and now I see it all the time walking through my door. Unlike a horrible linear donor scar that arises from LSE that usually can be easily corrected with grafts placed into it or at least be covered by longer hair, an overharvested, decimated donor area following FUE has limited options to correct or camouflage this devastating outcome. Besides simple inexperience, I think the other problem today that is causing patients to suffer this complication is the online boasting of high harvesting numbers like marketing touting “4,000 grafts,” “5,000 grafts,” etc., which I think in most patients they may not even have in their lifetime let alone in a single, standalone session of FUE. Yes, individuals with high density may be able to have these many grafts harvested but certainly I would hesitate to offer a patient that very high number during a single session, especially if they are younger and would require more surgeries in the future in order to preserve usable donor hair for future sessions given the nature of ongoing increase in hair loss demand and simultaneous reduction of donor supply. Techniques that will be more specifically outlined in this article will hopefully help the reader avoid overharvesting, something that I keep foremost in my mind during every harvest that I perform and during every moment that I am engaged in harvesting.
Ergonomics
A quick aside here on ergonomics before we begin a more in-depth discussion on FUE technique, which is the core of this article.[7] Unfortunately, FUE harvesting is much more demanding on a surgeon's physical condition than LSE harvesting. Accordingly, it is paramount that the surgeon be in top form to perform FUE harvesting, which I liken to being like an athlete. An athlete prepares before the event, performs during the event, and recuperates after the event in preparation for the next event. A surgeon should try to be physically fit, exercising regularly both weights and cardio, try not to drink excessively or at all, eat right (for the most part), get good sleep, and try not to be overweight, all of which can have an impact on surgical performance.[8] During the surgery, I recommend a relaxed posture and hand movements, which may need constant reminding when you are just beginning and feeling undue tension and frustration during the harvesting process. Frequent, scheduled breaks can also help with mini stretching exercises interrupting the surgery as needed. After surgery, it is important to recuperate with good body therapies including chiropractic and massage, both of which I engage in every week with scheduled appointments along with daily stretching after my workouts. An ounce of prevention is worth a pound of cure before chronic finger, neck, and back pains creep up on you and become hard to shake and that may throw your career off course.
Instrumentation
As mentioned in the introduction, the advent of newer devices in 2017 to 2018 has radically changed the field of FUE harvesting. Prior to this time, two major schools existed: the blunt punch camp espoused by Jim Harris[9] [10] and the sharp punch camp promulgated by John Cole.[11] The blunt punch touted much lower transection rates (especially in less skilled hands) but suffered from buried grafts and grafts that did not appear as clean as the sharply punched grafts. The sharp punch method celebrated a higher-quality graft but was much more sensitive to transection, especially in newer surgical hands. Then came the hybrid punch devices[12] of Jean Devroye[13] [14] called the WAW and of Roberto Trivellini[15] called by his namesake, both machines that I own and use (no financial affiliations myself). The so-called “hybrid” element defines this punch as having both blunt and sharp features ([Fig. 2]). The shape resembles a trumpet with the inside facing the graft being blunt to minimize risk of transection and the outer edge being sharp to sharply dissect the graft. In addition, the old blunt and sharp devices entered the skin through pure, high-speed rotation, whereas these devices use a gentle oscillating arc so that the torsional injury experienced with older methods are not encountered with these devices. In short, these devices offer much lower transection rates even in relatively less skilled hands and much higher graft quality, which translates into better survival and healthier, more natural-looking graft results. Even at the time of this publication, there are so many new models of these devices that recounting all of the newer features would not only lie beyond the scope of this article but also be outdated by the time you read this page. Instead, this article is meant to introduce you to the fundamental attributes of these kinds of state-of-the-art devices to stimulate your research and adoption of these excellent instruments to find what works best in your budget and your hands.

Technique
Preparation
In preparation for the procedure, the patient is asked to have a “high and tight” hairstyle a few days before the surgery. The recipient area where recipient sites will be made need not be shaved all the way down. In fact, I prefer to have some length in that area so that I can read how the hairs appear to guide me on where areas of miniaturization are observed and where areas of baldness are more apparent so that I can better create recipient sites that fit the observed balding pattern. When the patient enters the operatory, the back of the head is further shaved down with a zero guard to leave only 1 to 2 mm of hair shaft emanating from the skin surface so as to facilitate easy graft harvesting. With patients of African descent with very curly hair, it is critical that this hair shaft be particularly short because it is harder to cannulate these hairs and also the hair curl may make reading the correct hair angle more difficult (which will be explained more in-depth below).
