Key words
ultrasound - muscular - tendons - bones - ultrasound-color doppler
Introduction
Ultrasound (US) has become an established part of the diagnosis of acute sports injuries
due to its broad availability and cost-effectiveness and the systematic further development
of mobile ultrasound devices. It is typically used as the primary or focused examination
modality (point-of-care US, “POCUS”). In individual cases it can be used in addition
to other modalities (primarily magnetic resonance imaging [MRI]). US is used not only
in the daily clinical routine but also directly as mobile US in training centers and
training camps. As shown by the current example of pediatric fracture care, US is
becoming increasingly established in clinical guidelines further highlighting its
value [1]. In sports medicine US is primarily used in the acute initial diagnostic assessment
or in the intensive follow-up of muscle and tendon injuries (multiple examinations
in short time intervals after injury, e. g. 2–3 times per week or during weight bearing),
while newer specialized ultrasound applications like shear wave elastography and highly
sensitive Doppler methods (microvascular imaging) are used primarily in high-performance
sports. However, due to the limited number of available studies, there are only a
few use recommendations [2]. The implementation of US in musculoskeletal imaging, if suitable for diagnosis,
can contribute to better utilization of MRI capacities (elimination of Doppler examinations)
and significant cost savings in the healthcare system. [3]
This article provides an overview of the usual areas of application, frequently asked
questions regarding ultrasound in elite sports, and the value of mobile ultrasound
devices in sports traumatology.
Diagnostic assessment of muscle injuries
Diagnostic assessment of muscle injuries
Regardless of the modality, imaging methods in addition to clinical examination are
an essential part of the diagnosis of muscle injuries. On the one hand, the suspected
clinical diagnosis can be confirmed and on the other hand the exact extent of the
injury can be evaluated [4]. Based on these parameters, an optimal treatment decision and determination of the
prognosis regarding a return to competition (RTC) can be made [5].
Although MRI is considered the gold standard in the diagnosis of muscle injuries (regarding
the extent of a structural defect or the evaluation of non-structural lesions), US
provides fast and reliable initial diagnosis and optimized determination of the further
procedure [6]
[7]
[8]. Since US is usually more readily available than MRI, it is particularly suitable
for initial diagnosis as well as for repeated follow-up examinations ([Fig. 1]) in popular and elite sports to ensure close monitoring of training or to identify
complications early [8]. In particular, the anterior thigh and the musculature of the lower leg – compared
to the ischiocrural group – can be diagnosed with good sound quality due to the low
penetration depth.
 Fig. 1 Structural muscle injury (defect zone: 10 mm) in the rectus femoris muscle of a soccer
player. In the initial diagnostic assessment (A), the hypoechoic zone of rupture (star) can be clearly defined and is surrounded
by a clear hyperechoic zone of perilesional edema. A direct comparison to the healthy
opposite side (right half of the image) can be performed here. Over the course of
7 days (B), the margins become increasingly blurry (star) and the hypoechoic zone of rupture
becomes slightly smaller as a result of healing of the muscle while the surrounding
edema remains clearly visible. After 17 days (C) only slight edema with inhomogeneous muscle fibers is still visible and the muscle
still appears swollen. After 25 days, the structural defect and the zone of edema
are no longer visible (D).
Fig. 1 Structural muscle injury (defect zone: 10 mm) in the rectus femoris muscle of a soccer
player. In the initial diagnostic assessment (A), the hypoechoic zone of rupture (star) can be clearly defined and is surrounded
by a clear hyperechoic zone of perilesional edema. A direct comparison to the healthy
opposite side (right half of the image) can be performed here. Over the course of
7 days (B), the margins become increasingly blurry (star) and the hypoechoic zone of rupture
becomes slightly smaller as a result of healing of the muscle while the surrounding
edema remains clearly visible. After 17 days (C) only slight edema with inhomogeneous muscle fibers is still visible and the muscle
still appears swollen. After 25 days, the structural defect and the zone of edema
are no longer visible (D).
Close monitoring ensures the ability to plan early surgical measures or infiltration,
e. g., when healing of the tendon is limited by a persistent hematoma. Calcification
of a hematoma (in terms of post-traumatic myositis ossificans) can be definitively
verified as a possible complication on ultrasound based on the calcified structure
and corresponding dorsal acoustic shadowing. This makes expanded X-ray examination
unnecessary ([Fig. 2]). Consequently, muscle imaging (particularly in popular sports) is primarily performed
using US in many countries due to a lack of MRI capacity.
