

Subscribe to RSS
DOI: 10.1055/a-2489-4730
Women with Gynecological Cancers Receiving Specialized Ambulatory Palliative Care (SAPV)
Article in several languages: English | deutschAuthors

Abstract
Background
A dignified final phase of life spent at home is what many people with terminal cancer wish for. There are currently no studies with large datasets on the palliative care of patients with gynecological tumors in the home environment.
Material and Methods
Data from 5487 patients with gynecological-oncological disease who received specialized outpatient palliative care (SAPV) between 2017 and 2021 were included in the analysis.
Results
The analysis showed that 88.8% of the patients died in a home environment and that their symptom burden remained stable or even decreased slightly during treatment. The median duration of active SAPV was 23 days. Factors such as age, comorbidities, and symptom burden at the start of treatment influenced the survival time of patients. The SAPV team and relatives who provided care in the home environment were mostly very satisfied with the care provided.
Conclusion
The study provides important insights into the palliative care of patients with gynecological tumors and underscores the importance of SAPV for dignified end-of-life care.
Keywords
palliative care - gynecological tumors - symptom burden - specialized ambulatory palliative care (SAPV) - home environmentBackground
Most gynecological tumors are detected during screening, and curative rates have improved significantly in recent decades. However, the care of patients with terminal disease, especially female patients with extensive pelvic tumors, is still challenging and these patients require (additional) palliative care. The majority of people in Germany want to spend this final phase of life in their home environment [1]. This home environment may be the patient’s own home but can encompass their current place of residence (e.g., a care home); it must be differentiated from dying in hospital.
The German Society for Palliative Medicine (DGP) estimates that every year, up to 90% of all recently deceased persons received palliative care, which is provided by non-specialist providers. Approximately one in ten persons are estimated to require especially complex end-of-life care, also known as “specialized ambulatory palliative care” (SAPV) [2].
Previous analyses on the care provided to female patients receiving SAPV primarily differentiated between malignant and non-malignant disease [3] [4] [5] [6]. A large multicenter dataset on SAPV has permitted the targeted analysis of individual disease entities.
In this study we focused on patients with gynecological tumors and on the analysis and description of the symptom burden as well as other clinically relevant factors.
Our aim was to expand our understanding of the needs of critically ill gynecological patients receiving palliative care. We hope that this knowledge will be useful for treating gynecologists, oncologists, general practitioners and SAPV physicians. The aim is to help improve the quality of life and the self-determination of critically ill patients and allow these patients to have a dignified final stage of life in a familiar home environment which includes persons who they feel close to.
Materials and Method
Data from 22 SAPV providers who were operating in the North Rhine health insurance administrative district between 2017 and 2021 was anonymized and extracted (initially, there were 14 providers in 2017 which increased to 22 over time). Each provider was approved to offer services in a defined geographic area. According to their own projections, these 22 service providers covered around 5.7 million (60.0%) of the 9.5 million inhabitants in the health insurance administrative district of North Rhine [7].
Data sources and ethics
The patients’ data was recorded by the SAPV providers as part of their standard documentation of cases. Data extraction was coordinated by the alliance of SAPV teams for North Rhine (VSTN). All quantifiable patient information in the electronic data file was extracted in anonymized form. The merging of the data and data quality management was carried out by StatConsult, a software developer and contracted institute which carries out clinical research, development, and care research tasks. The requirements of the current version of the Helsinki Declaration were complied with. The research proposal was presented to the Ethics Commission of Witten/Herdecke University. No objections were raised (application no. 48/2023)
Participants and case definitions
The dataset includes all female patients who started treatment between 2017 and 2021. A small number of non-female persons (1.3%, most of them male) were not included in the analysis.
In most cases, SAPV is provided continuously without a break from the start of treatment until the death of the patient. But SAPV may be paused or even terminated for various reasons, for example when the patient is in hospital, transfers to a hospice or the symptom burden decreases due to the intensified care. Around one in five patients in our dataset had one or several breaks in SAPV. To include these patients in the analysis, we decided to group cases with treatment breaks of no longer than 13 days together. This was justified clinically by pointing out that short gaps in care were often the consequence of a stay in hospital for specialized procedures such as palliative chemotherapy or erythrocyte transfusions and were therefore caused by administrative requirements and not because specialized ambulatory palliative care was no longer indicated for these patients. The cut-off of 13 days was chosen on the basis of expert opinions. The decision was also underpinned by statistics, as a cut-off of 13 days allowed around 90% of cases with a break in SAPV to remain in the dataset.
