Subscribe to RSS
DOI: 10.1055/a-2436-7185
Current State and Outlook in Medical 3D Printing and the Role of Radiology
Article in several languages: English | deutschAuthors

Abstract
Background
Medical three-dimensional (3D) printing is playing an increasingly important role in clinical practice. The use of 3D printed models in patient care offers a wide range of possibilities in terms of personalized medicine, training and education of medical professionals, and communication with patients. DICOM files from imaging modalities such as CT and MRI provide the basis for the majority of the 3D models in medicine. The image acquisition, processing, and interpretation of these lies within the responsibility of radiology, which can therefore play a key role in the application and further development of 3D printing.
The purpose of this review article is to provide an overview of the principles of 3D printing in medicine and summarize its most important clinical applications. It highlights the role of radiology as central to developing and administering 3D models in everyday clinical practice.
Methods
This is a narrative review article on medical 3D printing that incorporates expert opinions based on the current literature and practices from our own medical centers.
Results/Conclusion
While the use of 3D printing is becoming increasingly established in many medical specialties in Germany and is finding its way into everyday clinical practice, centralized “3D printing labs” are a rarity in Germany but can be found internationally. These labs are usually managed by radiology departments, as radiology is a connecting discipline that – thanks to the imaging technology used to produce data for 3D printing – can play a leading role in the application of medical 3D printing. Copying this approach should be discussed in Germany in order to efficiently use the necessary resources and promote research and development in the future.
Key Points
-
3D printing in medicine is a rapidly growing field.
-
Image acquisition and processing provides an important basis for high-quality 3D models.
-
Radiology, as the specialist discipline responsible for imaging, has a crucial role to play.
-
Radiology should play a leading role in the introduction of 3D printing in everyday clinical practice.
Citation Format
-
Streckenbach A, Schubert N, Streckenbach F et al. Current State and Outlook in Medical 3 D Printing and the Role of Radiology. Fortschr Röntgenstr 2024; DOI 10.1055/a-2436-7185
Keywords
radiology - three-dimensional printing - 3D-print - additive manufacturing - personalized medicine - preoperative planningIntroduction
Since its advent in the 1980s, three-dimensional printing technology (3D printing) has also found its way into healthcare. Medical applications with 3D printing include patient-specific extra- and intracorporeal prostheses with complex reconstructions of the patient-specific anatomy, fabrication of models for training purposes, quality assurance, and interdisciplinary therapy planning. Applications using 3D printing of living tissue (known as bioprinting) are also already in use [1] [2].
High-quality medical 3D printing requires high-resolution diagnostic image data, and these data are collected mainly using computed tomography (CT) or magnetic resonance imaging (MRI) examinations. Radiology is playing an important role here. The discipline holds the expertise needed to both generate and administer high-resolution image data, as well as to create and post-process complex 3D models.
The following article provides an overview of the basic procedures and areas of application for 3D printing in medicine, and highlights future developments and the formative role of radiologists.
Principles of 3D printing
3D printing is an additive manufacturing process and uses a digital model to produce a physical 3D model on a layer-by-layer basis. The multi-step process of 3D printing can be divided into three main areas of activity: data collection, image processing, and the actual 3D printing.
Data collection
The data record generated from the image is used as the basis for the 3D printing manufacturing process. So it is important to take into account the relevant examination parameters prior to image acquisition for 3D printing. The parameters depend on both the examination modality selected and the intended use for the model. As a result, they can have a high degree of variability. Currently, in both CT and MRI there are standard diagnostic imaging protocols that mostly serve as the basis for 3D printing. However, to print bony structures [3] and specifically for CT or MRI-based printing of cardiac structures, special protocols are now used in clinical practice [4] [5] [6] [7].
If CT is used as the basis for 3D printing, the examinations should have a high image contrast, a high signal-to-noise ratio, and a high spatial resolution. Slice thickness of 1.25 mm or less, combined with a small field-of-view, are recommended to achieve the lowest possible voxel size [8]. Lower slice thicknesses may be necessary in individual applications, such as orbital reconstructions [9], but they also involve more post-processing. In addition, the choice of computing kernel has an impact on the spatial resolution and the image noise [10]. A bone kernel can have advantages when visualizing delicate anatomical structures, such as the temporal bone. However, due to the lower image noise compared to the bone kernel and the resulting anti-aliasing, a soft tissue kernel is often preferred [11]. Modern CT techniques, such as iterative or artificial intelligence-based techniques for reducing image noise and artifacts, can additionally improve the quality of the image data before further processing [12] [13].
For MRI-based printing of cardiovascular structures, ECG-triggered 3D balance steady-state precession and contrast-enhanced MRI angiography are the most commonly used techniques [14] [15]. This makes it possible to generate diagnostic image data that can be used for 3D printing without ionizing radiation, even in pediatric patients [4].
File formats
The internationally recognized Digital Imaging and Communications in Medicine (DICOM) format is the established standard for storing and exchanging medical image files from sonography, MRI, CT, and positron emission tomography (PET-) CT. However, it is not yet suitable for direct communication with 3D printers. These require a format that defines individual objects and surfaces that enclose the target area of a room layer by layer. Two commonly used standard file formats are standard tessellation language (STL) and object file (OBJ) format. These file formats break the surface of the target object into a series of triangles in a Cartesian coordinate system (tessellation) [16] [17]. In recent years, the additive manufacturing file format (AMF) has established itself as an advanced file format that also allows the storage of features such as surface texture, color, and material properties for a target model [18].
