

RSS-Feed abonnieren
DOI: 10.1055/a-2378-6902
Ultrasonographic Evaluation of Morphological Changes in Peripheral Nerves after Traumatic Injury and Nerve Repair – A Prospective Study
Autor*innen


Abstract
Purpose Ultrasound (US) has gained in importance for the visualization of morphological changes of injured nerves. After surgical repair, changes in neural structures are seen over time. The correlation of morphologic changes in US with the corresponding nerve function is uncertain. The aim of this study is to determine a correlation of post-traumatic morphological nerve changes with US and with nerve function after surgery.
Materials and Methods This dual-center, prospective cohort study was conducted between 2017 and 2022 and included 20 mixed sensory motor nerve lesions. Patients were followed up clinically (sensitivity, pain, and motor function) with US and electroneuromyography. We determined the US changes of the nerves including the interaction of the tissue after nerve repair and any correlation with nerve function. With US nerve cross-sectional area (CSA), the number of traversing fascicles, hypo-echogenicity, and presence of perineural scar were analyzed.
Results 20 lesions (12 median and 8 ulnar nerves) of 18 patients with intraoperatively confirmed nerve injury of at least 50% in the forearm were included. The average CSA was over 20 mm2 throughout the follow-up period, corresponding to a neuroma in continuity compared to the opposite side (10.75 mm2). Sensibility and motor function at 12 months were 6xS3/4 and 10xM3-5. There was a statistically significant correlation between continuous fascicles on US at 6 months and sensitivity at 12 months.
Conclusion This study supports the presence of post-traumatic morphological changes in nerve fibers with US after traumatic injury. Morphological changes in nerve structure after trauma can be detected with US indicating a correlation between continuity of nerve fascicles and development of sensitivity and motor function.
Introduction
Ultrasound (US) examination is a valuable diagnostic tool in hand surgery. The development of high-frequency (15–25 MHz) and ultra-high-frequency (30–70 MHz) US probes in combination with sophisticated image processing allows for the visualization of the smallest nerves and nerve bundles [1] [2]. Ultrasonography is used to visualize and assess impairment as well as traumatic injuries to nerves [3]. The examination helps to identify and document the cause and extent of nerve lesions as well as nerve transections [4] [5]. Compared to MRI, US scans are demonstrably more cost-effective, offer higher soft-tissue contrast, and allow for real-time examinations of the gliding ability of nerves with a dynamic component [6]. Limiting factors of this diagnostic tool are bones and nerves at a depth of more than 5 cm depending on the chosen probe [7]. Due to its availability and low cost, US examinations remain a very important tool when serial examinations are needed. Signs of nerve damage include a hypoechogenic pattern, swelling or absence of nerve bundles, and intraneural or perineural scarring. Trauma to peripheral nerve trunks can result in nerve fiber loss to varying degrees where complex pathophysiological changes (morphological and metabolic) subsequently occur at the site of injury [8]. US scans can be implemented immediately post-trauma. This differs from ENMGs, where pathological changes may be detected 14 days at the earliest following an injury.
According to Sunderland [9], histologic changes can be divided into five categories. Sunderland I describes a neurapraxia, which sonographically presents as unremarkable. Sunderland II and III describe an axonotmesis, which can sonographically show an increase in size and swelling of the fascicles. Sunderland IV (epineurium intact) and V (complete lesion) correspond to a neurotmesis and US shows a patchy or diffuse increase in echogenicity [10]. In this study, we focused on Sunderland stage V nerve lesions, defined as an interruption of the epineurium, perineurium, and endoneurium, without spontaneous regeneration potential. By definition, a stage IV lesion develops following suturing of the nerve, which may then have regenerative potential.
In case of a loss of nerve continuity, microsurgical repair is mandatory [10]. Surgical nerve suturing is a delicate operation and belongs to the field of microsurgery. The suture should allow for the nerve endings to touch (the ends “should kiss”) without any pressure or tension in the sutured area. The suture is performed using the single button suture technique with a very tiny thread (e. g., Nylon 9–0) and should be done solely in the epineurium [11]. Usually, a group of fascicles is repaired with as few buttons as possible but as many as necessary. In nerve surgery, US can be used to locate normal or pathological anatomy [12]. During microsurgical suturing, the enveloping structure (epineurium) is readapted, thereby creating continuity that can be seen sonographically.
Postoperative sutures are inconspicuous on MR imaging but, depending on the size and type of suture, appear as intraneural hyperechoic spots with comet tail artifacts on US [11]. US scans can provide important information regarding the actual state of the neurorrhaphy (e. g., size, extent, and location of postoperative scarring), indicate potential neuromas (neuroma in continuity, terminal neuroma) [13] and may be useful in advance of a potential second surgery [14]. In the case of complete nerve lesions stump neuromas develop in continuity with the edges of the nerve (round hypoechoic masses, can be displaced or retracted from the site of injury) [15] [16] [17]. In partial nerve lesions, a neuroma may develop along the injured nerve. US scans can estimate the percentage of involved fascicles [17] [18] [19]. Traumatic neuromas are a reactive hyperplasia of neuronal and fibrous tissue of the nerve sheath, which develops at the end of a proximal nerve stump [20]. A neuroma in continuity is defined as an axonotmetic injury in which the axons are disrupted but the connective tissue is continuous (crush or stretching) [21].