Marking
The first marking I undertake is to outline the hairline for the patient initially using an eyebrow pencil until the patient and I agree as to its shape and position, which I then reinforce with a permanent marker. I then outline the entire planned recipient area and then show the patient to make sure that we are both in agreement. At this point, I plan out the donor area and mark it out in preparation for FUE harvesting.
For the donor area, I first start to mark out the top line of the harvest looking at the upper limit of what I would consider the SDA. I then start to look at the bottom line of the harvest and begin to mark that out. If there is no sign of retrograde hair loss (hair loss coming up from the nape of the neck), I may draw a bottom line that is quite low going into the nape of the neck so that I can harvest these grafts being careful not to go so low as to risk exposure of these harvest sites if retrograde loss should occur over time. I then mark the midline from top to bottom connecting the top to the bottom line. I use the ruler to mark from the midline to the outer lateral limit and then use that distance to guide me to make the same distance on the contralateral side ([Fig. 3A]). I then finish squaring off the entire perimeter of my planned harvest area. I will then divide the donor area into relatively equidistant squares of 3 to 4 cm each ([Fig. 3B, C]). I use these squares to plan my harvest so that I harvest the entire planned area in a uniform manner and can pace and plan my harvest, which will be explained next.

Unlike in LSE cases where I harvest the strip first and give my staff the strip to start dissection, which I then use to calculate a projected number, I will create recipient sites first for FUE and from that number I will plan how to harvest the donor area. For example, if I make 2,000 recipient sites and I have marked out 20 grids, then I will need to divide those 2,000 planned grafts into the 20 grids. Dividing 2,000 grafts by 20 grids, that would equal 100 grafts per grid. If I see the central 12 grids are higher density and the outer 8 grids are lower density, then I may adjust my harvesting plan. For example, I may project that I would be able to harvest 125 grafts per grid for the central 12 grids, then that would yield me 1,500 grafts (by multiplying 125 by 12). The difference then would be 500 grafts left for the remaining 8 grids by subtracting 1,500 grafts from 2,000 grafts. Note that 500 divided by 8 would yield 62.5 grafts per grid, which could be rounded up to 65 grafts, for example. Accordingly, my plan would be to harvest roughly 125 grafts for the central 12 grids and 65 grafts for the outer 8 grids. As I progress with the actual harvesting of each grid, I will ask my staff to tell me the ongoing yield so that I can keep track of my numbers. My staff is trained to call out “130 in grid 3 and total so far is 300.” That way I can track my progress and not overharvest any one grid or any one side. When you are under high magnification, these grids are so critical to ensure that you are keeping pace over the geographic expanse and also not extending beyond the marked areas into areas outside of the SDA.
Anesthesia
I have a Joint Commission-accredited facility and use some level of intravenous pain control for patients consisting of meperidine (Demerol) and promethazine (Phenergan), and if you have an accredited facility I would highly recommend doing likewise.[16] Intravenous pain management can offer many advantages including minimal discomfort during anesthesia delivery, virtual elimination of anxiety, patient compliance during every phase of surgery especially during harvesting, retrograde amnesia of their experience, and a perceived foreshortening of the time that they experience that they were in surgery. Because the patient is prone during the harvesting phase that will last many hours, deeper levels of sedation that I use during LSE procedures, specifically using intravenous midazolam (Versed) and fentanyl, are unwise due to potential airway compromise. For those practitioners who are unable to deliver intravenous pain management, then oral sedation with possible nitrous gas anxiolysis can be supportive to more meticulous and slow delivery of the anesthetic to make the experience for the patient as pleasant as possible. In addition, two types of oral sedatives that I have heard work well (but have not tried since I do not need to do so) are a combination of oral midazolam, ketamine, and odansetron, known more popularly by its trade name MKO Melt (ImprimisRx, Carlsbad, CA) and a sufentanil sublingual product made by AcelRx Pharmaceuticals Inc (Hayward, CA).