Image processing
In order to convert the DICOM data into a format suitable for 3D printing, the image data have to be segmented. Voxels that belong to an anatomical structure (region of interest) are assigned to a volume or a mask. This process can be carried out manually or using (semi-)automatic procedures. These include the expansion to include neighboring voxels (region growing), the definition of thresholds for assigning voxels (thresholding), or the detection of object edges (edge detection). For this purpose, the DICOM files are imported into software that is specifically engineered for segmenting and designing 3D models. It is recommended that radiologists review the results to confirm that the digital model correctly represents the anatomical structures and meets the requirements for 3D printing ([Fig. 1]).

The segmented data are then converted into a file format suitable for 3D printing. This data record is then processed further using special 3D software known as computer aided design (CAD) or computer aided manufacturing (CAM) software. This allows further adjustments and error corrections to be made specific to 3D printing. In this step, if necessary, additional support elements are added to the model to hold it in position during printing or to be able to print overhangs [19]. Some basic image processing functions, such as segmentation and conversion to other file formats for creating a model for 3D printing can now also be performed using advanced visualization software. These are specialized computer programs for processing, analyzing, and visualizing medical image data. Programs frequently mentioned in the literature are Vitrea (Canon Medical Systems Europe B.V.; Netherlands), Mimics (Materialise; Belgium) and Syngo.via (Siemens Healthineers; Germany).
Due to the complexity of 3D models and the enormous importance of the geometric accuracy of the models, especially for patient-specific implants, image processing can be very challenging. This mainly concerns the compatibility of the data, the correction of model errors, consideration of the printing materials and technologies, as well as the optimal settings for printing parameters. This process therefore requires close cooperation between the departments involved, as well as careful planning and testing of the process chain. To ensure quality, the individual work steps have to be monitored and controlled by specially qualified experts. Due to the technical demands of 3D printing, these experts are primarily material scientists and engineers. Radiologists play a crucial role in radiological imaging, its techniques, and in checking the anatomical correctness of the 3D model.
Printing the 3D model
3D printers create models from the 3D printing files, which are usually applied as successive layers of material. When choosing printing technology, other aspects must be taken into account besides the availability and cost of the printer. These include the time required for printing, the selection of materials that can be used with the respective printer, in particular, the option to print in color, biocompatibility, the sterilizability of 3D printing, the temperature and humidity resistance of the material, and the question of the need to be able to print different materials at the same time. A variety of different printing technologies have been developed in the meantime. The three basic and most commonly used methods are presented below ([Fig. 2]). An overview can be found in [Table 1].

|
Method |
Description |
Materials |
Medical application |
Device costs in EUR |
Strengths |
Weaknesses |
Spatial resolution[20] |
Printing speed |
|
Fused deposition modeling (FDM) |
Layer-by-layer extrusion of a filament/ thermoplastic |
Plastics/thermoplastics, e.g. polylactide and polyethylene terephthalate; incl. biocompatibility |
Planning and simulation models, phantoms, prostheses, spare parts |
200–100,000 |
Widely used, variety of materials & colors, cost-effective filament, simultaneous use of different materials, durability |
Rough surfaces, low resolution, tendency to distort during printing |
z-axis: 0.1–0.5 mm x-y axis: 0.1–0.4 mm |
Ø 100–200 mm/h |
|
Stereo-lithography (SLA) |
Curing of photopolymer resin under UV light |
Epoxy/synthetic resin; incl. biocompatibility |
Planning and simulation models, phantoms, dental surgery |
200–150,000 |
High resolution, supports complex models, smooth surface, variety of materials |
Post-processing required, Long printing times Does not support simultaneous use of different materials |
z-axis: 0.02–0.2 mm x-y axis: 0.075–0.2 mm |
Ø 50–100 mm/h |
|
Selective sintering (SLS) |
Sintering of a powdered substrate using laser radiation |
Polymers, metals, ceramics and others; incl. biocompatibility |
Implants, osteosyntheses, surgical instruments |
150,000–800,000 |
Durable items, variety of usable materials, production of sterilizable items, good biocompatibility |
Cost-intensive. Long printing times Does not support simultaneous use of different materials |
z-axis: 0.1–0.2 mm x-y axis: 0.075–0.2 mm |
Ø 15–20 mm/h |
Printing methods
Fused deposition modeling
Fused deposition modeling is the most widely used method of 3D printing. In this procedure, a thermoplastic polymer (solid) is extruded through a heated nozzle and then placed on a heated print bed to cool layer by layer. The models generated are easy, inexpensive, and relatively quick to create ([Table 1]). Benefits include the wide availability of thermoplastic polymers or mixtures of these and similar plastics. In addition, these materials can be combined and reinforced with other materials such as carbon fibers during the printing process [21]. This technology also allows the use simultaneously of several colors or alternating printing of different materials in the same model. For example, supporting structures can be integrated that can be dissolved water after printing is completed [22].
The disadvantage, compared to other printing techniques, is a lower spatial resolution and accuracy ([Table 1]). Therefore, FDM printing is more likely to be used in feasibility studies and in the production of cost-effective prototypes or simulation models.
Stereolithography/resin printing
Stereolithography (SLA or resin printing) uses light-sensitive, dissolved synthetic resins that are cured layer by layer using different light sources with a specific wavelength spectrum, depending on the design principle. The model is “hung upside down”, attached to a base plate, and “pulled” layer by layer from the resin reservoir. This process is called photopolymerization and provides a wide range of usable materials. It is possible to add additional filler materials such as glass fiber or carbon fiber to the synthetic resins, for example, to increase the strength or reduce the weight of the workpiece [22]. In addition, biocompatible materials can also be used to produce 3D models for extra- and intracorporeal use. The geometric accuracy and the resolution of the components created with this technique exceeds the FDM process in this regard ([Table 1]).