US findings in traumatic nerve injuries are well known [7] [12] [13], but there is no study comparing US findings following traumatic nerve injury and repair with a clinical focus on sensory and motoric nerve regeneration. In this study, we wanted to obtain data on the outcome of nerve regeneration following traumatic nerve lesions and nerve repair based on US examinations as well as clinical and electrophysiological outcomes. The focus was on describing several objective parameters in US corresponding to nerve regeneration, which aid in the decision making process regarding the selection of the further treatment after nerve trauma or nerve surgery at any time during regeneration. The approach of this study was a prospective evaluation of US findings as well as clinical sensory and motor function after traumatic nerve injury and nerve repair. We wanted to answer the questions: Are there any correlations between post-traumatic morphologic nerve changes with US findings and clinical nerve function after surgery? Is there a time frame in which pathologic sonographic changes occur?
Methods
Study population
The objective was to establish a descriptive, prospective cohort study. Eligible patients who had undergone surgery were selected. Another requirement for participation in this dual center study (1 university tertiary referral center Level A, 1 regional trauma center Level B; no differences in technological standardization) was a minimum follow-up of 6 months following the surgical procedure. The inclusion criteria and examination protocol were standardized in both centers. The study was approved by the respective local ethics committee. Patient enrollment commenced on the 6/1/2017. Participants provided written informed consent. The patient characteristics of the study participants are shown in [Table 1]. The time baseline was defined as the date of the traumatic nerve lesion. The inclusion criteria were a traumatic nerve injury followed by a nerve repair (directly or with a nerve graft) of the median, ulnar, or radial nerves at the level of the arm, treated and examined during the period of 05/2017–05/2020 with at least 50% transection of the truncal nerve. The exclusion criteria were an age below 18 years and brachial plexus injuries. All participants were treated surgically and were monitored by clinical and sonographic follow-up at 6 weeks, 3 months, 6 months, 9 months, and 12 months postoperatively. In addition, an ENMG examination was arranged after 6 months and 12 months.
|
Characteristic |
Nerve lesions (n=20) |
|
Sex distribution: Male sex (percentage of male sex) |
18 (90%) |
|
Age, y, median (IQR) |
17–72 (42) |
|
Baseline date |
6/1/2017 to 12/29/2020 |
|
Left side |
12 (60%) |
|
Percentage of nerve lesion |
17 x 100%; 2 x 95%, 1 x 50% |
|
Type of included nerves |
8x ulnar nerve, 12x median nerve (17x distal forearm, 3x middle forearm) |
|
Number (N) of microsurgical repairs, Numbers of (N) microsurgical reconstruction with graft |
N=20 N=0 |
Clinical examination
Clinical examinations were established at predefined intervals (6 weeks, 3 months, 6 months, 9 months, and 12 months postoperatively) and were performed using a protocol with clear instructions for both physicians and patients. The clinical examination consisted partially of an inspection (hyposensitivity, hyper-/hypo-hidrosis, hyper-/hypotrichosis, muscle atrophy, skin abnormalities, swelling, nail deformation, etc.). The clinical examination focused on sensitivity, as a subjective parameter, and motor ability, as an objective parameter. The sensitivity was recorded according to the Medical Research Council (MRC) and was therefore graded as S0–S4 [22] (S0=absence of sensitivity in the autonomous area; S1=recovery of deep cutaneous pain sensitivity within the autonomous area of the nerve; S2=return of some degree of superficial cutaneous pain and tactile sensitivity within the autonomous area of the nerve; S3/S3+= return of superficial cutaneous pain and tactile sensitivity throughout the autonomous area, with disappearance of any previous overresponse; S3+= return of sensitivity as in S3; but in addition there is partial recovery of 2-point discrimination within the autonomous area (7–15 mm); S4=complete recovery (2-point discrimination of 2–6 mm). This parameter was recorded every time following careful patient instruction. The motoric ability was evaluated as an objective parameter using the method of Janda, also according to the MRC, and therefore graded from M0-M5 (M0=no discernible muscle contraction: 0% muscle strength; M1=discernible reaction, though not sufficient for movement: approx. 10% muscle strength; M2=movement to the full extent, though not possible against gravity, i. e. in a horizontal plane: approx. 25% muscle strength; M3=movement to the full extent and against gravity, without additional external resistance: approx. 50% muscle strength; M4=movement to the full extent against light to medium resistance: approx. 75% muscle strength; M5=movement to the full extent, even against a strong external resistance: 100% physiological muscle strength.). Pain was assessed based on the Visual Analog Scale (VAS). In addition, the presence of a Hoffmann-Tinel phenomenon was clinically assessed in each case.
Sonographic examination
The following parameters were visualized and evaluated during the sonographic examination: Nerve cross-section, continuous fascicles, echogenicity, and perineural scars. The nerve cross-section was measured in millimeters. For comparison, the opposite nerve was measured as well. The number of continuous fascicles was recorded sonographically. The echogenicity and peri- as well as intraneural scars were assessed. Hypoechogenicity of the suture was defined as a decrease in the echogenicity of the neural structure compared to the area proximal to the suture. A perineural/intraneural scar was defined as an increase in the echogenicity of the neural structure perineurally/intraneurally compared to the area proximally.