For the recipient area, I perform nerve blocks that include the supraorbital and auriculotemporal blocks along with a zygomaticotemporal block as needed in order to ensure the longevity of the anesthetic effect. The frontal half of the anesthesia is reinforced with an anterior ring block. Both the nerve blocks and the anterior ring block are undertaken first with 1% lidocaine with 1:100,000 epinephrine followed by 0.25% bupivacaine with 1:200,000 epinephrine after recipient-site creation and before FUE harvesting begins. The FUE donor area must be anesthetized with dilute lidocaine/bupivacaine block in a field block technique since a ring block and nerve block will not sufficiently work. Similarly, a field block with concentrated 1% lidocaine with 1:100,000 epinephrine and/or 0.25% bupivacaine with 1:200,000 epinephrine will be both highly toxic and paradoxically not be as durable as a dilute field block. [Table 1] outlines how to mix this dilute anesthetic to be used as the FUE donor field block.
In order to infiltrate this dilute anesthetic, I first start by injecting approximately 1 mL of concentrated 1% lidocaine with 1:100,000 epinephrine using a 30-gauge needle into the apices of the bottom edge of the grid to minimize feeling the entry of the larger needles used for infiltration of the tumescent field block ([Fig. 4]). I use 3 or 5 mL syringes outfitted with 25-gauge needles to infiltrate the field block because larger 10 mL syringes can cause undue finger strain. I start with instilling the anesthesia through those initial points that I anesthetized with the concentrated lidocaine ([Fig. 5A]). As the occipital nerves emanate from the bottom and arc upwards in the occipital region, anesthetizing the lowest portion of the grid usually begins the process of anesthetizing the entire donor area or at least minimizes discomfort as you progress upwards ([Fig. 5B]) and laterally ([Fig. 5C]), which is how I proceed when I anesthetize the donor for optimal patient comfort. This systematic approach provides the fastest delivery with the least pain for the patient to achieve long-lasting, durable results that should persist for the entire operative procedure ([Fig. 6]).



Once the area is anesthetized, the patient stays numb for the entire duration of the procedure. However, it is important to initially extend the anesthetic field block a little beyond the planned grid for optimal anesthesia and I will also often feather a few harvest sites just beyond the marked grids. In addition, when I approach each grid, I will add a little more tumescent field block using 3 to 5 mL into the grid that I am about to harvest in order to further optimize hemostasis and improve tissue turgor. I am not entirely convinced tissue turgor is critical for harvesting and some experts argue grafts need to be more freely mobile to minimize transection. I simply have the habit of instilling a little extra dilute anesthesia before I start each grid and find it helpful.
Harvesting
There are two components of harvesting that I think the beginner surgeon must grasp. The first is how to harvest a graft with minimal transection, and the second is how to progress the harvest over the donor area to perform a uniform harvest that resists the problem of overharvesting. We will discuss each of these components in depth.
To harvest a graft with healthy surrounding perifollicular tissue and no transection and to do so consistently require both visualizing the graft well and also feeling the proper graft release. To visualize the graft well starts with adequate magnification. I have used 2.5 × , 4.5 × , and now 8.5× magnifying loupes and will unequivocally say that the 8.5× loupes significantly reduces eyestrain and allows me to see subtle variations in hair exit angles that I simply could not appreciate with lower levels of magnification ([Fig. 7]). I use the Surgitel brand (General Scientific Corporation, Ann Arbor, MI) outfitted with a bright xenon light source. I also use two overhead directional lights that help me see the area for extracting the incised grafts and to see the pattern that I am creating with my harvesting to look for any missed sites or uneven harvesting. Also, my assistant who is extracting the grafts that I have incised relies on these directional overhead lights as well. When approaching a follicular unit, it is important that the punch is squarely centered on the follicle. Second, you should look for the blush of color under the skin which represents the continuation of the hair follicle under the skin ([Fig. 8]). You need to align the punch with this angle not the angle above the skin since the angle above the skin represents the hair curl. If you align it with the hair curl above the skin, you will transect the follicle below the skin ([Fig. 9]). This hair curl is even more extreme and confusing when dealing with patients of African descent so trimming the hair even shorter will be very helpful. To help visualize the hair exit angle I find it easier for me to sit squarely above the patient (superior to his head) and also higher looking somewhat downward ([Fig. 10]). If I feel that I cannot visualize the exit angle well or if I am encountering more consecutive transections, then I will adjust my head side to side or move my stool up or down (or the patient's head position) until I can see the exit angle and resume quality harvesting.