 Fig. 2 Soccer player with tear in the left biceps femoris (caput breve). In the initial
diagnostic assessment, the central hematoma and the ruptured fibers can be effectively
visualized. For precise evaluation of the extent of the injury, a supplementary MRI
examination is often performed in elite sports (A). After 3 days, extensive aspiration of the hematoma (B, left half of the image) is performed, thereby resulting in a significantly smaller
size of the defect after 14 days (B, right half of the image). In the short-term follow-up, calcification of the hematoma
with dorsal acoustic shadowing is visible 3 weeks after trauma (C, arrows). This increasingly disappears in the following 2 weeks due to targeted therapy
and the acoustic shadowing is no longer present on US (D, arrows).
Fig. 2 Soccer player with tear in the left biceps femoris (caput breve). In the initial
diagnostic assessment, the central hematoma and the ruptured fibers can be effectively
visualized. For precise evaluation of the extent of the injury, a supplementary MRI
examination is often performed in elite sports (A). After 3 days, extensive aspiration of the hematoma (B, left half of the image) is performed, thereby resulting in a significantly smaller
size of the defect after 14 days (B, right half of the image). In the short-term follow-up, calcification of the hematoma
with dorsal acoustic shadowing is visible 3 weeks after trauma (C, arrows). This increasingly disappears in the following 2 weeks due to targeted therapy
and the acoustic shadowing is no longer present on US (D, arrows).
Muscle injuries are categorized as direct (= extrinsic) and indirect (= intrinsic)
injuries according to the underlying pathomechanism [9]. Direct muscle trauma corresponding to muscle injury by an external force with resulting
contusion or laceration, is mainly caused by impact trauma (e. g. knee against thigh)
and is typically seen in Germany in contact sports like soccer, handball, and football/rugby.
This direct trauma often results in an intramuscular hemorrhage without actual tearing
of the fibers. The role of US is to locate and visualize the initial finding as the
baseline for follow-up. A correct patient history and an in-depth discussion of the
type of accident are absolutely necessary here. The injury grade is determined based
purely on clinical signs (mild, moderate, severe) corresponding to the loss of function
and the duration of the recovery phase [9]. Standardized examination with longitudinal and cross-sectional scans and acquisition
of panorama images should be used to ensure comparable follow-up examinations over
the long term ([Fig. 3]). In the case of mild contusion injuries, a focal inhomogeneous zone without a large
hematoma that typically regresses quickly can be seen. Severe contusions with a large
hematoma can have a different appearance depending on when the examination is performed.
Within the first 24 hours, hematomas can appear both hyperechogenic and hypoechogenic.
In the following days, hematomas tend to appear as hypoechoic fluid until they become
inhomogeneous after coagulation ([Fig. 3]). In addition, US offers the opportunity to quickly puncture intramuscular hematomas
under US guidance to reduce pain and the RTC time. In addition, puncture of the hematoma
makes it possible to better evaluate whether the muscle fibers are injured.
 Fig. 3 Young soccer player with impact trauma (knee against thigh) and muscle contusion
in the left vastus intermedius muscle. In the early phase, an inhomogeneous (“cloudy”)
defect zone with swelling in the muscle is visible (A), which becomes clearly demarcated and increases in size after 10 days (B). In the case of organized areas, aspiration was not performed (finding not compressible),
and the defect zone is significantly smaller after 28 days and is only still visible
as a small area of swelling (C). The area was imaged for the last time after about 6 weeks to check for complete
healing (D).
Fig. 3 Young soccer player with impact trauma (knee against thigh) and muscle contusion
in the left vastus intermedius muscle. In the early phase, an inhomogeneous (“cloudy”)
defect zone with swelling in the muscle is visible (A), which becomes clearly demarcated and increases in size after 10 days (B). In the case of organized areas, aspiration was not performed (finding not compressible),
and the defect zone is significantly smaller after 28 days and is only still visible
as a small area of swelling (C). The area was imaged for the last time after about 6 weeks to check for complete
healing (D).
Ruptures of muscle fibers are considered indirect muscle trauma. The underlying mechanism
is a pathological (over-) extension of the muscle fibers (typically during eccentric
contraction), which exceeds the viscoelastic boundaries of the tissue consequently
resulting in an injury. US is primarily suitable for the detection of structural muscle
injuries. It is inferior to MRI with respect to determining the extent of an injury
and characterizing the injury, especially in the case of small and non-structural
muscle injuries [10]. Since muscle injuries of the lower extremities often occur at the myotendinous
junction, the evaluation of tendon segments is relevant for the further prognosis.