One of the disadvantages of SLA printing is that post-processing the components is more time-consuming, because they are usually washed with isopropyl alcohol after removal from the resin tank and then they have to be cured under UV light.
Nevertheless, stereolithography has become established in the medical field because it produces highly accurate models and the manufacturing step is relatively fast ([Table 1]).
This makes SLA printing very suitable for making prototypes of medical devices with tight geometric tolerances and smooth surfaces, as well as for functional end-user parts and detailed anatomical models [23].
Selective sintering (SLS, DMLS and SLM)
In the selective sintering process, a powdered substrate, e.g. nylon or metal powder, is fused using a high-power laser. In addition, in contrast to the other processes, no supporting structures are necessary, as the non-fused material powder surrounds and supports the 3D model during printing. A further benefit of this process is the possibility of using metallic alloys for high-strength and sterilizable components with, in some cases, excellent biocompatibility.
Disadvantages include the high acquisition costs of special printing equipment and materials. As a result, use in everyday clinical practice is still rare.
This method has been used primarily in the manufacture of implants, e.g. in trauma or tumor treatment or to make dental implants [24].
Application areas in medicine
At the start of the 21st century, 3D printers were not widely available. So their medical applications were limited. At first, they were used mainly in orthopedics and traumatology. Steady improvements in print quality have made it possible to open up new application areas in medicine. Below are examples of the most important applications from our institution’s 3D printing center.
Neurosurgery and neuroradiology
In neurosurgery and neuroradiology, cerebrovascular 3D models are used to plan complex surgical or endovascular procedures, as well as to train medical staff. As part of this process, anatomical spatial relationships, as well as special anatomical features, are visualized pre-interventionally. This means that appropriate catheter and embolization materials can be tested in advance [25] [26]. A training model of an aneurysm of the posterior communicating artery is shown in [Fig. 3] ([Fig. 3]).

In addition, 3D models can also be used to test new and innovative therapy options and to conduct comparative studies of different intervention options [27].
New treatment options are offered by 3D printing of patient-specific skull reconstructions, e.g. in the form of titanium plates, for complex traumatic defects or after tumor resection, and personalized 3D implants or osteosynthesis screws in spinal surgery [28] [29].
Oral and maxillofacial surgery
In oral and maxillofacial (OMF) surgery, 3D printing is also used for aesthetic considerations, especially for patient-specific implants, e.g. for jaw or orbital floor reconstruction ([Fig. 4]) or for creating splints in orthognathic surgery [30] [31]. In cases of congenital facial deformities or traumatic defects, the healthy opposite side of the face can serve as a mirror-image template for a side-symmetrical reconstruction using 3D models. Various complex planes are aligned on the skull model created by segmentation. The healthy side is then mirrored along a facial midline onto the traumatically altered side [32] [33].

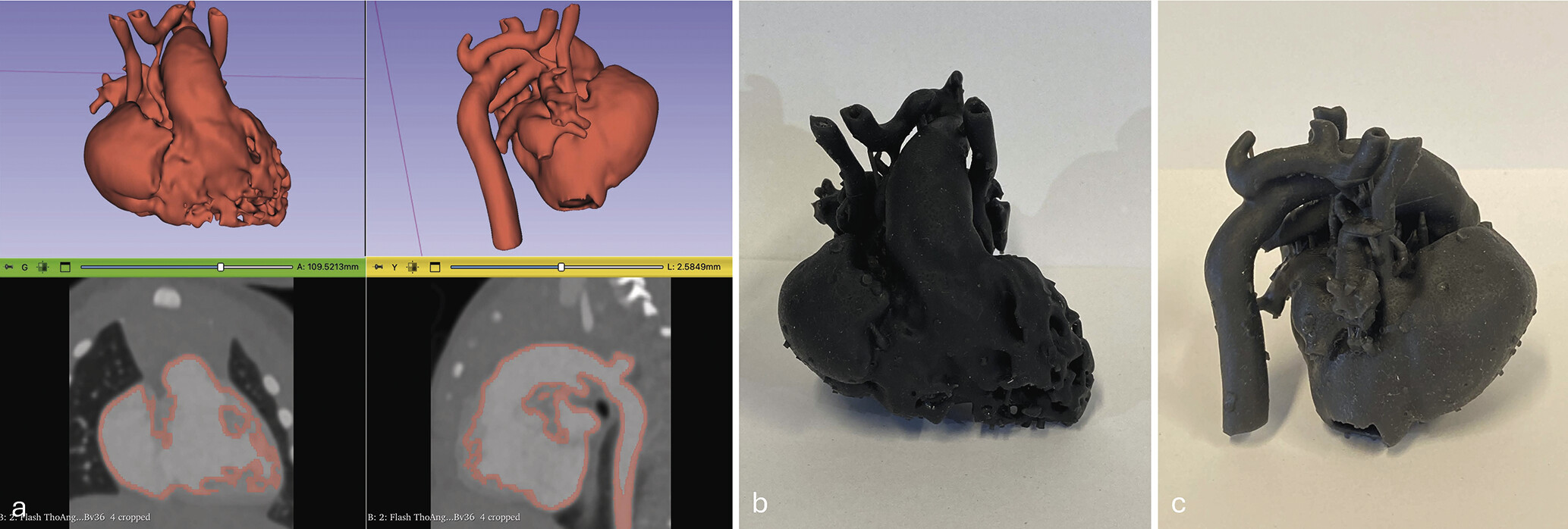
Cardiovascular surgery
In cardiovascular surgery, 3D printing is used in connection with heart diseases. It is mainly used to visualize congenital complex structural heart defects or tumor pathologies and thus to develop preoperative strategies ([Fig. 5]). Here, too, research into the production of patient-specific implants is being carried out in order to achieve, for example, improved coordination between the patient-specific anatomy and the aortic prosthesis when treating aortic aneurysms, which can lead to improved hemodynamics and consequently better long-term patency of the inlay prosthesis. [34] [35].