Endpoints
The primary endpoint was to determine the morphologic sonographic changes of the nerves including the response of the surrounding tissue after nerve repair. As a secondary endpoint, any correlation between morphologic sonographic changes and nerve function was assessed. The nerve cross-sectional area (CSA in mm2), number of traversing fascicles, potential hypoechogenicity/hyperechogenicity and presence of peri-/intraneural scars were analyzed sonographically at 6 weeks as well as 3, 6, 9, and 12 months postoperatively.
ENMG after 6 and 12 months
An ENMG examination was performed at 6 and 12 months. We used VikingTM On Nicolet EDX (Nicolet-Viking-EDX.pdf (neuroswiss.ch)). The following parameters were recorded: Motor and sensory nerve conduction velocity, amplitude, and motor latency. An ENMG at 6 months was performed in all 20 cases. After 12 months, an ENMG could be performed in all cases that still had a follow-up (n=12).
Results
Participants
We included 20 nerve lesions in 18 patients with intraoperatively confirmed trunk nerve injury. In the forearm, at least 50% of the cross-sectional area of all nerve lesions was affected. 12 median and 8 ulnar nerves were involved. In 17 cases, nerve transection occurred in the distal forearm and in 3 cases in the middle forearm. All lesions were treated surgically through direct nerve suturing. 90% of the participants were men and the median age at the time of the surgery was 42 years. There was a minimum follow-up of at least 6 months in all cases (100%). A follow-up period of at least 9 months was achieved in 14 cases (70%) and of at least 12 months in 12 cases (60%). In the clinical examination at 12 months, sensitivity presented as follows: 1x S1, 5x S2, 5x S3, and 1x S4. A motor function of M3–5 at 12 months was seen in 10 out of 12 patients. The results of the clinical examinations are summarized in [Fig. 1] and [Fig. 2].


Ultrasound
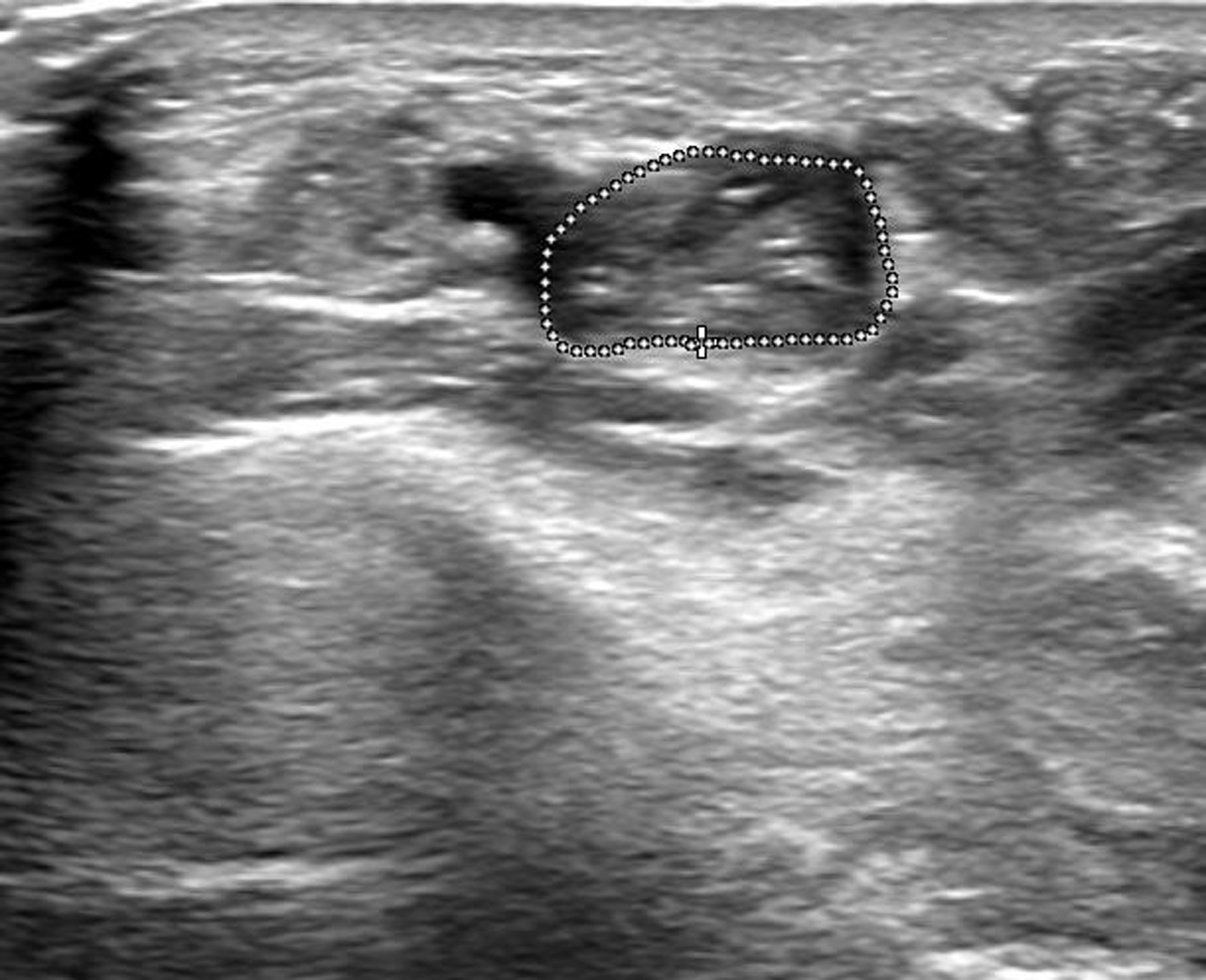
The sonographic results are summarized in [Table 2] and [Fig. 3] [4] [5] [6] [7] [8]. Compared to the average nerve cross-sectional area of 20 mm2 at 6 weeks postoperatively, the participants showed nerve cross-sectional areas of 25.7 mm2, 26.3 mm2, 23 mm2, and 25 mm2 at 3, 6, 9, and 12 months, respectively. Consequently, the average CSA in mm2 throughout the follow-up period was more than 20 mm2. In comparison, the opposite side showed average CSAs of 10.75 mm2 after 6 weeks. Compared to the sonographically detected average number of 10 continuous fascicles at 6 weeks postoperatively, participants had 10, 15, 12, and 11 continuous fascicles at 3, 6, 9, and 12 months, respectively. Compared to 6 patients with hypoechogenicity at 6 weeks postoperatively, 6, 3, 1, and 2 patients showed hypoechogenicity at 3, 6, 9, and 12 months, respectively. Compared to 1 patient with sonographically proven perineural scarring at 6 weeks postoperatively, 2, 2, 3, and 1 patient had sonographically proven perineural scarring at 3, 6, 9, and 12 months, respectively.





|
Time points |
|||||
|---|---|---|---|---|---|
|
Morphology US |
6 weeks (n=20) |
3 months (n=20) |
6 months (n=20) |
9 months (n=14) |
12 months (n=12) |
|
CSA in mm2 |
20 |
25.7 |
26.3 |
23 |
25 |
|