Variables and statistical analysis
The aim of this study is to provide a descriptive analysis of the care of patients with gynecological tumors receiving SAPV with the help of relevant clinical endpoints:
-
Patient’s wish: to pass away in a home environment
-
Symptom control: the course of the symptom burden
-
Satisfaction: assessment of the quality of care by third parties
Tumor disease was categorized into five gynecological-oncological disease groups based on ICD-10 diagnosis (diagnosis on admission or principal diagnosis): breast cancer, uterine cancer, ovarian cancer, vulvar cancer, and vaginal cancer.
To analyze the place of death, the location was subdivided into “home environment” (hospice, respite care, retirement home and nursing home, another place of residence and at home) and “in-patient care in hospital” (acute care hospital, palliative ward). Places such as a hospice were also classed as a home environment, as it is a place of residence which is not part of the in-patient care sector where SAPV may be provided as an additional medical service. Place of death was selected as a primary outcome criterion because patients had usually chosen SAPV as their preferred type of care with this in mind. We therefore assumed that one of the characteristics of good SAPV would be that a high percentage of patients, even if not all, achieved this goal. Over the course of palliative care, a certain percentage of patients will change their preferred place of death for medical or personal reasons. This is reasonable and also desirable, in line with the concept of individualized care which focuses on quality of life.
Differences with regards to the symptom burden at the beginning and the end of sampling are presented descriptively. Missing values were imputed if values were available for more than 70% of all included cases. The SAPV services used Likert scales for the (self-)assessment of the patient’s symptom burden. If it was at all possible, the patients were asked themselves; if this was not possible, assessment was done by a qualified professional. As part of the homogenization of data, the numerical values from the assessment were grouped into the categories none/mild/moderate/severe. Differences in symptom burdens were assessed for statistical significance using McNemar’s test. As it was assumed, based on clinical experience, that patients with vulvar or vaginal cancer would spend more time in hospital due to their higher morbidity burden from wounds, we carried out a comparison of the morbidity burden at the start of treatment with regards to wounds, stratified according to vulvar/vaginal cancer yes/no. Kaplan-Meier estimates were used to show the time spent in SAPV until death. Cox regression analysis was used to show correlations between characteristics and survival time.
To additionally assess the quality of care, the variable “Satisfaction with care” was also included. To assess this, after the patient had died, a survey was done of some of the teams, and relatives and the employees who had been providing care were asked to rate their satisfaction (5-point scale: very good to very poor). The values were pooled to simplify the assessment.
Results
Categorization of the sample and place of death
Out of the total patient population of 48882 SAPV patients, 5478 (11.2%) were diagnosed with a gynecological tumor. Some of the patients had more than one diagnosis, and both tumor entities were taken into account in the analysis. The frequency distribution of gynecological tumors is given in [Table 1].
|
Tumor location |
Frequency n (%) |
|
Breast |
3638 (66.4%) |
|
Ovary |
964 (17.6%) |
|
Uterus |
779 (14.2%) |
|
Vulva |
233 (4.3%) |
|
Vagina |
41 (0.7%) |
The median patient age was 76 years (Q1–Q3: 64–84 years| min/max: 25–103 years| age < 40 years: n = 109/2%). [Table 2] lists the length of stay, place of admission and place of death as well as other patient characteristics. The median time for SAPV was 23 days and 88.8% of the patients were able to die in their chosen home environment ([Table 2]). The median number of comorbidities in the gynecological cohort was 10 (Q1–Q3: 4–12, min–max: 2–18). The age-adapted Charlson Comorbidity Index (CCI) was 9.8 (Q1–Q3: 8–12, min–max: 2–14).
122 patients (2.2%) had a secondary diagnosis of another tumor disease. The capacity of patients to care for themselves was lower at the end of SAPV than at the start ([Table 3]).
Symptom burden
Important symptom complexes in palliative medicine such as lack of appetite, vomiting, difficulty breathing, weakness, and pain are shown in diagrams 1–5, both at the beginning and at the end of care. The typical symptoms of the dying process (lack of appetite and weakness) increase towards the end of care whereas medically controllable symptoms (pain, vomiting, difficulty breathing) decrease (in terms of moderate/severe pain). These differences were statistically significant for all symptoms with the exception of vomiting (difficulty breathing, weakness, and pain [p < 0.001]; lack of appetite [p = 0.003], see also [Fig. 1]). Patients with vulvar or vaginal cancer suffered particularly often from moderate to severe wounds (59.1%) and significantly more often than patients with other gynecological tumors (22.6%). The difference was statistically highly significant (p < 0.001) ([Fig. 1]).

Survival time
A Kaplan-Meier curve showing survival times is presented in [Fig. 2].