Musculoskeletal applications
With the 3D printing of patient-specific prostheses, orthopedics represents one of the largest sales markets in medical 3D printing. In addition, individual fastening plates, surgical osteotomy templates, and implants can be generated from 3D data [37]. Another area of application is the 3D printing of complex fractures for planning subsequent surgical treatment ([Fig. 6]) [38].

In patients with a unilateral disease, e.g. in the context of complex fractures, tumor resections, or osteotomy operations, the software can be used to mirror the normal anatomy of the unaffected side in order to obtain a 3D model for the affected side as a template for a side-symmetrical reconstruction. Even after tumor resection, 3D models can be used for the precise cutting of transplants to cover resection defects [39].
Radiotherapy
There is an increasing use of 3D printing in radiotherapy to produce phantoms for radiation planning, quality assurance, and research. One example of this is the mouse phantoms made with SLA that are used in preclinical radiation planning ([Fig. 7]). This application helps to ensure the quality of the procedures and training of staff, and it leads long term to fewer experimental animals [40]. In addition, 3D printing can be used to create anatomical molds for phantoms that can be used in multiple disciplines [41]. Indirect manufacturing has the benefit of being able to use not only printing materials but also a wide range of fabric-equivalent materials. In addition, the successful 3D printing of applicators for brachytherapy was also described [42].

Bioprinting
Bioprinting describes a 3D printing process in which cells, growth factors, and biomaterials are used as printing materials [43]. The biostructures created in this way can replace parts of organs or even entire organs with increasing complexity.
Bioprinting now allows the printing of skin substitutes, which are used, for example, to treat burn victims. In special procedures, printing can even be done directly on the pre-treated skin defect [44].
Personalized heart valves, which not only take individual patient morphology into account but also use bioprinting to incorporate physiologically active tissue, are another application area ([Fig. 8]) [45].

One goal of bioprinting is to print entire human organs. Only recently, the first transplantation of cardiac replacement tissue, known as cardiac patches, was carried out. Omental tissue from the peritoneum was coated with pluripotent, reprogrammed stem cells to replace functional heart tissue [48].
Future opportunities for radiology
Compared to other countries, the distribution of roles in medical 3D printing in Germany is still very heterogeneous and lies in the hands of individual, often non-radiological departments. It is not uncommon for individual departments/institutes, e.g. orthopedics and radiotherapy, to have their own 3D printer systems and work independently. However, in order to use the 3D printing methodology with its wide range of applications more efficiently and cost-effectively, it would be preferable to pool the individual expertise and resources. In the future, radiology could play a central role in the further development and implementation of 3D printing. In particular, essential steps preparing for printing are covered by radiological core competencies, such as knowledge of image acquisition, visualization, and image data processing, as well as handling image artifacts, knowledge of clinical context, and communication with requesters [20] [49].
A qualitative preliminary screening of the image data is necessary because, for example, CT image data already obtained from outpatient radiology cannot simply be used for an endoprosthetic 3D model. In the outpatient sector, the ALARA principle (as low as reasonably achievable) is often applied to examinations using X-rays as part of radiation protection, e.g. by using a tin/silver filter. This leads to higher image noise, especially in the 1 mm thin-slice reconstructions recommended for a 3D model [29] [36] [50]. In addition, in the outpatient setting, only thin-layer reconstructions in the bone kernel are often performed as standard. When creating a 3D model, a soft tissue kernel is preferable, and is usually only reconstructed in a layer thickness of 2–3 mm by default, which results in staircase artifacts [29] [36]. To create a suitable 3D model, the relevant examination often has to be repeated. For this reason, a connection to a 3D printing center would be preferable for these patients.
A high level of expertise in creating 3D renderings for 3D printing helps to ensure that sources of error are selectively avoided. For example, when creating 3D renderings, artificial smoothing of anatomical structures, such as vascular irregularities, can often occur. During segmentation and rendering, some smaller vascular branches, e.g. branches of the ophthalmic artery or anterior choroidal artery from the internal carotid artery in the head and neck area, are also automatically removed to simplify 3D printing. Whether such changes and adjustments are relevant for the respective application area, e.g. for a training course on a simulator or for patient-specific implants/stents, can only be assessed by experienced medical professionals with radiological expertise. However, radiological expertise in the field of segmentation can also be used to provide an assessment of the potential feasibility of successful 3D printing in advance, e.g. in complex neurosurgical or neuroradiological vascular interventions. For example, complex AV malformations with a small nidus are difficult to reconstruct and print in detail using the techniques currently developed.
To address such problems more efficiently, 3D printing centers with interdisciplinary structures would be useful. Particularly with regard to the challenges of imaging and as a link between the individual work steps, including quality assurance and testing, radiology can play a crucial advisory role alongside its role as strictly a service provider.
