

Subscribe to RSS
DOI: 10.1055/a-2432-2732
Preclinical Evidence of Mulberry Leaf Polysaccharides on Diabetic Kidney Disease: a Systematic Review and Meta-Analysis
Authors
This research was funded by the Project of Medical and Health Technology Platform of Zhejiang Province, grant numbers 2022RC004 and 2023KY434.

Abstract
Mulberry leaf polysaccharides (MLPs) have a variety of biological activities. Preliminary scattered evidence of preclinical studies have reported their potenzial effects on diabetic kidney disease (DKD). Here, we intended to assess the preclinical evidence of MLPs and explore their potenzial mechanisms on DKD, offering a scientific reference for the therapeutic use of MLPs. The study has been registered under the CRD42022309117 registration number at PROSPERO. Comprehensive search was conducted across eight databases from their establishment till January 2024, and eight studies with 270 animals were included in the meta-analysis. The primary outcome measurements in the MLP group, including serum creatinine (Scr) (P = 0.0005), blood urea nitrogen (BUN) (P = 0.02), 24-hour urinary protein (UP) (P = 0.001), and urinary microalbumin (UAlb) (P < 0.0001), were significantly reduced compared to the control group. Additionally, MLP treatment was significantly correlated with fasting blood glucose (FBG), total cholesterol (TC), protein expression of TGF-β1, CTGF mRNA, and the kidney index (all P values < 0.05) and delayed the progression of local pathological changes in the kidney. Subgroup analysis revealed significant species differences in the efficacy of MLPs. Also, it showed that the dosage of streptozotocin potenzially affected the Scr and UAlb results, while the duration of MLP treatment influenced UAlb results. MLPs may exert potenzial renal protection by delaying renal fibrosis, inhibiting inflammatory reactions, suppressing the growth hormone–insulin-like growth factor–insulin-like growth factor binding protein axis, and regulating the insulin receptor pathway. In summary, MLPs have multifaceted renal protective effects, suggesting their potenzial for treating DKD.
Keywords
mulberry leaf polysaccharides - DKD - meta-analysis - systematic review - renal protection - Moraceae - MorusIntroduction
Diabetic kidney disease (DKD) emerges as one of the prevailing microvascular complications of diabetes mellitus. It serves as a significant driver of end-stage renal disease (ESRD) on a global scale, potentially truncating a patientʼs lifespan by up to 16.9 years [1], while also imposing remarkable financial and social burdens on families and communities. Fundamental clinical features of DKD frequently entail a decline in the estimated glomerular filtration rate and/or an escalation in the urinary albumin excretion rate [2]. Concurrently, typical pathological manifestations encompass the thickening of the glomerular basement membrane, the proliferation of the mesangial matrix, and the onset of glomerulosclerosis [3]. Due to its insidious onset, rapid progression, and complex pathogenesis, conventional therapies targeting glycemic control, blood pressure, and proteinuria have limited efficacy in halting the progression of renal disease. Moreover, novel targeted therapies and biological treatments are still in the research and development phase and are costly, contributing to the continued rise in the incidence of end-stage DKD in recent years. Consequently, finding safe, economical, and efficient DKD treatments is crucial.
Natural plants represent a readily available resource for drug development. Morus alba L. (family Moraceae) has both medicinal and dietary uses. The total alkaloids extracted from its branches effectively treat hyperglycemia and have been approved as the first natural anti-diabetic drug marketed in China [4]. Mulberry leaf polysaccharides (MLPs), a major natural component of mulberry leaves, represent a compound polysaccharide mainly composed of glucose, gluconic acid, galacturonic acid, fructose, xylose, arabinose, galactose, rhamnose, and mannose. The techniques used for MLP extraction mainly included hot water extraction (HWE), ultrasound-assisted extraction (UAE), enzyme-assisted extraction (EAE), and microwave-assisted extraction (MAE). A comparison of these extraction methods and conditions for polysaccharides from mulberry leaves are summarized in [Table 1] [5], [6], [7], [8], [9], [10]. The structural characteristics of some of the polysaccharides extracted from mulberry leaves are shown in [Fig. 1] [5], [11], [12], [13]. Current research on MLPs has focused primarily on their potential activities in treating hyperglycemia, obesity prevention, immunomodulatory activity, antioxidant activity, and ability to regulate the gut microbiota [14], [15]. Despite the positive effects of MLPs on DKD demonstrated by preliminary preclinical studies, these studies are limited due to their small sample sizes, dispersed evidence, different experimental conditions used, and inadequate knowledge of the mechanisms involved. As a result, it is difficult to come to reliable conclusions, which has limited the use of MLPs in clinical settings. Systematic reviews of preclinical studies are highly regarded as essential tools for gaining knowledge and identifying pathways to guide the design of animal experiments [16]. Hence, this study utilized meta-analysis to assess the effectiveness and underlying mechanisms of MLPs in DKD models, offering preclinical proof and endorsing future clinical treatment and drug advancement.
|
Extraction method |
Conditions |
Yield (%) |
Ref |
|||
|---|---|---|---|---|---|---|
|
Temperature (℃) |
Time (min) |
Solid–liquid ratio (mg/L) |
Power/Enzyme/pH |
|||
|
HWE: hot water extraction; UAE: ultrasound-assisted extraction; MAE: microwave-assisted extraction; EAE: enzyme-assisted extraction |
||||||
|
HWE |
100 |
180 |
15 : 1 |
– |
7.2 |
[5] |
|
HWE |
80 |
60 |
40 : 1 |
– |
11.3 |
[6] |
|
UAE |
60 |
20 |
15 : 1 |
Ultrasonic power 60 W |
10.79 |
[9] |
|
UAE |
57 |
80 |
53 : 1 |
Ultrasonic power 100 W |
6.92 |
[10] |
|
MAE |
88 |
10 |
– |
Sample mass 20 g, microwave power 170 W |
9.41 |
[8] |
|
HWE-EAE |
HWE: 85℃, EAE: 45℃ |
HWE:60 min, EAE:50 min |
30 : 1 |
pH 6.5; Enzyme: pectinase, protease |
24.04 |
[7] |

Results
The preliminary search produced 489 articles based on the predefined retrieval strategy. After EndNoteX9.1 software was used to eliminate duplicates, 179 articles were excluded. Following an examination of the titles and abstracts, an additional 221 papers were disqualified for several factors, as follows: 1) not animal studies; 2) not MLP-related studies, or the subjects were not diabetic animal models; 3) reviews, case analyses, and comments, among others, as specified in the exclusion criteria. Following an additional screening that included a thorough full-text assessment, a further 81 articles were disqualified for reasons including 1) combined MLP therapy, 2) subjects not DKD animal models, 3) lack of predefined outcome indicators, 4) duplicate publication, 5) absence of controls, and 6) absence of full text. Eventually, the systematic review included eight qualifying studies [17], [18], [19], [20], [21], [22], [23], [24] ([Fig. 2]).