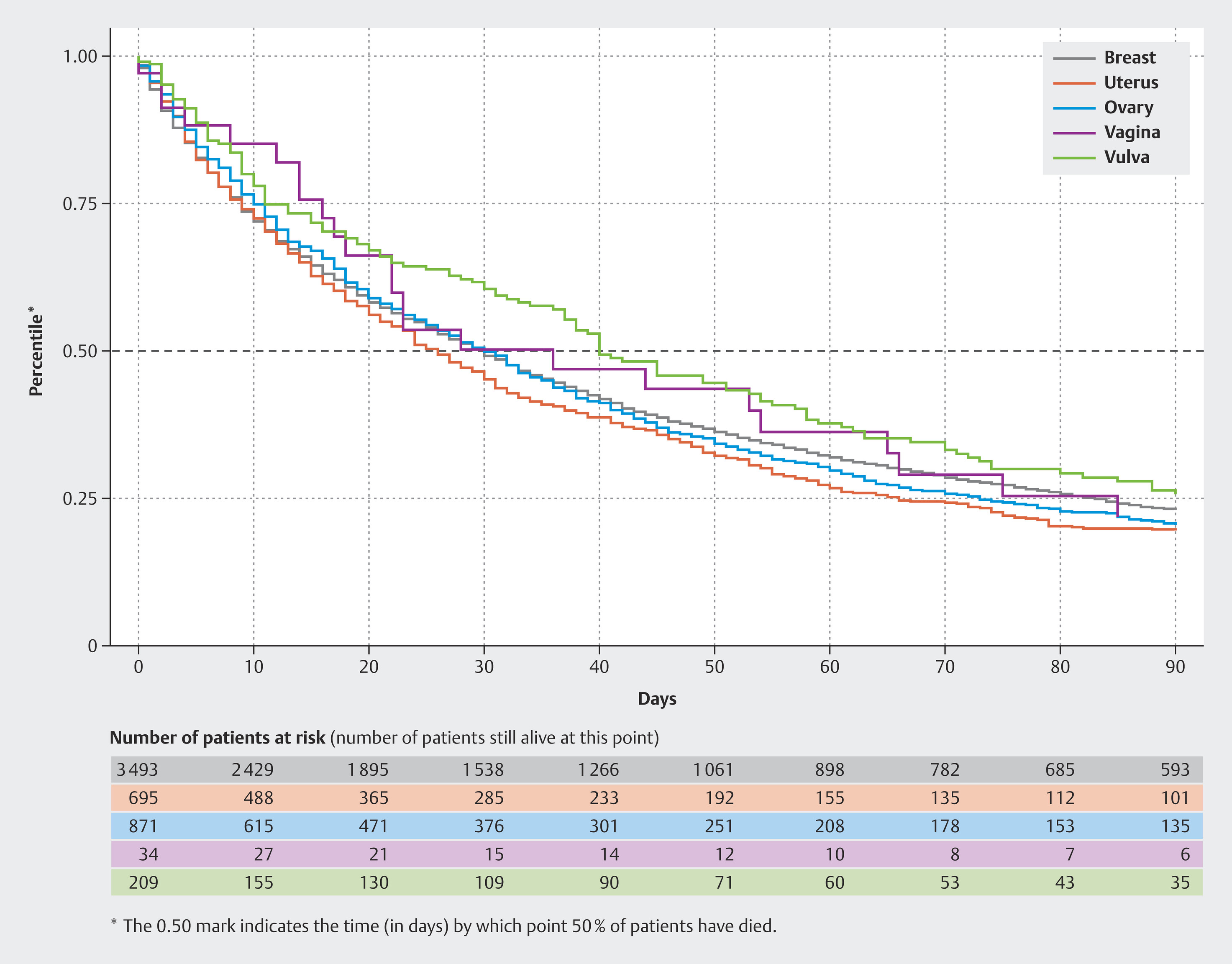
The median survival time differed according to tumor localization:
-
Breast: 30 with 95% CI (28–32)
-
Uterus: 26 with 95% CI (23–30)
-
Ovary: 30 with 95% CI (26–33)
-
Vulva: 40 with 95% CI (36–53)
-
Vagina: 36 with 95% CI (18–65)
Factors influencing survival time
Factors which influence survival time are presented using an aHR (adjusted Hazard Ratio = mortality risk). The aHR can be used to show differences between groups with regards to their probability of death. For example, if the Karnofsky Score on admission to care is 30 or less, then the HR of this group is 1.62 compared to a group with a Karnofsky Score of more than 30 and the mortality risk is therefore higher by a factor of 1.62 (or 62%). With continuous variables such as the CCI, the mortality risk increases by a factor of 1.01 for every point, in other words, by 1% [8]. An overview of the examined characteristics is shown in [Table 4].