Despite the great potential for innovation, there are, in addition to legal hurdles such as liability issues, currently no medical guidelines that recommend the use of 3D printing. Furthermore, the funding of 3D printing in the clinical and outpatient sectors has not yet been regulated fully and is not currently covered by health insurance companies in Germany. For this reason, in everyday clinical practice 3D printing is primarily carried out only as part of clinical studies and, due to the high time expenditure, segmentation is often carried out by non-medical personnel and only under partial medical supervision.
Currently, both radiological and non-radiological professional societies are increasingly addressing the challenges that still exist. For example, the Society for Manufacturing Engineers (SME) has set up a working group for medical 3D printing and the Radiological Society of North America (RSNA) has established the 3D Special Interest Group (SIG) to promote education and training in this area and to advance research into the feasibility and benefits of 3D printing applications. [46] [47].
Summary
When implemented correctly, medical 3D printing promises improved personalized patient care. In addition to creating individual anatomical prostheses and models, the bioprinting approach has a promising future.
Accurate image acquisition with detailed visualization of the anatomical target region is required for 3D printing today, which is why radiological expertise is taking a central role. Because 3D printing in medicine is based largely on anatomical data, radiology is responsible for correctly acquiring and interpreting this information. As a result, it is playing a key role in the production of medical 3D models.
To promote the integration of 3D printing in everyday medical practice in German-speaking countries and to expand research in this field, it would make sense to create a central organizational structure to manage resources from a range of different disciplines. As a hub for the many 3D printing steps in medicine, radiology holds an ideal central position, and it can play an increasingly cross-disciplinary, networking role to support medical colleagues, as well as supporting the design and engineering sectors in ways beyond image interpretation.
Despite current legal obstacles and a lack of funding, as well as its lack of consideration in medical guidelines, 3D printing is already widely used and offers opportunities for future developments in medicine.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Herzog J, Franke L, Lai Y. et al. 3D bioprinting of microorganisms: principles and applications. Bioprocess Biosyst Eng 2024; 47: 443-461
- 2 Sekar MP, Suresh S, Zennifer A. et al. Hyaluronic Acid as Bioink and Hydrogel Scaffolds for Tissue Engineering Applications. ACS Biomater Sci Eng 2023; 9: 3134-3159
- 3 van Eijnatten M, van Dijk R, Dobbe J. et al. CT image segmentation methods for bone used in medical additive manufacturing. Med Eng Phys 2018; 51: 6-16
- 4 Hussain T, Lossnitzer D, Bellsham-Revell H. et al. Three-dimensional dual-phase whole-heart MR imaging: Clinical implications for congenital heart disease. Radiology 2012; 263: 547-554
- 5 Well L, Weinrich JM, Meyer M. et al. Sensitivity of high-pitch dual-source computed tomography for the detection of anomalous pulmonary venous connection in infants. Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgeb. Verfahren 2021; 193: 551-558
- 6 Hussain T, Mathur S, Peel SA. et al. Coronary artery size and origin imaging in children: A comparative study of MRI and trans-thoracic echocardiography. BMC Med Imaging 2015; 15: 48
- 7 Byrne N, Velasco Forte M, Tandon A. et al. A systematic review of image segmentation methodology, used in the additive manufacture of patient-specific 3D printed models of the cardiovascular system. JRSM Cardiovasc Dis 2016; 5: 2048004016645467
- 8 Mahesh M. The AAPM/RSNA physics tutorial for residents: Search for isotropie resolution in CT from conventional through multiple-row detector. Radiographics 2002; 22: 949-962
- 9 Kozakiewicz M, Elgalal M, Loba P. et al. Clinical application of 3D pre-bent titanium implants for orbital floor fractures. J Craniomaxillofac Surg 2009; 37: 229-234
- 10 Boedeker KL, Cooper VN, McNitt-Gray MF. Application of the noise power spectrum in modern diagnostic MDCT: Part I. Measurement of noise power spectra and noise equivalent quanta. Phys Med Biol 2007; 52: 4027-4046
- 11 Leng S, McGee K, Morris J. et al. Anatomic modeling using 3D printing: Quality assurance and optimization. 3D Print Med 2017; 3: 6
- 12 McCollough CH, Leng S, Yu L. et al. Dual- and multi-energy CT: Principles, technical approaches, and clinical applications. Radiology 2015; 276: 637-653
- 13 Marcus RP, Morris JM, Matsumoto JM. et al. Implementation of iterative metal artifact reduction in the pre-planning-procedure of three-dimensional physical modeling. 3D Print Med 2017; 3: 5
- 14 Velasco Forte MN, Byrne N, Valverde I Perez. et al. 3D printed models in patients with coronary artery fistulae: Anatomical assessment and interventional planning. EuroIntervention 2017; 13: e1080-e1083