Traversing fascicles (Number of fascicles) |
10 |
10 |
15 |
12 |
11 |
|
Hypo-echogenicity (Number of nerves affected) |
6 |
6 |
3 |
1 |
2 |
|
Perineural scars (Number of nerves affected) |
1 |
2 |
2 |
3 |
1 |
|
Intraneural scars (Number of nerves affected) |
0 |
0 |
0 |
0 |
0 |
There was a statistically significant correlation between the number of continuous fascicles on sonography at 6 weeks and the level of sensitivity at 6 weeks postoperatively (0.018). For sonography at 3 months and level of sensitivity at 3 months postoperatively, the p-value was 0.032. For sonography at 6 months and level of sensitivity at 12 months postoperatively, the p-value was 0.031. The only statistically significant difference concerning the motor function was a p-value of 0.003 for sonography at 6 weeks.
There were no intraneural scars (hyperechogenicity within the nerve).
Irregular bulging of hypoechogenic tissue at the neurorrhaphy site was interpreted as a pathologic sign, reflecting inadequate fusion of nerve edges and a sign of a postsurgical neuroma formation.
According to our definition (axonotmetic injury in which the axons are severed but the connective tissue is continuous after surgical suturing [21]), all nerves developed a neuroma in continuity. Of these 20 nerve lesions, 3 (15%) were clinically relevant (pain VAS>3/10) at 6 months. Allodynia was not present in any patient.
Sensitivity of at least S3 increased from 25% at 6 months to 36% at 9 months and to 50% at 12 months during the indicated period. Motor function of at least M3 increased from 55% at 6 months to 57% at 9 months and to 83% at 12 months.
ENMG
After 6 months (n=20), motor latency ranged from 2.52 ms to 10.7 ms (mean: 5.15 ms, 7 lesions without measurable motor latency). The amplitudes reached values between 0.1 mV and 11.5 mV (average: 2.95 mV, 7 lesions without measurable amplitude). Sensory nerve conduction velocity was detected in 4 cases and averaged 43.8 m/s.
After 12 months (n=12), motor latency ranged from 3.2 ms to 8.75 ms (mean: 5.6 ms, 12 lesions with measurable motor latency). The amplitudes reached values between 0.3 mV and 6.3 mV (average: 2.6 mV, 12 lesions with measurable amplitude). Sensory nerve conduction velocity was detected in 4 cases and averaged 45.5 m/s (of which one lesion did not show any sensory nerve conduction velocity at 6 months).
Lesions with a low motor latency or no motor latency at 6 months at all showed lower clinical motor scores during the course of the study (n=4, no motor latency, M0–1). 2 cases did not show worse clinical symptoms despite having no motor latency (n=2, no motor latency, M3–4). The remaining lesions more or less showed the expected correlation between EMG and function (n=14, the better the motor latency, the higher the M value). After 12 months, 2 lesions showed a rather low clinical value (M2 and M3) despite good ENMG results (motor latency 6.3 ms and 8.75 ms). All but one lesion (n=13) showed an increase in amplitude in ENMGs at 12 months (compared with EMG at 6 months). A prolongation of motor latency and a slowing of nerve conduction velocity was shown in all lesions. If fasciculations and signs of degeneration or regeneration were found in the ENMGs performed, such signs were always noted.