Optimal evaluation of the myotendinous junction is difficult on US but can be used
in addition to MRI during interventions and short-term follow-up.
One limitation of non-contrast-enhanced US is the detection and evaluation of non-structural
muscle injuries (corresponding to grades 1–2 of the classification according to the
Munich Consensus Conference) [11]. Thus, Hotfiel et al. showed that conventional B-mode US showed discrepancies with
respect to MRI in minor muscle injuries in a significant number of cases [12]
[13]. However, in minor injuries, ultrasound functions as an effective gatekeeper: It
can be used to rule out a structural muscle injury (differentiation between grade
2 and 3 lesions) [11]. In the case of discrepancies on US (clear symptoms with functional impairment but
negative US result), MRI examination is helpful due to the higher sensitivity [14]. Even if imaging allows a basic estimation of the recovery time, the literature
shows that imaging markers do not provide better prognostic evaluation compared to
clinical parameters in the case of hamstring injuries. [15]
[16]
Contrast-enhanced ultrasound (CEUS) which is now also used in the musculoskeletal
region has shown in the first studies better detection than non-contrast-enhanced
B-mode ultrasound for the diagnosis of non-structural muscle injuries. Perfusion in
the areas of edema can be visualized based on the reduced and delayed contrast enhancement
([Fig. 4]) [12]
[13]. Therefore, in special cases, additional use of CEUS is helpful, particularly for
precise short-term monitoring of injury-controlled training or targeted weight bearing.
 Fig. 4 Edematous swelling without a structural lesion in the rectus femoris muscle after
multiple injuries in the past. CEUS shows a significant reduction in blood flow (A) and delayed and reduced contrast enhancement in the measurement via time-intensity
curve (B). The violet ROI represents perfusion in the area with edema, and the blue ROI indicates
normal perfusion in the reference muscle (vasus intermedius muscle). After 3 days,
only partial edema in the muscle is still visible (C).
Fig. 4 Edematous swelling without a structural lesion in the rectus femoris muscle after
multiple injuries in the past. CEUS shows a significant reduction in blood flow (A) and delayed and reduced contrast enhancement in the measurement via time-intensity
curve (B). The violet ROI represents perfusion in the area with edema, and the blue ROI indicates
normal perfusion in the reference muscle (vasus intermedius muscle). After 3 days,
only partial edema in the muscle is still visible (C).
Ligament tears and tendon injuries
Ligament tears and tendon injuries
The use of US for tendon injuries and ligament tears has been known and clinically
established for decades [2]. The advantages result from the dynamic examination, the high spatial resolution,
and the use of Doppler ultrasound (primarily in overuse injuries or tendinopathies).
The method is established particularly in superficial locations like the Achilles
tendon, patellar tendon, quadriceps tendon, and the ligaments of the knee joint ([Fig. 5]). The differentiation between a partial tear and complete tear can usually be achieved
here with high accuracy. The comparatively rarer (isolated or combined) injuries of
the aponeuroses of the lower leg region, often in the region of the medial gastrocnemius
and soleus muscle can be characterized optimally on ultrasound due to their superficial
position. There are new classifications for evaluating the extent of injury of gastrocnemius
aponeurosis and free gastrocnemius aponeurosis regarding the return-to-sport prognosis
([Fig. 6]) [17].
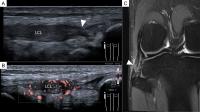 Fig. 5 Young soccer player injured during training with pain in the lateral knee joint.
Initial US examination shows the partial tear of the lateral collateral ligament with
significant swelling (grade II injury). Neither a complete tear nor a separating hematoma
is visible. The clear hypervascularization on highly sensitive Doppler imaging (B) confirms the diagnosis of a new partial tear. A follow-up MRI examination after
14 days showed still increased signal intensity with continuous ligament tissue fibers
(C). LCL: Lateral collateral ligament.
Fig. 5 Young soccer player injured during training with pain in the lateral knee joint.
Initial US examination shows the partial tear of the lateral collateral ligament with
significant swelling (grade II injury). Neither a complete tear nor a separating hematoma
is visible. The clear hypervascularization on highly sensitive Doppler imaging (B) confirms the diagnosis of a new partial tear. A follow-up MRI examination after
14 days showed still increased signal intensity with continuous ligament tissue fibers
(C). LCL: Lateral collateral ligament.