- 15 Velasco Forte MN, Byrne N, Valverde I. et al. Interventional Correction of Sinus Venosus Atrial Septal Defect and Partial Anomalous Pulmonary Venous Drainage: Procedural Planning Using 3D Printed Models. JACC Cardiovasc Imaging 2018; 11: 275-278
- 16 Haleem A, Javaid M, Suman R. et al. 3D Printing Applications for Radiology: An Overview. Indian J Radiol Imaging 2021; 31: 10-17
- 17 Kamio T, Suzuki M, Asaumi R. et al. DICOM segmentation and STL creation for 3D printing: A process and software package comparison for osseous anatomy. 3D Print Med 2020; 6: 17
- 18 Hiller JD, Lipson H. STL 2.0: A proposal for a universal multi-material Additive Manufacturing File format. 20th Annu. Int. Solid Free. Fabr. Symp. SFF 2009 2009; 266-278
- 19 Gardiner JD, Behnsen J, Brassey CA. Alpha shapes: Determining 3D shape complexity across morphologically diverse structures. BMC Evol Biol 2018; 18: 184
- 20 Rischen R, Jürgensen L, Schulze M. Erratum: Medizinischer 3D-Druck und die Rolle der Radiologie. Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgeb. Verfahren 2022; 194: e1-e1
- 21 Wickramasinghe S, Do T, Tran P. FDM-Based 3D printing of polymer and associated composite: A review on mechanical properties, defects and treatments. Polymers (Basel) 2020; 12: 1529
- 22 Gurr M, Mülhaupt R. 8.04 – Rapid Prototyping. Polymer Science: A Comprehensive Reference 2012; 8: 77-99
- 23 Pravdivtseva MS, Peschke E, Lindner T. et al. 3D-printed, patient-specific intracranial aneurysm models: From clinical data to flow experiments with endovascular devices. Med Phys 2021; 48: 1469-1484
- 24 Li Z, Wang Q, Liu G. A Review of 3D Printed Bone Implants. Micromachines (Basel) 2022; 13: 528
- 25 Kono K, Shintani A, Okada H. et al. Preoperative simulations of endovascular treatment for a cerebral aneurysm using a patient-specific vascular silicone model. Neurol Med Chir (Tokyo) 2013; 53: 347-351
- 26 Waran V, Devaraj P, Hari Chandran T. et al. Three-dimensional anatomical accuracy of cranial models created by rapid prototyping techniques validated using a neuronavigation station. J Clin Neurosci 2012; 19: 574-577
- 27 Paetow H, Streckenbach F, Brandt-Wunderlich C. et al. Development of a bioresorbable self-expanding microstent for interventional applications – An innovative approach for stent-assisted coiling. Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgeb. Verfahren 2024; 196: 714-725
- 28 Pucci JU, Christophe BR, Sisti JA. et al. Three-dimensional printing: Technologies, applications, and limitations in neurosurgery. Biotechnol Adv 2017; 35: 521-529
- 29 Habib A, Jovanovich N, Muthiah N. et al. 3D printing applications in spine surgery: An evidence-based assessment toward personalized patient care. Eur Spine J 2022; 31: 1682-1690
- 30 Lee YC, Kim SG. Redefining precision and efficiency in orthognathic surgery through virtual surgical planning and 3D printing: A narrative review. Maxillofac Plast Reconstr Surg 2023; 45: 42
- 31 Zoabi A, Redenski I, Oren D. et al. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. J Clin Med 2022; 11: 2385
- 32 Hsieh TY, Dedhia R, Cervenka B. et al. 3D Printing: Current use in facial plastic and reconstructive surgery. Curr Opin Otolaryngol Head Neck Surg 2017; 25: 291-299
- 33 Nyberg EL, Farris AL, Hung BP. et al. 3D-Printing Technologies for Craniofacial Rehabilitation, Reconstruction, and Regeneration. Ann Biomed Eng 2017; 45: 45-57
- 34 Shabbak A, Masoumkhani F, Fallah A. et al. 3D Printing for Cardiovascular Surgery and Intervention: A Review Article. Curr Probl Cardiol 2024; 49: 102086
- 35 Verghi E, Catanese V, Nenna A. et al. 3D Printing in Cardiovascular Disease: Current Applications and Future Perspectives. Surg Technol Int 2021; 38: 314-324
- 36 Shah D, Naik L, Paunipagar B. et al. Setting Up 3D Printing Services for Orthopaedic Applications: A Step-by-Step Guide and an Overview of 3DBioSphere. Indian J Orthop 2020; 54: 217-227
- 37 Du H, Tian XX, Li T Sen. et al. Use of patient-specific templates in hip resurfacing arthroplasty: Experience from sixteen cases. Int Orthop 2013; 37: 777-782
- 38 Dust T, Hartel MJ, Henneberg JE. et al. The influence of 3D printing on inter- and intrarater reliability on the classification of tibial plateau fractures. Eur J Trauma Emerg Surg 2023; 49: 189-199
- 39 Bellanova L, Paul L, Docquier PL. Surgical guides (Patient-Specific Instruments) for pediatric tibial bone sarcoma resection and allograft reconstruction. Sarcoma 2013; 2013: 787653
- 40 Wegner M, Frenzel T, Krause D. et al. Development and characterization of modular mouse phantoms for end-to-end testing and training in radiobiology experiments. Phys Med Biol 2023; 68
- 41 Wegner M, Gargioni E, Krause D. Indirectly additive manufactured deformable bladder model for a pelvic radiotherapy phantom. Transactions on Additive Manufacturing Meets Medicine 2021; 3: 498
- 42 Sands G, Clark CH, McGarry CK. A review of 3D printing utilisation in radiotherapy in the United Kingdom and Republic of Ireland. Physica Medica 2023; 115: 103143
- 43 Santoni S, Gugliandolo SG, Sponchioni M. et al. 3D bioprinting: Current status and trends—a guide to the literature and industrial practice. Bio-des. Manuf 2022; 5: 14-42