The meta-analysis encompassed eight studies, incorporating a collective cohort of 270 animals, distributed between 191 in the treatment group and 79 in the control group. Individual study sample sizes ranged from 16 to 60 animals. The animal species included rats and mice, with four studies using male Wistar rats [17], [20], [23], [24], two studies using male Sprague-Dawley (SD) rats [19], [21], one study using male db/db mice [18], and one study using equal numbers of male and female Kunming mice [22]. The weight range of the mice was 18 – 40 g, and the weights of the SD and Wistar rats were 150 – 270 g. Four studies employed intravenous administration of streptozotocin (STZ) (30 – 120 mg/kg) to induce models [17], [21], [22], [23], while three more studies used an intraperitoneal injection of STZ (50 – 65 mg/kg) [19], [20], [24]. One study used spontaneously diabetic db/db mice to generate the animal models [18]. For anesthesia induction, two studies used ether [17], [23], one study used chloral hydrate [20], and one study used urethane [21], while four studies did not report the anesthetic agents used [18], [19], [22], [24]. Five studies administered drugs orally by gavage (0.1 – 1.0 g/kg/day) [18], [19], [20], [21], [22], while three studies administered drugs by intraperitoneal injection (0.2 – 1.2 g/kg/day) [17], [23], [24]. Five studies implemented a dose gradient of MLPs (0.1 – 1.2 g/kg/day) [17], [20], [22], [23], [24]. The animals in the control groups were given distilled water treatment or an equal amount of physiological saline, and throughout the intervention, the total period ranged from 35 days to 8 weeks. In terms of outcomes, five studies reported primary outcomes, including blood urea nitrogen (BUN) and serum creatinine (Scr) [19], [20], [21], [22], [24], five studies reported 24-hour urinary protein (UP) [17], [19], [21], [22], [23], and five studies reported urinary microalbumin (UAlb) [17], [18], [20], [23], [24]. Secondary outcomes included fasting blood glucose (FBG), reported in seven studies [17], [18], [19], [20], [21], [22], [24], and total cholesterol (TC), reported in three studies [18], [19], [22]. Triglyceride (TG) was reported in two studies [18], [19]. In comparison, transforming growth factor beta1 (TGF-β1) protein expression in renal tissues was reported in three studies [18], [20], [22], connective tissue growth factor (CTGF) mRNA expression in renal tissues was reported in two studies [17], [23], and the kidney index was described in two studies [18], [21]. Several studies also reported other related indicators, such as TGF-β1 mRNA, insulin receptor substrate-1 (IRS-1) mRNA, renal insulin-like growth factor-1/IGF-binding protein-3 (IGF-1/IGFBP-3) mRNA, renal CTGF protein, C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), serum IGF-1/IGFBP-3, nuclear factor kappa B (NF-κB) protein, and renal Smad2, Smad3, and Smad4 protein expression. Additionally, some studies described renal tissue morphology, with some results presented semi-quantitatively, such as the relative area of the extracellular matrix (ECM) or the average optical density value (see [Table 2]).
|
Author (Ref.) |
Species (sex, N) |
Weight (g) |
Model method |
Criteria for modeling |
Anesthetic |
Administration Mode |
Intervention |
Duration of the Treatment |
Outcome index |
|
|---|---|---|---|---|---|---|---|---|---|---|
|
Treatment group (MLPs) |
Control group |
|||||||||
|
Treatment group (MLPs) |
Control group |
|||||||||
|
*MLPs: mulberry leaf polysaccharides; BUN: blood urea nitrogen; Scr: serum creatinine; UP:24-hour urinary protein; UAlb: urinary microalbumin; FBG: fasting blood glucose; TC: total cholesterol; TG: triglyceride; TGF-β1: transforming growth factor beta1; CTGF: connective tissue growth factor; IRS-1: insulin receptor substrate-1; IGF-1: insulin-like growth factor-1; IGFBP-3: IGF-binding protein-3; CRP: C-reactive protein; TNF-α: tumor necrosis factor-alpha; NF-κB: nuclear factor kappa B; ALT: alanine transaminase; AST: aspartate transaminase; SD rats: Sprague-Dawley rats; STZ: streptozotocin; NM: not mentioned; i. p.: intraperitoneal; i. v.: intravenous; NS: normal saline |
||||||||||
|
Liu [24] |
Wistar rats (male, 45/15) |
170 – 270 |
By i. p. injection of |
Rats with a blood glucose |
NM |
i. p. injection |
0.8/0.4/0.2 g/kg/d |
same volume of saline |
8 weeks |
|
|
Song [23] |
Wistar rats (male, 30/10) |
170 – 270 |
By i. v. injection of |
Rats with a blood glucose |
diethyl ether |
i. p. injection |
0.8/0.4/0.2 g/kg/d |
same volume of saline |
8 weeks |
|
|
Huang [21] |
SD rats (male, 8/8) |
200 – 240 |
By. i. v. injection of |
Rats with a blood glucose |
20% urethane, |
oral gavage |
0.15 |
same volume of distilled water |
8 weeks |
|
|
Zhang [20] |
Wistar rats (male, 32/10) |
150 – 250 |
By i. p. injection of |
Rats with a blood glucose |
10% Chloral |
oral gavage |
0.4/0.2/0.1 |
same volume of saline |
8 weeks |
|
|
Chen [22] |
Kunming mice |
18 – 22 |
By i. v. injection of |
Rats with a blood glucose |
NM |
oral gavage |
1/0.5/0.25 |
same volume of saline |
35 days |
|
|
Zhang [19] |
SD rats |
190 – 210 |
By i. p. injection of |
Rats with a blood glucose |
NM |
oral gavage |
0.2 |
same volume of distilled water |
8 weeks |
|
|
Zhang [18] |
db/db and db/m mice |
35 – 40 (db/db), |
spontaneous |
Rats with a blood glucose |
NM |
oral gavage |
0.4 |
same volume of saline |
6 weeks |
|
|
Wu [17] |
Wistar rats (male, 30/10) |
NM |
By i. v. injection of STZ (65 mg/kg) |
Rats with a blood glucose |
diethyl ether |
i. p. injection |
1.2/0.8/0.4 |
same volume of saline |
8 weeks |
|
All studies employed random allocation to the control and intervention groups. Out of the total, two studies (25%) provided sufficient details about the process of random sequence generation [19], [22]. One study used a random number table approach, while another utilized computer-generated random numbers. However, the six remaining studies failed to provide detailed descriptions of the specific procedures used for random allocation, indicating a high risk of bias in developing random sequences (selection bias). Out of all the studies included, two (25%) mentioned that animals were randomly housed [18], [21]. Nevertheless, none of the studies provided information on the baseline characteristics of the animals, allocation concealment, blinding of animal caregivers, researchers, and outcome assessors, or random outcome assessment. Consequently, evaluating the potential bias resulting from the concealment of group allocation and blinding of subjects is still uncertain. Nearly all studies provided complete data except for one study, which failed to indicate whether the missing animals affected the final results [20]. None of the studies discovered any additional sources of bias. The risk of bias summary for each study is presented in [Fig. 3].