 Fig. 6 Combined rupture of the aponeurosis of the medial gastrocnemius muscle affecting
the muscle and the free aponeurosis with hemorrhage. US shows the exact location and
extent of the rupture zone in the gastrocnemius muscle (MG) within the complex structure
of this anatomical region (A longitudinal section, C cross-section). Corresponding comparison MRI images (B coronal, D axial). MS = soleus muscle.
Fig. 6 Combined rupture of the aponeurosis of the medial gastrocnemius muscle affecting
the muscle and the free aponeurosis with hemorrhage. US shows the exact location and
extent of the rupture zone in the gastrocnemius muscle (MG) within the complex structure
of this anatomical region (A longitudinal section, C cross-section). Corresponding comparison MRI images (B coronal, D axial). MS = soleus muscle.
US is now the method of choice for diagnosing tendinopathies, primarily jumper’s knee
and Achilles tendinitis. The use of multiparametric US (mpUS, [18]) with shear wave elastography (SWE) and new 3 D Doppler techniques for quantifying
neovascularization elevate US to a new level and ensure continuous improvement of
standardization and comparability ([Fig. 7]). The quantification of 3 D vascularization reduces the subjectivity of examinations
and improves diagnostic significance of follow-up examinations ([Fig. 7B, E]). With respect to Achilles tendinitis, lower stiffness values in combination with
neovascularization on Doppler ultrasound can be observed [19]
[20]. With respect to jumper’s knee, diagnostically significant studies on SWE are currently
lacking, while B-mode characteristics like thickening, loss of structure, ossification
together with neovascularization are established criteria and are sufficient for diagnosis.
It can be clinically observed in a growing number of cases that the patellar ligament
at the caudal patellar pole is increasingly stiff on elastography during follow-up
after therapy, indicating fibrosis of the tissue in our opinion ([Fig. 7C, F]).
 Fig. 7 Professional athlete (soccer) with jumper’s knee. MpUS with baseline examination
prior to the start of the season (A–C) and follow-up after the season (D–F) with over 40 mandatory games and three ACP treatments prior to the season. Neovascularization
is significantly reduced over the course of the season in spite of the high physical
strain during the season (A, B vs. D, E). This can be quantified by 3 D methods (ratio of color voxels to grayscale voxels).
SWE shows increased stiffness of the patella tip after the season both on the color-coded
map and in a metric analysis. The player became symptom-free over time.
Fig. 7 Professional athlete (soccer) with jumper’s knee. MpUS with baseline examination
prior to the start of the season (A–C) and follow-up after the season (D–F) with over 40 mandatory games and three ACP treatments prior to the season. Neovascularization
is significantly reduced over the course of the season in spite of the high physical
strain during the season (A, B vs. D, E). This can be quantified by 3 D methods (ratio of color voxels to grayscale voxels).
SWE shows increased stiffness of the patella tip after the season both on the color-coded
map and in a metric analysis. The player became symptom-free over time.
Interventional ultrasound
Interventional ultrasound
Interventional ultrasound is to be used both for acute muscle injuries and chronic
overuse injuries of the tendons. Intramuscular hematomas can usually be clearly defined
after 2 to 3 days based on the organization process (hypoechoic to anechoic) [8]. This is the optimal point in time for US-guided aspiration [21]. In structural muscle defects (rupture of muscle fibers), the surrounding hematoma
or the hematoma separating the tendon segments can be aspirated at this time and at
the same time locally effective injection therapies (platelet rich plasma [PRP], autologous-conditioned
plasma [ACP]) can be administered ([Fig. 8]). This intervention can achieve faster healing of the muscle tissue with improved
adaptation of the muscle fibers. In vitro studies show the regenerative potential
of PRP in acute soft-tissue injuries but there are only a few randomized controlled
studies showing a clear clinical benefit [22]. Thus, individual studies on PRP injection in muscle injuries show an imaging correlation
for faster healing and reduction of the time until a return to training (“time to
sports”) [23].
 Fig. 8 Combination of modalities and US-guided intervention. Partial tear at the myotendinous
junction of the biceps femoris (caput longum) of a soccer player (A). After aspiration of the hematoma, ACP was injected during the same intervention
directly into the injured fibers (B). The short-term follow-up US examination after 2 weeks shows proper healing without
hematoma. Precise evaluation of the tendon segment is difficult on US (C). The follow-up MRI examination after 6 weeks shows good healing of the tendon with
the continued presence of surrounding edema (D).