The results of the ENMGs of S3/4 and M4/5 are summarized in [Table 3]. The amplitudes decrease from 6 months to 12 months, the motor latency increases, contrary to the expectation for nerve regeneration. We have observed that the values that were newly derivable after 12 months (n=7) are rather low and therefore reduce the calculated average.
|
Time points |
|||
|---|---|---|---|
|
Amplitudes (average) |
Motor latency (average) |
Nerve conduction velocity (average) |
|
|
S3/4 (6 months) n=5 |
2.5 mV (0.1 mV – 4.9 mV) (n=4) |
4.39 ms (2.52 ms – 4.8 ms) (n=4) |
48 m/s (n=1) |
|
S3/4 (12 months) n=7 |
1.86 mV (0.4 mV – 4.9 mV) (n=7) |
5.83 ms (4.9 ms – 8.75 ms) (n=7) |
43 m/s (n=1) |
|
M4/5 (6 months) n=7 |
3.39 mV (0.4 mV – 11.5 mV) (n=6) |
5.15 ms (3.5 ms – 10.7 ms) (n=6) |
42 m/s (n=1) |
|
M4/5 (12 months) n=6 |
2.93 mV (0.3 mV–6.3 mV) (n=6) |
5.36 ms (3.2 ms–8.3 ms) (n=6) |
42.5 m/s (42 m/s; 43 m/s) (n=2) |
Correlation between US and EMG
No significant correlation was found between US and ENMG. In all lesions, the amplitude (mV) slightly decreased from 6 months postoperatively to 12 months postoperatively due to huge standard deviations. Nerve conduction velocity remained virtually unchanged. Motor latency remained+- constant, although a slight increase in motor latency was also observed in some cases. These observations correlated with the clinical findings but not with US morphology.
Discussion
For the primary endpoint, we chose the sonographic morphological changes of the sutured nerves including the response of the surrounding tissue after nerve repair. We used any correlation between sonographic morphological changes and nerve function for the secondary endpoint.
Our results suggest that there are corresponding post-traumatic sonographic morphological changes in nerve fibers after traumatic injury. Therefore, a correlation between the clinical and electrophysiological sequence and the postoperative time and function is expected. However, sonography only represents the morphological changes and not the function of a nerve.
We emphasize that sonography is the only method to repeatedly visualize the structure of a nerve after surgical repair without the high cost of MRI.
Preoperative
In science, histological parameters are most often used as predictors of peripheral nerve damage and regeneration [8] [23]. However, they are not suitable as an additional examination in patients following a traumatic transection of a nerve. Sonography is a noninvasive examination method and should be taken into account when diagnosing both traumatically and non-traumatically induced nerve impairment [24]. Sonography, if available, is recommended for traumatic nerve lesions even during follow-up and in order to correlate with ENMG and/or clinical findings [25].
Postoperative/CSA
Our findings suggest that following surgical nerve suture, the cross-sectional area of a nerve remains enlarged compared to the opposite side, even months after surgery. These are normal findings in the sutured area of the nerve and are not pathological [11]. Thus, they do not correlate with nerve function. In reconstructive surgery of peripheral nerve lesions, sonography allows for a reliable postoperative evaluation of the continuity of a nerve (e. g., sufficient neurorrhaphy). On a postoperative US scan, the fascicles, which are well adapted by a suture, appear in continuity. Perineural collections can be detected as a mild and fusiform increase in nerve size (cross-sectional area).
Previous studies have also demonstrated that pathologic US findings do not significantly correlate with ENMGs or the clinical picture [26]. Consistently large postoperative CSAs, which persist for months, do not correlate with improved or impaired nerve function. Almost all of the nerves examined in our study met the criteria for a neuroma in continuity, but few were actually clinically relevant. The nerve cross-sectional area shows a marked increase after a few weeks and persists for up to 12 months.
The literature suggests that there is probably no direct correlation between neuroma size, nerve function, and potential for recovery. By definition, all lesions develop a neuroma during the course of recovery, but only 3 out of 20 cases were symptomatic in our cohort. However, if the neuroma is very large (>5x the normal nerve diameter), regeneration is unlikely [10]. This extent of neuroma was not observed in our study.
Previous data shows that an asymptomatic neuroma in patients with thyroid cancer following neck dissection needed no therapeutic intervention. Even after two years there were no significant changes in clinical or sonographic findings [27].
Number of continuous fascicles
After the traumatic transection of a nerve, the distal segment undergoes a slow process of degeneration (Wallerian degeneration) [8]. Our study shows that as early as 6 weeks after microsurgical repair, the first “continuous” fascicles can be detected sonographically. Surgery generates a neuroma in continuity here. We interpret this in the context of Waller’s degeneration taking place. It can be assumed that the enveloping structure of the nerve remains and sonographic differentiation is not possible.
Hypo-echogenicity
Our study supports hypoechogenic changes starting early and then decreasing up to 12 months postoperatively. Irregular bulging of hypoechoic tissue at the neurorrhaphy site should be interpreted as a pathological sign, representing inadequate fusion of nerve edges and a sign of postsurgical neuroma formation [28]. Reactive focal swelling related to edema and venous congestion could also be the result of neural distortion by the scar. Our results suggest that hypo-echogenicity occurs early in the postoperative course and decreases markedly after 9 months.