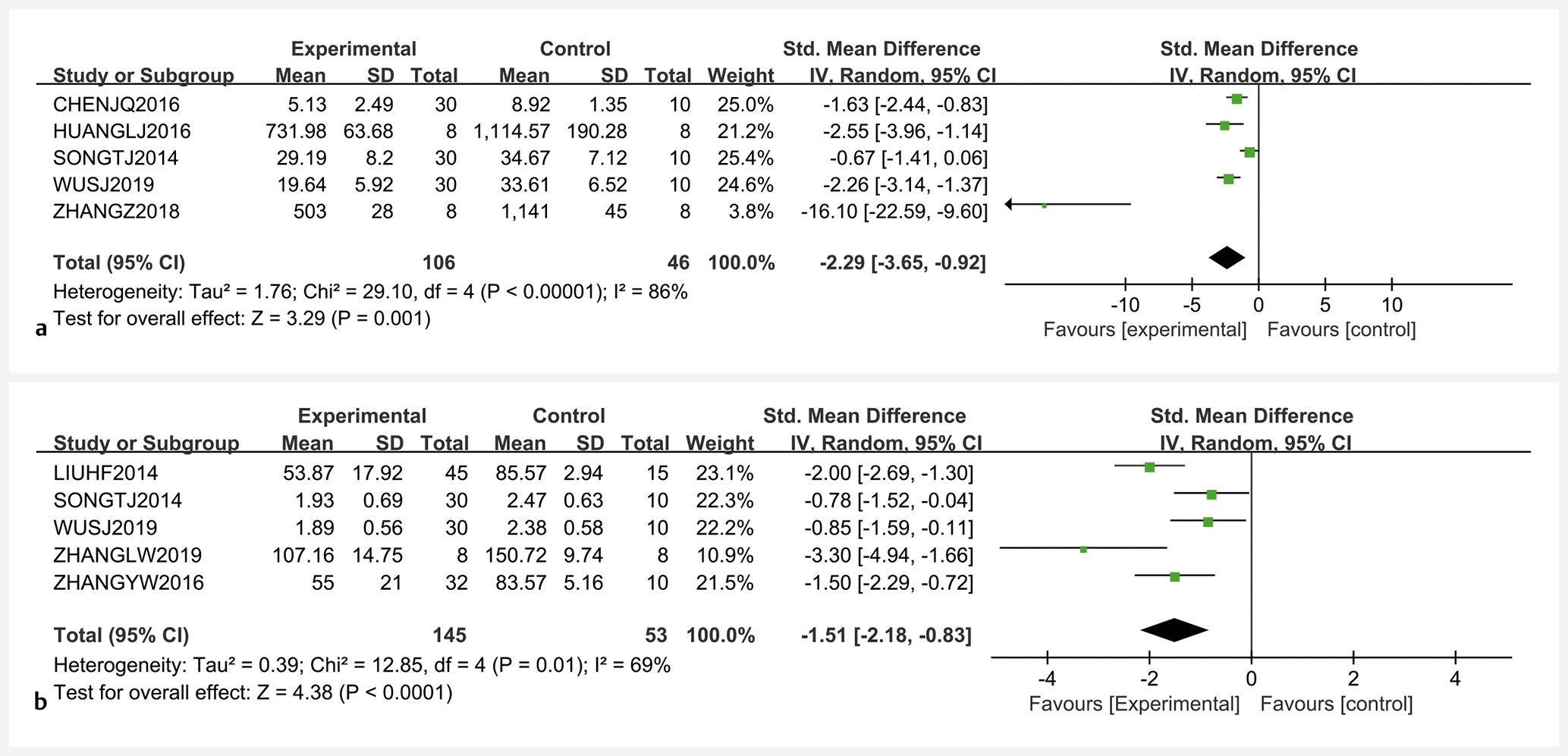
Five research studies examined the influence of MLPs on Scr. Compared to the control group, MLPs substantially decreased Scr (n = 174, SMD = − 1.45, 95% CI [− 2.27, − 0.63], P = 0.0005; heterogeneity: Chi² = 15.88, P = 0.003; I²=75%; [Fig. 4 a]). Five studies also reported the effect of MLPs on BUN. The presence of a significant difference in BUN level was noteworthy between the treatment group and control group (n = 174, SMD = − 1.19, 95% CI [− 2.22, − 0.16], P = 0.02; heterogeneity: Chi² = 26.58, P < 0.0001; I² = 85%; [Fig. 4 b]). Notably, UP was evaluated in five studies, revealing significant heterogeneity in their outcomes. Utilizing a random-effects model, a meta-analysis elucidated that the experimental group manifested a lowered UP levels relative to the control group (n = 152, SMD = − 2.29, 95% CI [− 3.65, − 0.92], P = 0.001; heterogeneity: Chi² = 29.10, P < 0.00 001; I² = 86%; [Fig. 5 a]). There have been five studies that discussed how MLPs affect UAlb. The data indicated that the experimental group had significantly lower UAlb levels following MLP treatment in comparison to the control group (n = 198, SMD = − 1.51, 95% CI [− 2.18, − 0.83], P < 0.0001; heterogeneity: Chi² = 12.85, P = 0.01; I² = 69%; [Fig. 5 b]). Given the notable statistical heterogeneity observed across these studies, a random-effects model was adopted alongside subgroup analysis to elucidate the underlying factors contributing to the heterogeneity further.

FBG served as an outcome measure in seven studies. Relative to the control group, the MLP group exhibited a notably lower FBG (n = 230, SMD = − 2.34, 95% CI [− 2.79, − 1.88], P < 0.00 001; heterogeneity: Chi² = 8.22, P = 0.22; I² = 27%; [Fig. 6 a]). TC values were documented in three investigations. The meta-analysis unveiled that relative to the control group, the experimental group displayed a significantly diminished TC level (n = 72, SMD = − 1.54, 95% CI [− 2.86, − 0.22], P = 0.02; heterogeneity: Chi² = 8.77, P = 0.01; I² = 77%; [Fig. 6 b]). TG levels were reported in two studies. The pooled results did not differ significantly from the control group, despite the individual study results suggesting statistically significant differences (n = 32, SMD = − 6.42, 95% CI [− 13.90, 1.07], P = 0.09; heterogeneity: Chi² = 10.79, P = 0.001; I² = 91%; [Fig. 6 c]). The meta-analysis of the three included studies that assessed the expression of TGF-β1 protein showed that the experimental groupʼs TGF-β1 protein levels were significantly lower than those of the control group (n = 98, SMD = − 2.32, 95% CI [− 3.99, − 0.65], P = 0.007; heterogeneity: Chi² = 14.16, P = 0.0008; I² = 86%; [Fig. 7 a]). The impact of MLP therapy on CTGF mRNA expression was documented in two studies. Relative to the control cohort, the experimental group displayed a significant reduction in CTGF mRNA level (n = 80, SMD = − 1.20, 95% CI [− 1.79, − 0.61], P < 0.0001; heterogeneity: Chi² = 1.16, P = 0.28; I² = 13%; [Fig. 7 b]). Two studies examined the influences of MLPs on the kidney index. Following MLP treatment, the experimental group exhibited a significantly lowered kidney index relative to the control group (n = 32, SMD = − 1.54, 95% CI [− 2.37, − 0.72], P = 0.0002; heterogeneity: Chi² = 0.30, P = 0.58; I² = 0%; [Fig. 7 c]).


Three studies evaluated pathological changes in renal tissues [18], [19], [22]. Following H&E or periodic acid-Schiff (PAS) staining, the MLP treatment group demonstrated much less proliferation of the mesangial matrix and mesangial cells than the control group, with a remarkable improvement of basement membrane thickening. The electron microscope verified these findings [22]. Optical microscopy results reported in two studies demonstrated improvements in epithelial cell swelling and reduced interstitial inflammatory cell infiltration in the drug-treated group [19], [22]. Additionally, it was discovered that the relative area of the ECM was substantially smaller than that of the control group [19]. The average optical density value (IOD)/AREA in the drug group was significantly lower than in the control group, according to the analysis of the IOD value of the PAS-positive basement membrane and the pixel area of the glomerular vascular tuft (AREA) [18].
Subgroup analysis of Scr revealed significant heterogeneity attributable to differences in the injected dose of STZ (I² = 93.4%; P < 0.05) and species variation (I² = 86.9%; P < 0.05). A comparison of Scr levels between the different rodent types indicated that MLPs exhibited superior efficacy in SD rats (SMD, − 3.20; 95% CI, [− 4.34, − 2.05]) compared to mice (SMD, − 0.82; 95% CI, [− 1.56, − 0.08]) and Wistar rats (SMD, − 0.78; 95% CI, [− 1.24, − 0.31]). Furthermore, establishment of the animal models using low-dose STZ (STZ ≤ 60 mg/kg) led to better improvements in the Scr levels compared to those given high STZ doses (STZ > 60 mg/kg) (SMD, − 3.20; 95% CI, [− 4.34, − 2.05] vs. SMD, − 0.79; 95% CI, [− 1.18, − 0.39]) (See Table 1S, Supporting Information). In the UAlb subgroup analysis, significant heterogeneity was observed, possibly due to species variation (I² = 80.4%; P < 0.05), duration of drug administration (I² = 80.4%; P < 0.05), and different methods used for model establishment (I² = 80.4%; P < 0.05). Comparative analysis of UAlb among the different rodent types showed that MLP treatment was more effective in db/db mice (SMD, − 3.3; 95% CI, [− 4.94, − 1.66]) compared to Wistar rats (SMD, − 1.29; 95% CI, [− 1.87, − 0.71]). When MLPs were administered for less than 8 weeks, a more significant reduction in UAlb was observed compared to treatment for longer than 8 weeks (SMD, − 3.3; 95% CI, [− 4.94, − 1.66] vs. SMD, − 1.29; 95% CI, [− 1.87, − 0.71]). Furthermore, the use of spontaneous db/db mice resulted in better improvement in UAlb compared to STZ-induced diabetic models (SMD, − 3.3; 95% CI, [− 4.94, − 1.66] vs. SMD, − 1.29; 95% CI, [− 1.87, − 0.71]) (see Table 2S, Supporting Information). Species stratification in the BUN subgroup analysis substantially reduced the heterogeneity of the results (I² = 81.2%; P < 0.05). Comparative study of BUN among the different rodent types showed that MLP treatment was more effective in SD rats (SMD, − 3.03; 95% CI, [− 5.99, − 0.08]) compared to mice (SMD, − 1.28; 95% CI, [− 2.06, − 0.51]) and Wistar rats (SMD, − 0.03; 95% CI, [− 0.48, 0.42]) (see Table 3S, Supporting Information). The UP subgroup analysis did not reveal any significant impacts on the heterogeneity of the data concerning the amount of STZ injection, type of rodent, dosage of the drugs, or duration of drug administration (see Table 4S, Supporting Information).