Fig. 8 Combination of modalities and US-guided intervention. Partial tear at the myotendinous
junction of the biceps femoris (caput longum) of a soccer player (A). After aspiration of the hematoma, ACP was injected during the same intervention
directly into the injured fibers (B). The short-term follow-up US examination after 2 weeks shows proper healing without
hematoma. Precise evaluation of the tendon segment is difficult on US (C). The follow-up MRI examination after 6 weeks shows good healing of the tendon with
the continued presence of surrounding edema (D).
Fracture ultrasound
US for fracture diagnosis is not capable of completely replacing projection radiography
but should only be used as an additional method in defined indications and to avoid
unnecessary imaging with ionizing radiation [24]. It is used for fracture diagnosis, for monitoring of fracture healing, and for
imaging ligament instabilities and traumatic soft-tissue injuries – particularly in
adolescence.
US imaging always visualizes the cortical bone surface and can be used to confirm
or exclude a fracture ([Fig. 9A, B]). A major advantage of US is the ability to additionally evaluate the soft-tissue
sheath around the bone for detecting hematomas or joint effusion in the same examination.
Additional X-ray examination is advantageous for precise evaluation of the fracture
position/dislocation.
 Fig. 9 Examples of point-of-care US (A–C) and supplementary US examination (D–F) in fracture diagnosis. A–C 28-year-old amateur athlete after a climbing accident (bouldering) with visible interruption
of the cortical bone on ultrasound (A longitudinal section, B cross-section) resulting in diagnosis of a Weber B fracture. The supplementary preoperative
X-ray examination (C) is used to evaluate the position of the fracture. D–F 29-year-old professional ballet dancer with initial suspicion of splenic rupture
in left-sided upper abdominal pain. After the patient history is taken and splenic
trauma is ruled out, the circumscribed point of pain in the region of the 11th rib
indicated by the patient is examined. Dislocated rib fracture with a significant interruption
of the bone (D longitudinal section) and surrounding diffuse hyperechoic hematoma (marked) compared
to the normal intercostal musculature (star, E cross section) can be seen here. The initial X-ray examination was negative (F).
Fig. 9 Examples of point-of-care US (A–C) and supplementary US examination (D–F) in fracture diagnosis. A–C 28-year-old amateur athlete after a climbing accident (bouldering) with visible interruption
of the cortical bone on ultrasound (A longitudinal section, B cross-section) resulting in diagnosis of a Weber B fracture. The supplementary preoperative
X-ray examination (C) is used to evaluate the position of the fracture. D–F 29-year-old professional ballet dancer with initial suspicion of splenic rupture
in left-sided upper abdominal pain. After the patient history is taken and splenic
trauma is ruled out, the circumscribed point of pain in the region of the 11th rib
indicated by the patient is examined. Dislocated rib fracture with a significant interruption
of the bone (D longitudinal section) and surrounding diffuse hyperechoic hematoma (marked) compared
to the normal intercostal musculature (star, E cross section) can be seen here. The initial X-ray examination was negative (F).
In adults, examination can be performed prior to X-ray in the case of suspected rib
fracture(s). If a radiograph has already been acquired without detection of a fracture,
the affected rib (patient scanned at the point of maximum pain) should be examined
sonographically in the case of clinical suspicion of a fracture ([Fig. 9D–F]). Particularly in the case of rib fractures, the intercostal muscle should always
be additionally evaluated since the surrounding hematoma is helpful for fracture detection
([Fig. 9E]). During follow-up, US can be additionally used in the case of a lack of callus
detection on projection radiography since a callus can be visualized with greater
morphological precision and earlier [25]
[26]. Thus, follow-up examinations and the resulting radiation exposure can be increased
in stages.
When documenting fractures, a standard protocol with corresponding documentation should
always be used since it is absolutely necessary to be able to reproduce the exact
location and sound plane in follow-up examinations (e. g., in the case of multiple
examiners).
Mobile ultrasound
Technical innovations in equipment technology in the last decade have resulted in
the availability of increasingly compact and cost-effective ultrasound equipment.
These devices can be transmitted to a tablet or cell phone with a cable or via Wi-Fi
(Bluetooth or WLAN). This makes ultrasound a location-independent modality that can
be used clinically as well as preclinically. It is becoming increasingly established
in different medical disciplines. Therefore, mobile devices can be used directly at
the patient bedside as an expansion of the clinical examination and can be used preclinically
in emergency medical care (e. g., for diagnosing pneumothorax after trauma or for
FAST ultrasound). In sports traumatology, such systems have not yet become fully established
or are only used on a supplementary basis. In a comparison of multiple mobile US devices
(hand-held devices), none of the evaluated devices had all of the features desired
by experts (image quality, ease-of-use, portability, total cost, availability of different
probes) [27]. However, due to their compactness, these devices offer advantages for individual
areas ([Table 1]).