Perineural/intraneural scarring
Our results showed that perineural scarring after neurorrhaphy was fortunately minimal. The presence of fibrous tissue can hinder MR and US imaging. It can encase the nerve, compressing the fascicles, and as such the nerve is no longer visible in the scar tissue [11]. Therefore, the question is thus how pronounced is the scarring postoperatively. Intraneural scarring was never observed in our sonographic follow-up.
Neuroma
End-to-end neurorrhaphy is an established method that significantly reduces the incidence of symptomatic neuromas [29]. Misdirected or off-target outgrowth, excessive scar tissue, or a gap between the nerve stumps prevents the axons from reaching their final destination. Such an unsuccessful regeneration process leads to the formation of a neuroma [21]. Neuromas in continuity can only be evaluated in conjunction with clinical, sonographic, and ENMG findings.
Correlation of US, ENMG, and clinical findings
No significant correlation was found between US, ENMG, and clinical findings. In all lesions, the amplitude (mV) increased from 6 months postoperatively to 12 months postoperatively. Nerve conduction velocity remained slightly decreased. Motor latency improved for the most part, although an increase in motor latency was also observed in some cases. No statistically significant correlation between ultrasound and clinical findings was observed. However, lesions with a low motor latency or no motor latency at all at 6 months did show a lower clinical motor score during the course of the study. Still, some cases did not show worse clinical symptoms despite worse motor latency. The predominant lesions more or less showed the expected correlation between ENMG and function (more motor latency, higher M value). It shows that although in many cases an ENMG examination provides a supporting and correlating tool, there are also cases where this correlation is absent. We interpret this in our study based on the distribution of the data and the increase in inducible stimuli (increase from n=4 to n=7). We have observed that the values that were newly derivable after 12 months are rather low and therefore reduce the calculated average. It can therefore be assumed that during later regeneration these values will worsen the expected average value and thus influence our results.
US findings in traumatic nerve injuries are well known [7] [12] [13], but in contrast to other already published studies, our study compares US findings following traumatic nerve injury and repair with the clinical outcome regarding sensory and motoric nerve regeneration. In the literature, US is recommended for the diagnostic workup of peripheral nerve lesions in addition to clinical and electrophysiological investigations and should be used in the clinical workup of traumatic nerve lesions. With this study, we provide initial indications of the corresponding temporal sequences of morphological changes and possible correlations between the individual clinical findings.
Limitations
The literature shows that depression and the workers' compensation status are significantly associated with the formation of symptomatic neuromas [29]. Such factors were not considered in this study. Furthermore, only 20 lesions could be included, which limits the power of the study.
Conclusion
To our knowledge, this is the first study comparing US findings after traumatic nerve injury and nerve repair with clinically examined sensory and motoric nerve regeneration and corresponding ENMG findings. It supports the presence of post-traumatic morphological changes in nerve fibers seen with US scans. These post-traumatic morphological changes may be observed in a correlating sequence with postoperative function over time. In accordance with this, our data suggests that the more continuous fascicles are present in the US examination at 6 months postoperatively in mixed motor and sensory nerves, the more likely sensitivity will return at 12 months. Finally, in this prospective study, we only evaluated 20 nerve lesions, highlighting the interest in future studies that quantify the presence of post-traumatic sonographically detectable morphological changes in nerve fibers after traumatic injury to a greater extent. Our data provides pioneering data for future required studies.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Walter U. How small can small nerves be for diagnostic ultrasonography?. Ultraschall Med – Eur J Ultrasound 2019; 40: 400-402
- 2 Puma A, Azulay N, Grecu N. et al. Comparison of high-frequency and ultrahigh-frequency probes in chronic inflammatory demyelinating polyneuropathy. J Neurol 2019; 266: 2277-2285