Sensitivity analysis of Scr, BUN, UAlb, and UP did not reveal any significant bias, indicating the stability of the meta-analysis results (Fig. 1S, Supporting Information).
Notably, none of the studies included in the analysis reported any adverse events, making it difficult to determine whether or not the MLP treatment was related to any complications or adverse events.
Discussion
To our knowledge, this study represents the first meta-analysis of preclinical evidence that examines the protective benefits of MLPs on DKD. The results indicated that MLP treatment offers multifaceted protection against DKD, suggesting its potential as a therapeutic agent for DKD. Nevertheless, the heterogeneity in the outcomes must not be disregarded. This heterogeneity may partially stem from differences among the included studies, including pharmacological variations, differences in the type of rodent used as models, and the study designs. Sensitivity analysis suggested the stability of the results. For further exploration, a random-effects model was cautiously employed. We conducted subgroup analyses of outcome measures, specifically, different doses of STZ injection, rodent type, drug doses, and duration of drug administration. The results indicated significant differences in the efficacy of MLP treatment associated with the animal model used, with more substantial improvements in the Scr and BUN levels observed in SD rats compared to the other animal models (P < 0.05). However, improvements in UAlb were more marked in db/db mice (P < 0.05). It is thus suggested that the animal model should be specifically selected to observe more significant differences in outcomes and treatment efficacy. The selection of the STZ dosage is a crucial determinant for successfully establishing the DKD model. Lower dosages of STZ may not effectively cause diabetes as anticipated. However, high dosages of STZ can lead to either the mortality of the animal or nephrotoxicity [25]. The subgroup analysis in this study revealed notable disparities in the improvement of Scr and UAlb between high-dose STZ (≥ 60 mg/kg) and low-dose STZ (< 60 mg/kg), with animals administered low-dose STZ demonstrating superior effectiveness. A possible explanation is that besides inducing hyperglycemia, high-dose STZ has toxic effects on the kidneys, which can act as a confounding factor in animal models of DKD. Considering that many studies still use high doses of STZ for modeling, it is recommended that future DKD research employ appropriate STZ doses (40 – 60 mg/kg) for successful modeling without the induction of nephrotoxicity. In clinical practice, the dose-response and time-response interactions of drugs are crucial. The subgroup analysis of UAlb indicated that the duration of drug action had a marked effect on the treatment efficacy. In contrast, the dosage did not significantly impact the results. The effectiveness of MLP treatment did not improve with time. Nonetheless, it revealed a negative tendency in the later stages, indicating that treatment duration may be a source of heterogeneity. We tentatively attribute this to the progressive and irreversible nature of DKD, where prolongation of MLP treatment only delays rather than reverses DKD progression. As the disease progresses, UAlb levels may not accurately reflect the extent of kidney damage, and concurrent evaluation of kidney function using indicators such as Scr, BUN, and creatinine clearance is thus recommended. The results of the subgroup analysis should be considered carefully due to the small sample size. Because of the limited number of articles, we could not perform a meta-regression analysis.
For diabetics, hyperglycemia has traditionally been regarded as the triggering factor for DKD, where dysfunctions in glucose and lipid metabolism contribute to hemodynamic disturbances in renal blood flow, thereby constituting the primary pathological mechanisms underlying DKD. Numerous studies show that keeping blood glucose levels close to normal can prevent the development of overt proteinuria and lower the urinary albumin excretion rate [26]. Therefore, improving blood glucose control is believed to be effective for renal protection. Numerous preclinical investigations have demonstrated the strong hypoglycemic bioactivity of MLPs [14], [15]. MLPs can reduce the levels of free fatty acids in mice with type 2 diabetes [27]. According to recent research, isolated and purified MLP-2C can decrease cholesterol levels by enhancing the conversion of cholesterol to bile acids, reducing the generation of endogenous cholesterol, and raising cholesterol efflux [5]. In comparison to the control group, the current meta-analysisʼs findings likewise demonstrated a significant drop in FBG and an improvement in TC following MLP treatment. Two studies involving TG levels suggested that MLP treatment could lower TG, although no positive results were observed after the combination. The heterogeneity of these two studies (P = 0.001, I² = 91%) may have led to wide confidence intervals in the random-effects model and produced negative results (P = 0.09). Confirmation of the kidney protective effects of MLPs concerning improvements in glucose and lipid metabolism necessitates additional investigation. Considering the high variability in FBG measurements, future evaluations could include the measurement of HbA1c or glycosylated albumin better to assess the impact of glucose metabolism on renal function.
The molecular and biological mechanisms underlying the renoprotective effects of MLPs have not been fully elucidated. The possible mechanisms by which MLPs treat DKD can be summarized as follows ([Fig. 8]): (1) anti-fibrosis: renal interstitial fibrosis is seen as the last common pathway that leads to renal failure in DKD. Along with the downstream transcription factor Smad, TGF-β1 is an essential mediator of fibrosis [28]. Dysregulation of the TGF-β1/Smad pathway may either promote ECM deposition directly or induce epithelial cells to transform into myofibroblasts through the epithelial-mesenchymal transition (EMT), resulting in renal fibrosis [29]. CTGF, as a downstream effector of TGF-β1, accelerates the progression of renal fibrosis induced by TGF-β [30]. The comprehensive findings from prior research [17], [18], [20], [22], [23], [24] unveiled that MLP therapy markedly reduced the levels of both TGF-β1 protein and CTGF mRNA, alongside diminished expression of TGF-β1 mRNA and Smad protein relative to the control group. These findings indicated that MLPs may reduce activation of the TGF-β1/Smad signaling pathway, and downregulate the mRNA expression of CTGF, thus mitigating the progression of diabetic kidney fibrosis. (2) Anti-inflammation: earlier research has demonstrated that one of the critical factors in the development of DKD is inflammation. The transcription factor NF-κB is essential for initiating and regulating inflammatory responses. It can cause over-activation of pathways linked to TNF-α, IL-6, hs-CRP, and MCP-1 (monocyte chemotactic protein-1), setting off a chain reaction of inflammatory responses and worsening damage to renal tissue [31]. Animal experiments [21], [22] have shown that MLPs can downregulate NF-κB expression in the kidney tissues of DKD mice and rats and reduce serum TNF-α and hs-CRP levels. This implies that MLPs may modulate the protein expression of NF-κB in the kidney, limit the production of inflammatory factors, alleviate renal tissue inflammation, reduce mesangial matrix proliferation, and thus mitigate DKD. (3) Dysregulation of the growth hormone–insulin-like growth factor–insulin-like growth factor binding protein (GH–IGF–IGFBP) axis: another element in the pathophysiology of DKD is the GH–IGF–IGFBP axis [32]. Serum IGF-1 induces renal interstitial cell proliferation and has been linked to proliferative alterations in the kidneyʼs vasculature. Studies have shown that increased expression of renal IGF-1 receptors may lead to kidney hypertrophy, a hallmark of DKD. A meta-analysis of clinical studies revealed a correlation between high levels of IGF-1 or an elevated IGF-1/IGFBP-3 ratio and the advancement of renal disease, leading to a higher all-cause mortality rate [33]. It was found that MLP treatment decreased the levels of IGF-1/IGFBP-3 mRNA in both the serum and kidney [19]. This suggests that the therapeutic impact of MLPs on DKD may be attributed to the inhibition of the IGF-1/IGFBP-3 signaling pathway. However, the specific mechanism awaits further investigations. (4) Regulation of metabolism: as described, dysregulation of glucolipid metabolism is a crucial pathological process involved in DKD. In addition to exerting renoprotective effects by the direct lowering of glucose and lipid levels, MLPs were shown to inhibit the development of insulin resistance [34]. Preliminary studies have found that MLPs can regulate the expression of IRS-1, AdipoR1, and resistin mRNA in DKD rats [20], [35], [36], among which, improving insulin sensitivity may play an important role in stabilizing glucose–lipid metabolism and thus mitigating the progression of DKD. However, further in-depth molecular studies are required to assess the mechanism underlying the effects of MLPs.