Table 1
Overview of the areas of application and general advantages and disadvantages of mobile
ultrasound. Adapted based on Hees et al. [27].
|
Application area
|
Advantages
|
Disadvantages
|
|
|
|
|
|
|
|
|
|
|
|
|
-
US-guided intervention
-
Fracture diagnosis
-
Trauma (eFAST)
|
|
|
The published literature on the use of mobile ultrasound devices in sports traumatology
is currently still sparse. Individual studies were able to show that standard measurements
of muscle thickness and the evaluation of muscle architecture with mobile ultrasound
devices have good comparability with standard ultrasound [28]. From clinical experience, it can be reported that superficial structures, e. g.,
the quadriceps muscle or the muscles of the lower leg, can be evaluated with mobile
devices with acceptable image quality. Difficulties arise at anatomical locations
with significantly greater muscle volumes, e. g. when evaluating the ischiocrural
group (hamstrings) or their proximal tendon insertions. Mobile ultrasound devices
reach their limit here regarding image quality due to the penetration depth and view.
Use of mobile ultrasound devices on-field (e. g., on the sideline)
Use of mobile ultrasound devices on-field (e. g., on the sideline)
Due to their compact size, mobile ultrasound devices can be used directly on the field
at sporting events/competitions [29]. As a rule, they are suitable for quick confirmation of findings from the clinical
examination [5], but their diagnostic significance when used on the field during sporting events/competitions
is limited. Even if they complete the clinical examination, they are not able to handle
the complexity of the situation. In addition to the time pressure, the opinion of
the athlete who may not be able to continue the game/competition even without a pathological
finding (clinical or sonographic) must be taken into consideration in these situations.
In addition, it is important to note that the visualization of an intramuscular hematoma
as a correlate of a structural muscle defect or contusion trauma is relevant for the
diagnosis of acute muscle injuries but cannot be sufficiently evaluated in the early
phase (a few minutes after the injury). Thus, fast evaluation on the field at sporting
events/competitions has the following risks: false-positive findings can be unsettling
for both athletes and examiners; false-negative findings can result in further diagnostic
workup and corresponding targeted therapy or training management not being sufficiently
implemented [30]. For these reasons, the use of ultrasound on the field at sporting events/competitions
has not yet become established and is also not recommended by us.
A much more established area of application is the use of mobile ultrasound after
a competition in the locker room or at training centers. A comprehensive clinical
examination including a focused ultrasound examination can be performed in a quiet
environment. US is helpful not only for the detection of a muscle or tendon injury
but also for the determination of the further course of action (compression bandage,
MRI, injection therapy, physiotherapy, training management). Depending on the findings,
an MRI examination can be planned or these resources can be saved. Thus, acute diagnosis
can be improved and the athlete can receive treatment that is prompt, optimized, and
cost-effective as well as resource-efficient. If mobile ultrasound devices are compared
to traditional stationary ultrasound devices with respect to diagnostic significance,
the results in the literature are acceptable, but they are highly dependent on the
examiner and the body region being examined. [31]
Mobile ultrasound devices have special importance in the framework of away games or
at training camps since interdisciplinary cooperation with the athlete’s established
radiology partners and the necessary infrastructure are often not available on site.
The areas of application include acute injury diagnosis, monitoring, training management
in the case of pain from overuse, and US-guided infiltration. Remote devices are an
interesting option here and represent a possible future use. They allow telemedicine
consultation or a second opinion from a specialist either in real time or with a delay
after transfer of the images (tele-ultrasound) [32].
Summary
US in sports traumatology includes many clinical areas of application – especially
muscle and tendon ultrasound – and is primarily used for a focused initial diagnostic
assessment and intensive follow-up. As a result of technical advancements, mobile
US devices are increasingly being used in training centers and extraclinically, which
includes both advantages and risks (keyword: structured training of examiners). In
contrast, the use of US for diagnostic assessment at sporting events/competitions
has not become established yet due to the complexity and the time pressure. However,
US is used intensively at training centers and training camps. New US applications
like SWE and 3 D vascularization are increasingly being used in tendon diagnosis,
albeit currently primarily in the field of research. In the coming years, tele-ultrasound
will become increasingly important since the focused acquisition of sonographic images
in sports traumatology can be effectively interpreted by an additional specialist
(standardized and focused examination structure).