- 3 Vögelin E. Ultrasonography: the third eye of hand surgeons. J Hand Surg Eur Vol 2020; 45: 219-225
- 4 Toia F, Gagliardo A, D’Arpa S. et al. Preoperative evaluation of peripheral nerve injuries: What is the place for ultrasound?. J Neurosurg 2016; 125: 603-614
- 5 Cartwright MS, Chloros GD, Walker FO. et al. Diagnostic ultrasound for nerve transection. Muscle Nerve 2007; 35: 796-799
- 6 Brown JM, Yablon CM, Morag Y. et al. US of the Peripheral Nerves of the Upper Extremity: A Landmark Approach. RadioGraphics 2016; 36: 452-463
- 7 Ali ZS, Pisapia JM, Ma TS. et al. Ultrasonographic Evaluation of Peripheral Nerves. World Neurosurg 2016; 85: 333-339
- 8 Geuna S, Raimondo S, Ronchi G. et al. Chapter 3 Histology of the Peripheral Nerve and Changes Occurring During Nerve Regeneration. In: International Review of Neurobiology. Elsevier; 2009: 27-46
- 9 Agarwal A, Chandra A, Jaipal U. et al. A panorama of radial nerve pathologies- an imaging diagnosis: a step ahead. Insights Imaging 2018; 9: 1021-1034
- 10 Wijntjes J, Alfen N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve 2021; 63: 455-466
- 11 Tagliafico A, Altafini L, Garello I. et al. Traumatic Neuropathies: Spectrum of Imaging Findings and Postoperative Assessment. Semin Musculoskelet Radiol 2010; 14: 512-522
- 12 Haldeman CL, Baggott CD, Hanna AS. Intraoperative ultrasound-assisted peripheral nerve surgery. Neurosurg Focus 2015; 39: E4
- 13 Bäumer T, Grimm A, Schelle T. Diagnostische Nervensonographie. Radiol 2017; 57: 157-165
- 14 Peer S, Harpf C, Willeit J. et al. Sonographic Evaluation of Primary Peripheral Nerve Repair. J Ultrasound Med 2003; 22: 1317-1322
- 15 O’Reilly MAR, O’Reilly PMR, Sheahan JN. et al. Neuromas as the cause of pain in the residual limbs of amputees. An ultrasound study. Clin Radiol 2016; 71: 1068.e1-1068.e6
- 16 Chen K-H, Lee K-F, Hsu H-C. et al. The Role of High-Resolution Ultrasound in the Diagnosis of a Traumatic Neuroma in an Injured Median Nerve. Am J Phys Med Rehabil 2009; 88: 771-774
- 17 Fodor D, Rodriguez-Garcia SC, Cantisani V. et al. The EFSUMB Guidelines and Recommendations for Musculoskeletal Ultrasound – Part I: Extraarticular Pathologies. Ultraschall Med – Eur J Ultrasound 2022; 43: 34-57
- 18 Lauretti L, D’Alessandris QG, Granata G. et al. Ultrasound evaluation in traumatic peripheral nerve lesions: from diagnosis to surgical planning and follow-up. Acta Neurochir (Wien) 2015; 157: 1947-1951
- 19 Private Specialist Practice Berta Kowalska, Krakow, Poland, Kowalska B. Assessment of the utility of ultrasonography with high-frequency transducers in the diagnosis of posttraumatic neuropathies. J Ultrason 2015; 15: 15-28
- 20 Foltán R, Klíma K, Spacková J, Sedý J. Mechanism of traumatic neuroma development. Med Hypotheses 2008; 71: 572-576
- 21 Dömer P, Kewitz B, Heinen CPG. et al. Analysis of regeneration- and myelination-associated proteins in human neuroma in continuity and discontinuity. Acta Neurochir (Wien) 2018; 160: 1269-1281
- 22 Anđelković S, Lesic A, Bumbasirevic M. et al. The outcomes od 150 consecutive patients with digital nerve injuries treated in a single centre. Turk Neurosurg 2017; 27: 289-293
- 23 Vleggeert-Lankamp CLAM. The role of evaluation methods in the assessment of peripheral nerve regeneration through synthetic conduits: a systematic review: Laboratory investigation. J Neurosurg 2007; 107: 1168-1189
- 24 Mallon S, Starcevic V, Rheinboldt M. et al. Sonographic evaluation of peripheral nerve pathology in the emergency setting. Emerg Radiol 2018; 25: 521-531
- 25 Padua L, Di Pasquale A, Liotta G. et al. Ultrasound as a useful tool in the diagnosis and management of traumatic nerve lesions. Clin Neurophysiol 2013; 124: 1237-1243
- 26 Kerasnoudis A, Tsivgoulis G. Nerve Ultrasound in Peripheral Neuropathies: A Review: Nerve Ultrasound in Peripheral Neuropathies. J Neuroimaging 2015; 25: 528-538
- 27
Zhu L,
Zhang Y,
Zhou G.
et al. Asymptomatic traumatic neuroma after neck dissection in a patient with thyroid
cancer.
- 28 Peer S, Bodner G, Meirer R. et al. Examination of Postoperative Peripheral Nerve Lesions with High-Resolution Sonography. Am J Roentgenol 2001; 177: 415-419
- 29 Maslow JI, LeMone A, Scarola GT, Loeffler BJ, Gaston RG. Digital Nerve Management and Neuroma Prevention in Hand Amputations. Hand (N Y) 2023; 18: 838-844
Correspondence
Publikationsverlauf
Eingereicht: 02. September 2023
Angenommen nach Revision: 21. Juli 2024
Artikel online veröffentlicht:
06. September 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
Léna G. Dietrich, Bettina Juon, Christian Wirtz, Esther Vögelin. Ultrasonographic Evaluation of Morphological Changes in Peripheral Nerves after Traumatic Injury and Nerve Repair – A Prospective Study. Ultrasound Int Open 2024; 10: a23786902.