Before researching the biological activities and applications of polysaccharides, extracting and purifying them is necessary. Variations in extraction procedures, separation techniques, and purification processes can result in discrepancies in the chemical makeup of polysaccharide extracts, which can impact the reliability of subsequent evaluations of biological activity. Currently, due to their significant diversity and complex chemical compositions and structures, there is no standardized, simple, low-cost, and effective separation and purification system for MLPs [15]. The different extraction methods lead to differences in the yield of MLPs, as is shown in [Table 1]. Among the various reported extraction processes on MLPs, Yang et al. optimized the extraction conditions under the synergy of HAE and EAE by Box–Behnken design and obtained the best collaborative extraction processes with the extraction rate of MLPs reaching as high as 24.04 ± 0.98% [7]. It is thus recommended that future efforts focus on quality control and the establishment of standardization in the extraction and purification process, fully considering the samplesʼ purity to ensure the productʼs safety and effectiveness.
Compared to clinical trials, animal experiments are more exploratory in their research protocols and intervention processes. The quality of this preclinical systematic review was rated as moderate. The risk of bias tool for animal studies (RoBT), which was established by the Systematic Review Center for Laboratory Animal Experimentation (SYRCLE), has been widely used in preclinical systematic reviews and recommended by other organizations as a standard for methodological quality assessment [37]. We recommend that future researchers adhere to SYRCLEʼs RoBT for evaluating the methodological quality of animal experiments and complying with the reporting criteria of preclinical studies as defined in the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines [38]. It is crucial to record both the characteristics of animals and baseline data carefully. Additionally, providing thorough descriptions of the randomization and allocation concealment processes, estimating appropriate sample sizes, maintaining rigorous blinding protocols, and ensuring outcome blinding are imperative to elevate the quality of animal experiments and promote reporting standards.
The investigation into MLPs is still in its initial phases and has concentrated chiefly on cellular and animal models. There is a lack of enough clinical research to confirm the effectiveness and safety of these substances in humans. Hence, we propose enhancing interdisciplinary cooperation and carrying out controlled human trials under appropriate conditions integrating pharmacokinetics, toxicology, and clinical experiments. This approach will enable a comprehensive investigation of the clinical effectiveness, optimal dosage, and treatment duration of MLPs, thereby thoroughly assessing their efficacy and potential risks.
This systematic review may lack toxicological information. While a few of the included studies described normal levels of alanine transaminase (ALT) and aspartate transaminase (AST) following treatment with MLPs, this is still far from actual toxicological reports. We advise that future researchers enhance the documentation of toxicological findings.
The limitations of our study may include the following. (1) Research on natural materials associated with traditional Chinese medicine primarily focuses on Southeast Asia. Due to probable language barriers, only papers written in Chinese or English were included in the search, leading to an unavoidable selection bias. (2) The included studies lacked negative results, and the animal models did not incorporate animals with relevant comorbidities (the animals used in the studies lacked relevant comorbidities or risk factors), potentially leading to overestimating the treatment efficacy [39]. Animal models having comorbidities, such as obesity, hyperlipidemia, hypertension, or other risk factors, should be used when conditions allow. This may better reflect the physiology of diabetic patients and assist in the therapeutic translation of experimental outcomes [40]. (3) For the multiple-dose group, we adopted the strategy recommended by CHSRI, combining them to form a single-dose group. However, this approach also loses some information regarding dose-response relationships. (4) Mechanism-related indicators are insufficient for the comprehensive description of the effects of MLPs on renal protection mechanisms. Moreover, the studies on relevant indicators were independent, lacking connections between mechanisms, and are thus unable to reflect the relationships between different mechanisms. Future studies are advised to consider high-throughput analysis to assist in revealing the primary targets or critical pathways linked with the impacts of MLPs.
In conclusion, preclinical in vivo evidence indicates that MLPs protect the kidneys and are thus potential candidates for treating DKD. Further high-quality, large-sample, multi-mechanism studies are required to assess the effectiveness, safety, and renal protective mechanisms of MLPs. Additionally, it is unknown whether the results observed in animal models apply to humans, necessitating further evaluation by clinical trials.
Material and Methods
The study was registered at PROSPERO under registration number CRD42022309117. The systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards, the preferred reporting items for systematic reviews and meta-analyses.
A computerized search was performed in the Web of Science, Cochrane Central Register of Controlled Trials, EMBASE, and PubMed databases, as well as in Chinese databases, including SinoMed, Wanfang, VIP, and CNKI, to identify studies investigating MLP treatment of DKD in animal models. Every search strategy was used from the databaseʼs creation until January 2024. The search encompassed articles published solely in Chinese and English. In addition, the bibliographies of the incorporated articles underwent manual scrutiny to uncover additional relevant research. The full details regarding the literature search strategy are to be found in Table 5S (Supporting information).
Two authors (Y. W. and J. Z.) independently reviewed the research abstracts and titles and then conducted full-text reviews to determine which papers should be included or excluded. The inclusion criteria were as follows. (1) Selection of diabetic animal models as the study model. Models can be constructed using many methods, with the criterion for success being a FBG level of more than 11.1 mmol/L. (2) The treatment group received exclusively MLPs at any dosage, whereas the control group received non-functional fluids of the same volume or no therapy. There were no limitations on the delivery method and the formulation. (3) The primary outcome measures were UAlb, UP, BUN, and Scr. For a more comprehensive assessment of renal damage, at least one of four parameters, namely, Scr, BUN, UP, or UAlb, had to be included. The secondary outcomes assessed in this study were FBG, TC, and TG levels. Additionally, the study investigated the protective mechanism of MLPs in DKD by measuring TGF-β1 protein levels and CTGF mRNA expression, among other factors. (4) Randomized controlled trials. The following were the criteria for exclusion: (1) studies that are not in vivo, including in vitro investigations, clinical trials, case reports, reviews, editorials, and abstracts; (2) alternative animal models; (3) MLP treatment combined with other medications; (4) absence of predetermined primary outcome measures; (5) lack of a control group; (6) duplicate publications.