The second component of quality harvesting is feeling for transection and feeling for proper graft release. This is the harder of the two components that requires a longer learning curve but that must be mastered. Initially, you will be very frustrated and feel as if you will never master it but one day you simply will. You will begin to feel the release and know even before you check if the graft has been released or transected by extracting it whether you have succeeded or not. I can feel when I have not gone deep enough and I can oftentimes feel transection as well. The punch must go deep enough to release the arrector pili muscle and all dermal attachments but not so deep that the bulbs are mangled/hooked or to engender a greater degree of transection. You will begin to feel this release in pressure where there is a slight give in the tissue. That release in pressure should signal the end of your depth of punch penetration. If you stop short of this release, you will have either “capping” where you rip off the epidermal cap and leave the rest of the graft behind due to insufficient graft release or you will have a “stripped graft” with little quality supporting perifollicular tissue that could lead to poor graft growth if transplanted. Transection, however, feels a lot like the release of the dermal attachments but oftentimes is more abrupt and sooner than tissue release. Further, when the angle of approach is off, the tissue feels tough as you progress and then there is an abrupt release, which signifies most likely a transection. In contrast, when the graft is properly released (not transected), the punch glides through like butter and then there is a gentle release of the tissue. You will begin to be able to feel this difference as you progress in your learning. However, I am not always 100% right. That is why constant verbal callouts from your assistant who is extracting grafts behind your incisions will give you much-needed feedback. My assistant will call out “1 T out of 3” or “2 good out of 3,” both meaning 1 transection out of 3 hairs in a particular 3-hair follicular unit or “stripped”/“need more tissue,” meaning I am not going deep enough, or alternatively “capped.” That is also why I start very slowly during my harvest to begin with and always extract my own grafts that I incise to start so that I can evaluate the grafts for quality, transections, and other problems. If there are any issues that come up, I will slow down and do my own extractions. Also, from the corner of my eye, I am looking at the graft my assistant is extracting and seeing the problems with my incisions without even him calling out to me my issues. Another critical component to feeling is to lighten your grip and to hold the instrument closer to the tip for better sensitivity. What is amazing is that if you do this, the instrument will oftentimes autocorrect minor alignment issues and miraculously move the punch in the exact direction needed to harvest the graft. I have to constantly remind myself to lighten my grip as I progress, especially if I begin to encounter any consecutive transections. Finally, the last visual feedback is that if a graft has been properly released, oftentimes you should see the graft pop up a millimeter above the surrounding skin. One tip with African hair is that the punch should enter in a curved arc to follow the upper trajectory of the curl just deep enough to feel the dermal/arrector pili release. At times, simply entering almost perpendicularly with minimal arcing of the punch will work better. This is technically very hard for a beginner, and I would recommend to stay only with straighter hair to start until you have mastered it.