DOI: 10.1055/a-2378-6902
-
References
- 1 Walter U. How small can small nerves be for diagnostic ultrasonography?. Ultraschall Med – Eur J Ultrasound 2019; 40: 400-402
- 2 Puma A, Azulay N, Grecu N. et al. Comparison of high-frequency and ultrahigh-frequency probes in chronic inflammatory demyelinating polyneuropathy. J Neurol 2019; 266: 2277-2285
- 3 Vögelin E. Ultrasonography: the third eye of hand surgeons. J Hand Surg Eur Vol 2020; 45: 219-225
- 4 Toia F, Gagliardo A, D’Arpa S. et al. Preoperative evaluation of peripheral nerve injuries: What is the place for ultrasound?. J Neurosurg 2016; 125: 603-614
- 5 Cartwright MS, Chloros GD, Walker FO. et al. Diagnostic ultrasound for nerve transection. Muscle Nerve 2007; 35: 796-799
- 6 Brown JM, Yablon CM, Morag Y. et al. US of the Peripheral Nerves of the Upper Extremity: A Landmark Approach. RadioGraphics 2016; 36: 452-463
- 7 Ali ZS, Pisapia JM, Ma TS. et al. Ultrasonographic Evaluation of Peripheral Nerves. World Neurosurg 2016; 85: 333-339
- 8 Geuna S, Raimondo S, Ronchi G. et al. Chapter 3 Histology of the Peripheral Nerve and Changes Occurring During Nerve Regeneration. In: International Review of Neurobiology. Elsevier; 2009: 27-46
- 9 Agarwal A, Chandra A, Jaipal U. et al. A panorama of radial nerve pathologies- an imaging diagnosis: a step ahead. Insights Imaging 2018; 9: 1021-1034
- 10 Wijntjes J, Alfen N. Muscle ultrasound: Present state and future opportunities. Muscle Nerve 2021; 63: 455-466
- 11 Tagliafico A, Altafini L, Garello I. et al. Traumatic Neuropathies: Spectrum of Imaging Findings and Postoperative Assessment. Semin Musculoskelet Radiol 2010; 14: 512-522
- 12 Haldeman CL, Baggott CD, Hanna AS. Intraoperative ultrasound-assisted peripheral nerve surgery. Neurosurg Focus 2015; 39: E4
- 13 Bäumer T, Grimm A, Schelle T. Diagnostische Nervensonographie. Radiol 2017; 57: 157-165
- 14 Peer S, Harpf C, Willeit J. et al. Sonographic Evaluation of Primary Peripheral Nerve Repair. J Ultrasound Med 2003; 22: 1317-1322
- 15 O’Reilly MAR, O’Reilly PMR, Sheahan JN. et al. Neuromas as the cause of pain in the residual limbs of amputees. An ultrasound study. Clin Radiol 2016; 71: 1068.e1-1068.e6
- 16 Chen K-H, Lee K-F, Hsu H-C. et al. The Role of High-Resolution Ultrasound in the Diagnosis of a Traumatic Neuroma in an Injured Median Nerve. Am J Phys Med Rehabil 2009; 88: 771-774
- 17 Fodor D, Rodriguez-Garcia SC, Cantisani V. et al. The EFSUMB Guidelines and Recommendations for Musculoskeletal Ultrasound – Part I: Extraarticular Pathologies. Ultraschall Med – Eur J Ultrasound 2022; 43: 34-57
- 18 Lauretti L, D’Alessandris QG, Granata G. et al. Ultrasound evaluation in traumatic peripheral nerve lesions: from diagnosis to surgical planning and follow-up. Acta Neurochir (Wien) 2015; 157: 1947-1951
- 19 Private Specialist Practice Berta Kowalska, Krakow, Poland, Kowalska B. Assessment of the utility of ultrasonography with high-frequency transducers in the diagnosis of posttraumatic neuropathies. J Ultrason 2015; 15: 15-28
- 20 Foltán R, Klíma K, Spacková J, Sedý J. Mechanism of traumatic neuroma development. Med Hypotheses 2008; 71: 572-576
- 21 Dömer P, Kewitz B, Heinen CPG. et al. Analysis of regeneration- and myelination-associated proteins in human neuroma in continuity and discontinuity. Acta Neurochir (Wien) 2018; 160: 1269-1281
- 22 Anđelković S, Lesic A, Bumbasirevic M. et al. The outcomes od 150 consecutive patients with digital nerve injuries treated in a single centre. Turk Neurosurg 2017; 27: 289-293
- 23 Vleggeert-Lankamp CLAM. The role of evaluation methods in the assessment of peripheral nerve regeneration through synthetic conduits: a systematic review: Laboratory investigation. J Neurosurg 2007; 107: 1168-1189
- 24 Mallon S, Starcevic V, Rheinboldt M. et al. Sonographic evaluation of peripheral nerve pathology in the emergency setting. Emerg Radiol 2018; 25: 521-531
- 25 Padua L, Di Pasquale A, Liotta G. et al. Ultrasound as a useful tool in the diagnosis and management of traumatic nerve lesions. Clin Neurophysiol 2013; 124: 1237-1243
- 26 Kerasnoudis A, Tsivgoulis G. Nerve Ultrasound in Peripheral Neuropathies: A Review: Nerve Ultrasound in Peripheral Neuropathies. J Neuroimaging 2015; 25: 528-538
- 27
Zhu L,
Zhang Y,
Zhou G.
et al. Asymptomatic traumatic neuroma after neck dissection in a patient with thyroid
cancer.
- 28 Peer S, Bodner G, Meirer R. et al. Examination of Postoperative Peripheral Nerve Lesions with High-Resolution Sonography. Am J Roentgenol 2001; 177: 415-419
- 29 Maslow JI, LeMone A, Scarola GT, Loeffler BJ, Gaston RG. Digital Nerve Management and Neuroma Prevention in Hand Amputations. Hand (N Y) 2023; 18: 838-844