- 44 Zhu W, Ma X, Gou M. et al. 3D printing of functional biomaterials for tissue engineering. Curr Opin Biotechnol 2016; 40: 103-112
- 45 Bhandari S, Yadav V, Ishaq A. et al. Trends and Challenges in the Development of 3D-Printed Heart Valves and Other Cardiac Implants: A Review of Current Advances. Cureus 2023; 15: e43204
- 46 SME Medical Additive Manufacturing/3D Printing Workgroup. Society for Manufacturing Engineers website. Accessed January 30, 2024 at: https://www.sme.org/medical-am3dp-workgroup
- 47 RSNA 3D Printing Special Interest Group. Radiological Society of North America website. Accessed November 13, 2023 at: https://www.rsna.org
- 48 Edri R, Gal I, Noor N. et al. Personalized Hydrogels for Engineering Diverse Fully Autologous Tissue Implants. Adv Mater 2019; 31: e1803895
- 49 Trace AP, Ortiz D, Deal A. et al. Radiology’s Emerging Role in 3D Printing Applications in Health Care. J Am Coll Radiol 2016; 13: 856-862.e4
- 50 Ogden KM, Aslan C, Ordway N. et al. Factors Affecting Dimensional Accuracy of 3-D Printed Anatomical Structures Derived from CT Data. J Digit Imaging 2015; 28: 654-63
Correspondence
Publication History
Received: 29 March 2024
Accepted after revision: 28 September 2024
Article published online:
30 October 2024
© 2024. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Herzog J, Franke L, Lai Y. et al. 3D bioprinting of microorganisms: principles and applications. Bioprocess Biosyst Eng 2024; 47: 443-461
- 2 Sekar MP, Suresh S, Zennifer A. et al. Hyaluronic Acid as Bioink and Hydrogel Scaffolds for Tissue Engineering Applications. ACS Biomater Sci Eng 2023; 9: 3134-3159
- 3 van Eijnatten M, van Dijk R, Dobbe J. et al. CT image segmentation methods for bone used in medical additive manufacturing. Med Eng Phys 2018; 51: 6-16
- 4 Hussain T, Lossnitzer D, Bellsham-Revell H. et al. Three-dimensional dual-phase whole-heart MR imaging: Clinical implications for congenital heart disease. Radiology 2012; 263: 547-554
- 5 Well L, Weinrich JM, Meyer M. et al. Sensitivity of high-pitch dual-source computed tomography for the detection of anomalous pulmonary venous connection in infants. Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgeb. Verfahren 2021; 193: 551-558
- 6 Hussain T, Mathur S, Peel SA. et al. Coronary artery size and origin imaging in children: A comparative study of MRI and trans-thoracic echocardiography. BMC Med Imaging 2015; 15: 48
- 7 Byrne N, Velasco Forte M, Tandon A. et al. A systematic review of image segmentation methodology, used in the additive manufacture of patient-specific 3D printed models of the cardiovascular system. JRSM Cardiovasc Dis 2016; 5: 2048004016645467
- 8 Mahesh M. The AAPM/RSNA physics tutorial for residents: Search for isotropie resolution in CT from conventional through multiple-row detector. Radiographics 2002; 22: 949-962
- 9 Kozakiewicz M, Elgalal M, Loba P. et al. Clinical application of 3D pre-bent titanium implants for orbital floor fractures. J Craniomaxillofac Surg 2009; 37: 229-234
- 10 Boedeker KL, Cooper VN, McNitt-Gray MF. Application of the noise power spectrum in modern diagnostic MDCT: Part I. Measurement of noise power spectra and noise equivalent quanta. Phys Med Biol 2007; 52: 4027-4046
- 11 Leng S, McGee K, Morris J. et al. Anatomic modeling using 3D printing: Quality assurance and optimization. 3D Print Med 2017; 3: 6
- 12 McCollough CH, Leng S, Yu L. et al. Dual- and multi-energy CT: Principles, technical approaches, and clinical applications. Radiology 2015; 276: 637-653
- 13 Marcus RP, Morris JM, Matsumoto JM. et al. Implementation of iterative metal artifact reduction in the pre-planning-procedure of three-dimensional physical modeling. 3D Print Med 2017; 3: 5
- 14 Velasco Forte MN, Byrne N, Valverde I Perez. et al. 3D printed models in patients with coronary artery fistulae: Anatomical assessment and interventional planning. EuroIntervention 2017; 13: e1080-e1083
- 15 Velasco Forte MN, Byrne N, Valverde I. et al. Interventional Correction of Sinus Venosus Atrial Septal Defect and Partial Anomalous Pulmonary Venous Drainage: Procedural Planning Using 3D Printed Models. JACC Cardiovasc Imaging 2018; 11: 275-278
- 16 Haleem A, Javaid M, Suman R. et al. 3D Printing Applications for Radiology: An Overview. Indian J Radiol Imaging 2021; 31: 10-17
- 17 Kamio T, Suzuki M, Asaumi R. et al. DICOM segmentation and STL creation for 3D printing: A process and software package comparison for osseous anatomy. 3D Print Med 2020; 6: 17
- 18 Hiller JD, Lipson H. STL 2.0: A proposal for a universal multi-material Additive Manufacturing File format. 20th Annu. Int. Solid Free. Fabr. Symp. SFF 2009 2009; 266-278
- 19 Gardiner JD, Behnsen J, Brassey CA. Alpha shapes: Determining 3D shape complexity across morphologically diverse structures. BMC Evol Biol 2018; 18: 184
- 20 Rischen R, Jürgensen L, Schulze M. Erratum: Medizinischer 3D-Druck und die Rolle der Radiologie. Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgeb. Verfahren 2022; 194: e1-e1