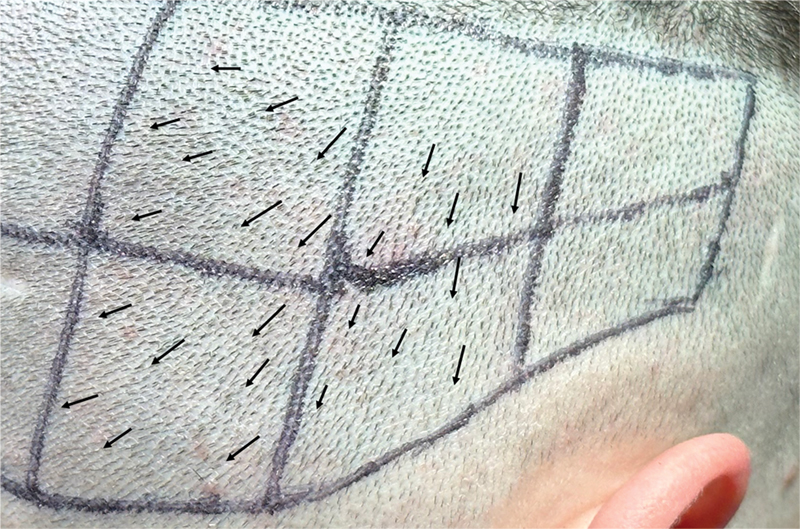
If you can successfully harvest a graft by look and feel, the next goal is to master progressing over a grid in a systematic way that will help minimize risk of overharvesting, speed up the harvesting process by avoiding skipping over areas or needing to adjust punch angles too often because you are skipping over wide areas (which will be further explained), and to ensure uniform graft numbers. I always start with the top grid (grid closest to me when I am sitting at the head of the patient) immediately to the right of midline. I start on the left side of each grid because my assistant who is sitting to my left can extract the grafts that I have incised as I move progressively away from him farther to the right over a grid. As alluded to earlier, it is important not to skip around, which wastes time, because hairs gradually change direction ([Fig. 11]), so staying in one small region of a 3 × 3 cm grid will allow your punch to remain relatively in the same angle as you proceed all the while taking very careful inspection to see how a graft angle slowly changes so that you can make minor adjustments as you march forward. I will harvest the top grid and move down the grids (moving away from me toward the patient's nape of the neck), then complete all major grids on the right side, followed by the major grids on the left side moving from top grid just off midline on the left and moving laterally in a mirror image to the way that I progressed on the right side. I finish with completing the lateral grids with lower density on the left side and then wrap up by returning to the remaining lateral (lower density) grids on the right side.
When I evaluate the next graft that I am going to incise I think to myself will a graft above it (that is, closer to me and anatomically superior to the graft I am planning to harvest) be able to cover the hole that I leave behind ([Fig. 12]). You have to imagine the patient sitting up or standing and the hair immediately above extending over to cover the hole you just made to make sure that you do not see the hole. The second criterion I am thinking about as I harvest is whether I am simply leaving too large a gap behind. For example, if two adjacent follicular units are very widely spaced already, I would be hesitant to remove one of them to leave a much larger gap behind. This situation becomes particularly more problematic in patients who have already undergone at least one session of FUE because they already have gaps left behind where you must progress more slowly and more deliberately to avoid overharvesting. The third component that I think about is whether I am removing too many large grafts and only leaving small grafts behind (an unfortunate bias that all of us FUE surgeons have to take the best grafts for transplantation but that may render the donor area more quickly overdepleted). This is especially true when I am looking at an area and seeing a lot of finer grafts, then I would be particularly hesitant to take out the larger grafts in that area that may render the area overharvested. These are only some of the components in your decision making when planning the progress over the donor area that will require time and patience to master.

Conclusion
Unfortunately, this primer on FUE basics can only scratch the surface on technique for proper harvesting. Nevertheless, I am hopeful that by providing an overview of key elements to planning, anesthesia, and harvesting that the reader will do further exploration into these topics before going headlong into the delicate art of FUE hair surgery or any hair surgery for that matter. Frustration will give way to mastery and pain into joy as the art of hair surgery, and in this case FUE, will be a mountain that you will enjoy climbing in your career hopefully over and over again.
Conflict of Interest
None declared.
-
References
- 1 International Society of Hair Restoration Surgery: 2020 Practice Census Results.