The following information was independently extracted by two authors, identified as B. C. and D. W.: (1) the year the study was published and the name of the first author; (2) specific information about the animals used in each study, including the number, species, sex, and weight; (3) how the animal models were developed, including the drug dosages needed, the method of administration, and the criteria used to determine if the model was successful, as well as details about the anesthesia protocols used; (4) the intervention procedures for both the treatment and control groups will include details such as the method of administration, the dosages of drug given, and the length of time the intervention will last; (5) the primary and secondary outcome measures will be used to evaluate the effectiveness of the intervention. The variables were retrieved from the final time if the results were acquired at several time points. All data were collected if results were obtained from interventions in subgroups with varying dosages. Efforts were made to reach out to the authors for more information, but without a response, the data were obtained through WebPlotDigitizer. During the data extraction procedure, discrepancies were handled by conversation or discussion with a third party (Y. R.).
The assessment of study quality for each included study was independently undertaken through two authors (Y. W. and B. C.) using the SYRCLEʼs RoBT [37]. This tool comprises 10 components, encompassing aspects, such as sequence generation, baseline characteristics, allocation concealment, random housing of animals, blinding for caregivers and researchers, random outcome assessment, blinding for outcome assessors, incomplete outcome data reporting, selective outcome reporting, and identification of other potential sources of bias. Each component is assigned a score of 1 point, yielding a total score out of 10. In cases of disagreement, a third party (Y. R.) intervened to resolve discrepancies through arbitration.
When there were differences in the dosage of MLP among subgroups, the Cochrane Handbook for Systematic Reviews of Interventions (CHSRI Version 6.4, 2023) [41] suggested a technique to handle this by merging the results of the subgroups with varying dosages into a single treatment group. The formula employed for merging continuous variables was as follows:
The predetermined outcomes were regarded as continuous variables, and their evaluation was implemented utilizing the mean difference (MD) with a 95% confidence interval (CI). In cases where there were discrepancies in measurement methods or units used for outcome reporting, the standardized MD (SMD) was employed rather than MD to compute the overall effect size. It was attempted to evaluate the statistical heterogeneity through the Cochrane Q-test and the I2 statistic; a value of I2 below 50% was suggestive of the adoption of a fixed-effects model, while I2 surpassing 50% led to the utilization of a random-effects model. It was attempted to implement subgroup analysis to figure out the influences of variables involving animal species, STZ injection dosage, drug dosage levels, and treatment duration on the outcomes, revealing potential sources of clinical heterogeneity. For the purpose of conducting sensitivity analysis, STATA 16.0 was employed to ascertain the robustness and consistency of the primary outcomes. Meta-regression was precluded due to the restricted number of studies. The RevMan 5.4.1 was utilized for meta-analysis. Given the inclusion of less than 10 studies, no publication bias was analyzed. P subordinate 0.05 was regarded to signify statistical significance.
Contributorsʼ Statement
Data collection: Y.Wang, J.Zhang; design of the study: Y.Wang, Y.Ruan; statistical analysis: D.Wang, B.Chen; analysis and interpretation of the data: B.Chen, J.Zhang; drafting the manuscript: Y.Wang, B.Chen; critical revision of the manuscript: Y.Wang.
Conflict of Interest
The authors declare that they have no conflict of interest.
Supporting Information
- Supporting Information (PDF) (opens in new window)
The literature search strategy, sensitivity analyses, and subgroup analysis are available as Supporting Information.
-
References
- 1 Wen CP, Chang CH, Tsai MK, Lee JH, Lu PJ, Tsai SP, Wen C, Chen CH, Kao CW, Tsao CK, Wu X. Diabetes with early kidney involvement may shorten life expectancy by 16 years. Kidney Int 2017; 92: 388-396
- 2 ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Leon J, Lyons SK, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Gabbay RA. on behalf of the American Diabetes A. 11. Chronic kidney disease and risk management: Standards of care in diabetes-2023. Diabetes Care 2023; 46: S191-S202
- 3 Reidy K, Kang HM, Hostetter T, Susztak K. Molecular mechanisms of diabetic kidney disease. J Clin Invest 2014; 124: 2333-2340
- 4 Qu L, Liang X, Tian G, Zhang G, Wu Q, Huang X, Cui Y, Liu Y, Shen Z, Xiao C, Qin Y, Miao H, Zhang Y, Li Z, Ye S, Zhang X, Yang J, Cao G, Li Y, Yang G, Hu J, Wang X, Li Z, Li Y, Zhang X, Zhang G, Chen L, Hua W, Yu M, Lu C, Zhang X, Jiang H. Efficacy and safety of mulberry twig alkaloids tablet for the treatment of type 2 diabetes: A multicenter, randomized, double-blind, double-dummy, and parallel controlled clinical trial. Diabetes Care 2021; 44: 1324-1333
- 5 Li R, Zhou J, Zhang X, Zhang T, Wang J, Zhang M, He C, Chen H. Isolation, structural characterization and cholesterol-lowering effects of a novel polysaccharide from mulberry (Morus alba L.) leaf. Ind Crops Prod 2023; 202: 117010
- 6 Wang F, Li J, Jiang Y. Polysaccharides from mulberry leaf in relation to their antioxidant activity and antibacterial ability. J Food Process Eng 2010; 33: 39-50
- 7 Yang S, Li Y, Jia D, Yao K, Liu W. The synergy of Box-Behnken designs on the optimization of polysaccharide extraction from mulberry leaves. Ind Crops Prod 2017; 99: 70-78
- 8 Thirugnanasambandham K, Sivakumar V, Maran JP. Microwave-assisted extraction of polysaccharides from mulberry leaves. Int J Biol Macromol 2015; 72: 1-5
- 9 Ying Z, Han X, Li J. Ultrasound-assisted extraction of polysaccharides from mulberry leaves. Food Chem 2011; 127: 1273-1279
- 10 Zhang DY, Wan Y, Xu JY, Wu GH, Li L, Yao XH. Ultrasound extraction of polysaccharides from mulberry leaves and their effect on enhancing antioxidant activity. Carbohydr Polym 2016; 137: 473-479
- 11 Chen X, Sheng Z, Qiu S, Yang H, Jia J, Wang J, Jiang C. Purification, characterization and in vitro and in vivo immune enhancement of polysaccharides from mulberry leaves. PLoS One 2019; 14: e0208611
- 12 Yuan Q, Xie Y, Wang W, Yan Y, Ye H, Jabbar S, Zeng X. Extraction optimization, characterization and antioxidant activity in vitro of polysaccharides from mulberry (Morus alba L.) leaves. Carbohydr Polym 2015; 128: 52-62
- 13 Xia W, Liu SQ, Zhang WQ, Luo GA. Structural features of a pectic polysaccharide from mulberry leaves. J Asian Nat Prod Res 2008; 10: 857-865