- 21 Wickramasinghe S, Do T, Tran P. FDM-Based 3D printing of polymer and associated composite: A review on mechanical properties, defects and treatments. Polymers (Basel) 2020; 12: 1529
- 22 Gurr M, Mülhaupt R. 8.04 – Rapid Prototyping. Polymer Science: A Comprehensive Reference 2012; 8: 77-99
- 23 Pravdivtseva MS, Peschke E, Lindner T. et al. 3D-printed, patient-specific intracranial aneurysm models: From clinical data to flow experiments with endovascular devices. Med Phys 2021; 48: 1469-1484
- 24 Li Z, Wang Q, Liu G. A Review of 3D Printed Bone Implants. Micromachines (Basel) 2022; 13: 528
- 25 Kono K, Shintani A, Okada H. et al. Preoperative simulations of endovascular treatment for a cerebral aneurysm using a patient-specific vascular silicone model. Neurol Med Chir (Tokyo) 2013; 53: 347-351
- 26 Waran V, Devaraj P, Hari Chandran T. et al. Three-dimensional anatomical accuracy of cranial models created by rapid prototyping techniques validated using a neuronavigation station. J Clin Neurosci 2012; 19: 574-577
- 27 Paetow H, Streckenbach F, Brandt-Wunderlich C. et al. Development of a bioresorbable self-expanding microstent for interventional applications – An innovative approach for stent-assisted coiling. Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgeb. Verfahren 2024; 196: 714-725
- 28 Pucci JU, Christophe BR, Sisti JA. et al. Three-dimensional printing: Technologies, applications, and limitations in neurosurgery. Biotechnol Adv 2017; 35: 521-529
- 29 Habib A, Jovanovich N, Muthiah N. et al. 3D printing applications in spine surgery: An evidence-based assessment toward personalized patient care. Eur Spine J 2022; 31: 1682-1690
- 30 Lee YC, Kim SG. Redefining precision and efficiency in orthognathic surgery through virtual surgical planning and 3D printing: A narrative review. Maxillofac Plast Reconstr Surg 2023; 45: 42
- 31 Zoabi A, Redenski I, Oren D. et al. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. J Clin Med 2022; 11: 2385
- 32 Hsieh TY, Dedhia R, Cervenka B. et al. 3D Printing: Current use in facial plastic and reconstructive surgery. Curr Opin Otolaryngol Head Neck Surg 2017; 25: 291-299
- 33 Nyberg EL, Farris AL, Hung BP. et al. 3D-Printing Technologies for Craniofacial Rehabilitation, Reconstruction, and Regeneration. Ann Biomed Eng 2017; 45: 45-57
- 34 Shabbak A, Masoumkhani F, Fallah A. et al. 3D Printing for Cardiovascular Surgery and Intervention: A Review Article. Curr Probl Cardiol 2024; 49: 102086
- 35 Verghi E, Catanese V, Nenna A. et al. 3D Printing in Cardiovascular Disease: Current Applications and Future Perspectives. Surg Technol Int 2021; 38: 314-324
- 36 Shah D, Naik L, Paunipagar B. et al. Setting Up 3D Printing Services for Orthopaedic Applications: A Step-by-Step Guide and an Overview of 3DBioSphere. Indian J Orthop 2020; 54: 217-227
- 37 Du H, Tian XX, Li T Sen. et al. Use of patient-specific templates in hip resurfacing arthroplasty: Experience from sixteen cases. Int Orthop 2013; 37: 777-782
- 38 Dust T, Hartel MJ, Henneberg JE. et al. The influence of 3D printing on inter- and intrarater reliability on the classification of tibial plateau fractures. Eur J Trauma Emerg Surg 2023; 49: 189-199
- 39 Bellanova L, Paul L, Docquier PL. Surgical guides (Patient-Specific Instruments) for pediatric tibial bone sarcoma resection and allograft reconstruction. Sarcoma 2013; 2013: 787653
- 40 Wegner M, Frenzel T, Krause D. et al. Development and characterization of modular mouse phantoms for end-to-end testing and training in radiobiology experiments. Phys Med Biol 2023; 68
- 41 Wegner M, Gargioni E, Krause D. Indirectly additive manufactured deformable bladder model for a pelvic radiotherapy phantom. Transactions on Additive Manufacturing Meets Medicine 2021; 3: 498
- 42 Sands G, Clark CH, McGarry CK. A review of 3D printing utilisation in radiotherapy in the United Kingdom and Republic of Ireland. Physica Medica 2023; 115: 103143
- 43 Santoni S, Gugliandolo SG, Sponchioni M. et al. 3D bioprinting: Current status and trends—a guide to the literature and industrial practice. Bio-des. Manuf 2022; 5: 14-42
- 44 Zhu W, Ma X, Gou M. et al. 3D printing of functional biomaterials for tissue engineering. Curr Opin Biotechnol 2016; 40: 103-112
- 45 Bhandari S, Yadav V, Ishaq A. et al. Trends and Challenges in the Development of 3D-Printed Heart Valves and Other Cardiac Implants: A Review of Current Advances. Cureus 2023; 15: e43204
- 46 SME Medical Additive Manufacturing/3D Printing Workgroup. Society for Manufacturing Engineers website. Accessed January 30, 2024 at: https://www.sme.org/medical-am3dp-workgroup
- 47 RSNA 3D Printing Special Interest Group. Radiological Society of North America website. Accessed November 13, 2023 at: https://www.rsna.org
- 48 Edri R, Gal I, Noor N. et al. Personalized Hydrogels for Engineering Diverse Fully Autologous Tissue Implants. Adv Mater 2019; 31: e1803895
- 49 Trace AP, Ortiz D, Deal A. et al. Radiology’s Emerging Role in 3D Printing Applications in Health Care. J Am Coll Radiol 2016; 13: 856-862.e4
- 50 Ogden KM, Aslan C, Ordway N. et al. Factors Affecting Dimensional Accuracy of 3-D Printed Anatomical Structures Derived from CT Data. J Digit Imaging 2015; 28: 654-63