- 2 Lam SM, Williams Jr KL. eds. Follicular Unit Excision (FUE). 2nd ed.. New Delhi, India: Jaypee Brothers Medical Publishers; 2022
- 3 Beehner M. FUE vs FUT-MD: study of 1,780 follicles in four patients. Hair Transplant Forum Int. 2016; 26 (04) 160-161
- 4 Josephitis D, Shapiro R. FUT vs. FUE graft survival: a side-by-side study of 3 patients undergoing a routine 2,000+ graft hair transplantation. Hair Transplant Forum Int. 2018; 28 (05) 179-182
- 5 Lam SM. Hair Transplant 101. St. Louis, MO: Quality Medical Publishing; 2023
- 6 Unger W, Solish N, Giguère D. et al. Delineating the “safe” donor area for hair transplanting. Am J Cosmet Surg 1994; 11: 239-243
- 7 Williams Jr KL, Arienzo JN. Ergonomics in FUE donor harvesting. In: Williams Jr KL, Lam SM. eds. Hair Transplant 360: Follicular Unit Excision (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022
- 8 Attia P, Gifford B. Outlive: The Science & Art of Longevity. Harmony; 2023
- 9 Harris JA. Follicular unit extraction: the SAFE system. Hair Transplant Forum Int. 2004; 14: 157 , 163, 164
- 10 Harris JA. New methodology and instrumentation for follicular unit extraction: lower follicle transection rates and expanded patient candidacy. Dermatol Surg 2006; 32 (01) 56-61 , discussion 61–62
- 11 Cole J. A strong proponent of FUE. Hair Transplant Forum Int. New York, NY. 2011; 21 (06) 193-194
- 12 Tykocinski A. Dealing with a hybrid trumpet punch. Hair Transplant Forum Int. 2017; 27 (01) 14-16
- 13 Devroye J. Motorized FUE with hybrid punch. In: Williams Jr KL, Lam SM. eds. Hair Transplant 360: Follicular Unit Excision (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022
- 14 Devroye J. Powered FU extraction with the short-arc-oscillation flat punch FUE system (SFFS). Hair Transplant Forum Int. 2016; 26 (04) 129-136
- 15 Trivellini R. The Trivellini system and technique. Hair Transplant Forum Int. 2018; 28 (05) 188-190
- 16 Lam SM. Anesthesia principles and techniques for FUE. In: Lam SM, Williams Jr KL. eds. Hair Transplant 360: Follicular Unit Extraction (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022
Address for correspondence
Publication History
Accepted Manuscript online:
21 September 2023
Article published online:
30 October 2023
© 2023. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 International Society of Hair Restoration Surgery: 2020 Practice Census Results.
- 2 Lam SM, Williams Jr KL. eds. Follicular Unit Excision (FUE). 2nd ed.. New Delhi, India: Jaypee Brothers Medical Publishers; 2022
- 3 Beehner M. FUE vs FUT-MD: study of 1,780 follicles in four patients. Hair Transplant Forum Int. 2016; 26 (04) 160-161
- 4 Josephitis D, Shapiro R. FUT vs. FUE graft survival: a side-by-side study of 3 patients undergoing a routine 2,000+ graft hair transplantation. Hair Transplant Forum Int. 2018; 28 (05) 179-182
- 5 Lam SM. Hair Transplant 101. St. Louis, MO: Quality Medical Publishing; 2023
- 6 Unger W, Solish N, Giguère D. et al. Delineating the “safe” donor area for hair transplanting. Am J Cosmet Surg 1994; 11: 239-243
- 7 Williams Jr KL, Arienzo JN. Ergonomics in FUE donor harvesting. In: Williams Jr KL, Lam SM. eds. Hair Transplant 360: Follicular Unit Excision (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022
- 8 Attia P, Gifford B. Outlive: The Science & Art of Longevity. Harmony; 2023
- 9 Harris JA. Follicular unit extraction: the SAFE system. Hair Transplant Forum Int. 2004; 14: 157 , 163, 164
- 10 Harris JA. New methodology and instrumentation for follicular unit extraction: lower follicle transection rates and expanded patient candidacy. Dermatol Surg 2006; 32 (01) 56-61 , discussion 61–62
- 11 Cole J. A strong proponent of FUE. Hair Transplant Forum Int. New York, NY. 2011; 21 (06) 193-194
- 12 Tykocinski A. Dealing with a hybrid trumpet punch. Hair Transplant Forum Int. 2017; 27 (01) 14-16
- 13 Devroye J. Motorized FUE with hybrid punch. In: Williams Jr KL, Lam SM. eds. Hair Transplant 360: Follicular Unit Excision (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022
- 14 Devroye J. Powered FU extraction with the short-arc-oscillation flat punch FUE system (SFFS). Hair Transplant Forum Int. 2016; 26 (04) 129-136
- 15 Trivellini R. The Trivellini system and technique. Hair Transplant Forum Int. 2018; 28 (05) 188-190
- 16 Lam SM. Anesthesia principles and techniques for FUE. In: Lam SM, Williams Jr KL. eds. Hair Transplant 360: Follicular Unit Extraction (FUE). Vol. 4. 2nd ed.. New Delhi: Jaypee Brothers Medical Publishers; 2022