- 14 Wang H, Huang G. Extraction, purification, structural modification, activities and application of polysaccharides from different parts of mulberry. Food Funct 2024; 15: 3939-3958
- 15 Chen R, Zhou X, Deng Q, Yang M, Li S, Zhang Q, Sun Y, Chen H. Extraction, structural characterization and biological activities of polysaccharides from mulberry leaves: A review. Int J Biol Macromol 2024; 257: 128669
- 16 van Luijk J, Leenaars M, Hooijmans C, Wever K, de Vries R, Ritskes-Hoitinga M. Towards evidence-based translational research: the pros and cons of conducting systematic reviews of animal studies. ALTEX 2013; 30: 256-257
- 17 Wu SJ. Mulberry leaf polysaccharides suppress renal fibrosis. Int J Biol Macromol 2019; 124: 1090-1093
- 18 Zhang LW. Improvement Effect and Mechanism of Mulberry Leaf Active Components on Diabetes and Liver and Kidney Injury Complicated [dissertation]. Nanjing: Nanjing University of Chinese Medicine; 2019
- 19 Zhang Z, Li L, Li ZK, Wu F, Hang BY, Cai BY, Weng ZF, Zhao L, Ding CF, Du YG. Effect and mechanism of mulberry leaf polysaccharide on type 1 diabetic nephropathy in rats. Natl Med J Chin 2018; 98: 1792-1796
- 20 Zhang YW, Xue JT, Li Q, Han ZX, Liu HF. Protective effects and mechanism of mulberry leaf polysaccharide on diabetic nephropathy rats. Chin Arch Tradit Chin Med 2016; 34: 1381-1383
- 21 Huang LJ, Du YG, Sun ZJ, Zhou HM, Lv B, Shen CL, Zhao XM. Effects of mulberry leaf flavonoids and polysaccharides on serum tumor necrosis factor-α, C-reactive protein content and renal function in diabetic rats. Chin J Gerontol 2016; 36: 4703-4705
- 22 Chen JQ, Lin SJ, Zheng N. Effects of polysaccharides from mulberry leaves on diabetic nephropathy in mice. Chin J Hosp Pharm 2016; 36: 806-809
- 23 Song TJ, Li Q, Xue JT, Han ZX, Liu HF, Wang GY. Effect of mulberry leaf polysaccharide on CTGF expression in kidney of DN rats. Food Nutr Chin 2014; 20: 73-75
- 24 Liu HF, Han ZX, Nie Y, Jin LY, Wang GY, Yue H, Li Q, Xue JT, Shen MS. Effect of mulberry leaf polysaccharide on renal fibrosis in diabetic nephropathy rats. Chin J Gerontol 2014; 14: 3959-3960
- 25 Goyal SN, Reddy NM, Patil KR, Nakhate KT, Ojha S, Patil CR, Agrawal YO. Challenges and issues with streptozotocin-induced diabetes – A clinically relevant animal model to understand the diabetes pathogenesis and evaluate therapeutics. Chem Biol Interact 2016; 244: 49-63
- 26 Skyler JS. Microvascular complications. Retinopathy and nephropathy. Endocrinol Metab Clin North Am 2001; 30: 833-856
- 27 Liu CG, Ma YP, Zhang XJ. Effects of mulberry leaf polysaccharide on oxidative stress in pancreatic β-cells of type 2 diabetic rats. Eur Rev Med Pharmacol Sci 2017; 21: 2482-2488
- 28 Feng L, Chen C, Xiong X, Wang X, Li X, Kuang Q, Wei X, Gao L, Niu X, Li Q, Yang J, Li L, Luo P. PS-MPs promotes the progression of inflammation and fibrosis in diabetic nephropathy through NLRP3/Caspase-1 and TGF-β1/Smad2/3 signaling pathways. Ecotoxicol Environ Saf 2024; 273: 116102
- 29 Wang L, Wang HL, Liu TT, Lan HY. TGF-Beta as a master regulator of diabetic nephropathy. Int J Mol Sci 2021; 22: 7881
- 30 Sun Y, Ge J, Shao F, Ren Z, Huang Z, Ding Z, Dong L, Chen J, Zhang J, Zang Y. Long noncoding RNA AI662270 promotes kidney fibrosis through enhancing METTL3-mediated m(6) A modification of CTGF mRNA. FASEB J 2023; 37: e23071
- 31 Oda Y, Nishi H, Nangaku M. Role of inflammation in progression of chronic kidney disease in type 2 diabetes mellitus: Clinical implications. Semin Nephrol 2023; 43: 151431
- 32 Oh Y. The insulin-like growth factor system in chronic kidney disease: Pathophysiology and therapeutic opportunities. Kidney Res Clin Pract 2012; 31: 26-37
- 33 Mohebi R, Liu Y, Hansen MK, Yavin Y, Sattar N, Pollock CA, Butler J, Jardine M, Masson S, Heerspink HJL, Januzzi jr. JL. Insulin growth factor axis and cardio-renal risk in diabetic kidney disease: An analysis from the CREDENCE trial. Cardiovasc Diabetol 2023; 22: 176
- 34 Ren C, Zhang Y, Cui W, Lu G, Wang Y, Gao H, Huang L, Mu Z. A polysaccharide extract of mulberry leaf ameliorates hepatic glucose metabolism and insulin signaling in rats with type 2 diabetes induced by high fat-diet and streptozotocin. Int J Biol Macromol 2015; 72: 951-959
- 35 Liu HF, Ren YH, Song TJ, Han ZX. Effect of mulberry leaves polysaccharides on gene expression of resistin in type 2 diabetes mellitus rats. Food Nutr Chin 2012; 18: 67-68
- 36 Han ZX, Xue JT, Li Q, Song TJ, Wang GY, Liu HF. Effect of MLP on expression of AdipoR1 in diabetic nephropathy rats. Food Nutr Chin 2014; 20: 74-75
- 37 Hooijmans CR, Rovers MM, de Vries RB, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLEʼs risk of bias tool for animal studies. BMC Med Res Methodol 2014; 14: 43
- 38 Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Osteoarthritis Cartilage 2012; 20: 256-260
- 39 Franco A, Malhotra N, Simonovits G. Social science. Publication bias in the social sciences: Unlocking the file drawer. Science 2014; 345: 1502-1505
- 40 Brosius 3rd FC, Alpers CE, Bottinger EP, Breyer MD, Coffman TM, Gurley SB, Harris RC, Kakoki M, Kretzler M, Leiter EH, Levi M, McIndoe RA, Sharma K, Smithies O, Susztak K, Takahashi N, Takahashi T. Mouse models of diabetic nephropathy. J Am Soc Nephrol 2009; 20: 2503-2512
- 41 Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane, 2023. Accessed February 2024 at http://www.training.cochrane.org/handbook
Correspondence
Publication History
Received: 02 June 2024
Accepted after revision: 27 September 2024
Accepted Manuscript online:
02 October 2024
Article published online:
28 October 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Wen CP, Chang CH, Tsai MK, Lee JH, Lu PJ, Tsai SP, Wen C, Chen CH, Kao CW, Tsao CK, Wu X. Diabetes with early kidney involvement may shorten life expectancy by 16 years. Kidney Int 2017; 92: 388-396
- 2 ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Leon J, Lyons SK, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Gabbay RA. on behalf of the American Diabetes A. 11. Chronic kidney disease and risk management: Standards of care in diabetes-2023. Diabetes Care 2023; 46: S191-S202
- 3 Reidy K, Kang HM, Hostetter T, Susztak K. Molecular mechanisms of diabetic kidney disease. J Clin Invest 2014; 124: 2333-2340
- 4 Qu L, Liang X, Tian G, Zhang G, Wu Q, Huang X, Cui Y, Liu Y, Shen Z, Xiao C, Qin Y, Miao H, Zhang Y, Li Z, Ye S, Zhang X, Yang J, Cao G, Li Y, Yang G, Hu J, Wang X, Li Z, Li Y, Zhang X, Zhang G, Chen L, Hua W, Yu M, Lu C, Zhang X, Jiang H. Efficacy and safety of mulberry twig alkaloids tablet for the treatment of type 2 diabetes: A multicenter, randomized, double-blind, double-dummy, and parallel controlled clinical trial. Diabetes Care 2021; 44: 1324-1333
- 5 Li R, Zhou J, Zhang X, Zhang T, Wang J, Zhang M, He C, Chen H. Isolation, structural characterization and cholesterol-lowering effects of a novel polysaccharide from mulberry (Morus alba L.) leaf. Ind Crops Prod 2023; 202: 117010
- 6 Wang F, Li J, Jiang Y. Polysaccharides from mulberry leaf in relation to their antioxidant activity and antibacterial ability. J Food Process Eng 2010; 33: 39-50
- 7 Yang S, Li Y, Jia D, Yao K, Liu W. The synergy of Box-Behnken designs on the optimization of polysaccharide extraction from mulberry leaves. Ind Crops Prod 2017; 99: 70-78
- 8 Thirugnanasambandham K, Sivakumar V, Maran JP. Microwave-assisted extraction of polysaccharides from mulberry leaves. Int J Biol Macromol 2015; 72: 1-5
- 9 Ying Z, Han X, Li J. Ultrasound-assisted extraction of polysaccharides from mulberry leaves. Food Chem 2011; 127: 1273-1279
- 10 Zhang DY, Wan Y, Xu JY, Wu GH, Li L, Yao XH. Ultrasound extraction of polysaccharides from mulberry leaves and their effect on enhancing antioxidant activity. Carbohydr Polym 2016; 137: 473-479
- 11 Chen X, Sheng Z, Qiu S, Yang H, Jia J, Wang J, Jiang C. Purification, characterization and in vitro and in vivo immune enhancement of polysaccharides from mulberry leaves. PLoS One 2019; 14: e0208611
- 12 Yuan Q, Xie Y, Wang W, Yan Y, Ye H, Jabbar S, Zeng X. Extraction optimization, characterization and antioxidant activity in vitro of polysaccharides from mulberry (Morus alba L.) leaves. Carbohydr Polym 2015; 128: 52-62
- 13 Xia W, Liu SQ, Zhang WQ, Luo GA. Structural features of a pectic polysaccharide from mulberry leaves. J Asian Nat Prod Res 2008; 10: 857-865
- 14 Wang H, Huang G. Extraction, purification, structural modification, activities and application of polysaccharides from different parts of mulberry. Food Funct 2024; 15: 3939-3958
- 15 Chen R, Zhou X, Deng Q, Yang M, Li S, Zhang Q, Sun Y, Chen H. Extraction, structural characterization and biological activities of polysaccharides from mulberry leaves: A review. Int J Biol Macromol 2024; 257: 128669
- 16 van Luijk J, Leenaars M, Hooijmans C, Wever K, de Vries R, Ritskes-Hoitinga M. Towards evidence-based translational research: the pros and cons of conducting systematic reviews of animal studies. ALTEX 2013; 30: 256-257
- 17 Wu SJ. Mulberry leaf polysaccharides suppress renal fibrosis. Int J Biol Macromol 2019; 124: 1090-1093
- 18 Zhang LW. Improvement Effect and Mechanism of Mulberry Leaf Active Components on Diabetes and Liver and Kidney Injury Complicated [dissertation]. Nanjing: Nanjing University of Chinese Medicine; 2019
- 19 Zhang Z, Li L, Li ZK, Wu F, Hang BY, Cai BY, Weng ZF, Zhao L, Ding CF, Du YG. Effect and mechanism of mulberry leaf polysaccharide on type 1 diabetic nephropathy in rats. Natl Med J Chin 2018; 98: 1792-1796
- 20 Zhang YW, Xue JT, Li Q, Han ZX, Liu HF. Protective effects and mechanism of mulberry leaf polysaccharide on diabetic nephropathy rats. Chin Arch Tradit Chin Med 2016; 34: 1381-1383
- 21 Huang LJ, Du YG, Sun ZJ, Zhou HM, Lv B, Shen CL, Zhao XM. Effects of mulberry leaf flavonoids and polysaccharides on serum tumor necrosis factor-α, C-reactive protein content and renal function in diabetic rats. Chin J Gerontol 2016; 36: 4703-4705
- 22 Chen JQ, Lin SJ, Zheng N. Effects of polysaccharides from mulberry leaves on diabetic nephropathy in mice. Chin J Hosp Pharm 2016; 36: 806-809
- 23 Song TJ, Li Q, Xue JT, Han ZX, Liu HF, Wang GY. Effect of mulberry leaf polysaccharide on CTGF expression in kidney of DN rats. Food Nutr Chin 2014; 20: 73-75
- 24 Liu HF, Han ZX, Nie Y, Jin LY, Wang GY, Yue H, Li Q, Xue JT, Shen MS. Effect of mulberry leaf polysaccharide on renal fibrosis in diabetic nephropathy rats. Chin J Gerontol 2014; 14: 3959-3960
- 25 Goyal SN, Reddy NM, Patil KR, Nakhate KT, Ojha S, Patil CR, Agrawal YO. Challenges and issues with streptozotocin-induced diabetes – A clinically relevant animal model to understand the diabetes pathogenesis and evaluate therapeutics. Chem Biol Interact 2016; 244: 49-63
- 26 Skyler JS. Microvascular complications. Retinopathy and nephropathy. Endocrinol Metab Clin North Am 2001; 30: 833-856
- 27 Liu CG, Ma YP, Zhang XJ. Effects of mulberry leaf polysaccharide on oxidative stress in pancreatic β-cells of type 2 diabetic rats. Eur Rev Med Pharmacol Sci 2017; 21: 2482-2488
- 28 Feng L, Chen C, Xiong X, Wang X, Li X, Kuang Q, Wei X, Gao L, Niu X, Li Q, Yang J, Li L, Luo P. PS-MPs promotes the progression of inflammation and fibrosis in diabetic nephropathy through NLRP3/Caspase-1 and TGF-β1/Smad2/3 signaling pathways. Ecotoxicol Environ Saf 2024; 273: 116102
- 29 Wang L, Wang HL, Liu TT, Lan HY. TGF-Beta as a master regulator of diabetic nephropathy. Int J Mol Sci 2021; 22: 7881
- 30 Sun Y, Ge J, Shao F, Ren Z, Huang Z, Ding Z, Dong L, Chen J, Zhang J, Zang Y. Long noncoding RNA AI662270 promotes kidney fibrosis through enhancing METTL3-mediated m(6) A modification of CTGF mRNA. FASEB J 2023; 37: e23071
- 31 Oda Y, Nishi H, Nangaku M. Role of inflammation in progression of chronic kidney disease in type 2 diabetes mellitus: Clinical implications. Semin Nephrol 2023; 43: 151431
- 32 Oh Y. The insulin-like growth factor system in chronic kidney disease: Pathophysiology and therapeutic opportunities. Kidney Res Clin Pract 2012; 31: 26-37
- 33 Mohebi R, Liu Y, Hansen MK, Yavin Y, Sattar N, Pollock CA, Butler J, Jardine M, Masson S, Heerspink HJL, Januzzi jr. JL. Insulin growth factor axis and cardio-renal risk in diabetic kidney disease: An analysis from the CREDENCE trial. Cardiovasc Diabetol 2023; 22: 176
- 34 Ren C, Zhang Y, Cui W, Lu G, Wang Y, Gao H, Huang L, Mu Z. A polysaccharide extract of mulberry leaf ameliorates hepatic glucose metabolism and insulin signaling in rats with type 2 diabetes induced by high fat-diet and streptozotocin. Int J Biol Macromol 2015; 72: 951-959
- 35 Liu HF, Ren YH, Song TJ, Han ZX. Effect of mulberry leaves polysaccharides on gene expression of resistin in type 2 diabetes mellitus rats. Food Nutr Chin 2012; 18: 67-68
- 36 Han ZX, Xue JT, Li Q, Song TJ, Wang GY, Liu HF. Effect of MLP on expression of AdipoR1 in diabetic nephropathy rats. Food Nutr Chin 2014; 20: 74-75
- 37 Hooijmans CR, Rovers MM, de Vries RB, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLEʼs risk of bias tool for animal studies. BMC Med Res Methodol 2014; 14: 43
- 38 Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Osteoarthritis Cartilage 2012; 20: 256-260
- 39 Franco A, Malhotra N, Simonovits G. Social science. Publication bias in the social sciences: Unlocking the file drawer. Science 2014; 345: 1502-1505
- 40 Brosius 3rd FC, Alpers CE, Bottinger EP, Breyer MD, Coffman TM, Gurley SB, Harris RC, Kakoki M, Kretzler M, Leiter EH, Levi M, McIndoe RA, Sharma K, Smithies O, Susztak K, Takahashi N, Takahashi T. Mouse models of diabetic nephropathy. J Am Soc Nephrol 2009; 20: 2503-2512
- 41 Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane, 2023. Accessed February 2024 at http://www.training.cochrane.org/handbook