Satisfaction of relatives with care
For quality management purposes, the patient’s relatives and the employees providing care were asked after SAPV had ended about how satisfied they were with the care that had been provided. The data on satisfaction levels (combined data from relatives and employees) were available for 71.9% of cases where SAPV had ended. Overall satisfaction was very high: 97.9% of surveyed persons rated their experience as Good or Very Good (Very Good: 75.9%, Good: 22.0%, Medium: 1.7%, Poor: 0.3%).
Discussion
Summary
This study is the first study to evaluate a large cohort of gynecological-oncology patients receiving SAPV in Germany and covers 22 SAPV care areas in the health insurance region of North Rhine.
In terms of achieving the primary goals of SAPV, which were helping patients to be able to die in a home environment and controlling/stabilizing agonizing symptoms in the last days of the patient’s life, the results were very good: 88.9% of patients died in a home environment (defined as “a place of residence” which included nursing homes and other outpatient places of residence); despite the dying process, the symptom burden remained stable and severity of symptoms even decreased slightly over the course of care. Moreover, 97.9% of surveyed persons rated their experience with the course of SAPV as “Very Good” or “Good.”
The cohort investigated in this study corresponds in terms of age and place of death to other comparable oncological SAPV cohorts [9] [10] [11].
Place of death
Our data show that a high percentage of patients with gynecological tumors were able to achieve the wish which had prompted them to request SAPV at the start of care and did not die in hospital (88.9%). This percentage was significantly higher than for the overall population: in 2017 only 27% of deaths occurred in a home environment and this percentage had been decreasing continuously since 2001 (2001: 21%; 2011: 23%) [12] [13]. In the cohort, 12.1% died in hospital or on a palliative ward. This circumstance is generally not an indication that the offer of SAPV has failed but reflects the importance of the hospital sector for the provision of palliative care in severe cases. Given the special challenges of the dying process, the patient’s preferred place of death may change over time, for example, if special medical needs arise which cannot be adequately addressed on an outpatient basis. Future studies should look into the question of the reasons which prompt a change in the preferred place to die.
It was noticeable that “nursing home” as the place of death was overrepresented in our dataset (18.3%) compared to the figure for a general oncological SAPV cohort [11]. From a clinical perspective we surmise that this difference could be explained by the fact that the patients were female. Care at home is often coordinated and supported by the patient’s spouse or live-in partner. Because of the lower life expectancy and the presumably poorer care provided by men of that generation, women are more likely to be forced to move to a nursing home as their partner is unable to provide care at home. This association should be the subject of further analysis.
Symptom burden
A positive impact was found with regards to the symptom burden of patients: medically well-treatable symptoms such as pain, difficulty breathing and nausea even decreased slightly between the start of care and dying, although clinically and in the natural course of things, a deterioration would be expected considering the progressive process of dying. That this did not occur speaks for the success of multimodal therapy during SAPV. Symptoms which are directly linked to the dying process such as weakness were more pronounced before death, a circumstance, which is to be expected in the natural process of dying. But as the differences in symptom burden are rather small overall, we interpret them as signs of a stabilization of the system through SAPV, particularly with regards to agonizing symptoms such as pain, difficulty breathing, und nausea.
Place of death
When we looked at the different gynecological tumors, the Kaplan-Meier curve showed that survival times under SAPV varied according to the gynecological tumor entity but that the overall times were similar to those of a comparable general oncological SAPV cohort [11]. Because of the clinically different courses and different symptom burdens of gynecological tumors, the significantly longer mean survival time for vaginal (36 days) and vulvar cancers (40 days) would appear to be explained by the higher symptom burden (e.g., wounds), which probably led to “earlier” admission to SAPV (admission bias). Cox regression analysis showed that comorbidities, a low Karnofsky Score, and a high symptom burden at the start of care increased the risk of early mortality. This result corresponds to the results of other analyses of oncological cohorts from this dataset [10].
Strengths and weaknesses
The strength of this study is the size of the dataset which allowed the symptom burden of persons with gynecological tumors receiving SAPV in Germany to be differentiated. The multicenter survey included 22 different service providers (around two thirds of all service providers in the North Rhine region at the time of the survey) and can therefore be described as representative for the North Rhine region. As SAPV contracts in North Rhine contain binding quality specifications for all services (billing, staffing ratios, and documentation), bias caused by a lack of data on service providers is rather unlikely. Compared to the national Germany average, a slight distortion of the data in our dataset with regards to the frequency of individual disease types is to be expected, as the utilization of SAPV varies from region to region. In the North Rhine region, 9% of all insured persons who died were receiving SAPV, which was lower than the national average for Germany of 13.1% – a circumstance which is usually explained by the well-established palliative care in North Rhine [2]. Unfortunately, it is not possible to deduce from the data how many patients did not receive SAPV despite having an indication for care and whether this led to bias. When the distribution of the different tumor entities was compared with those from the Federal Cancer Registry of the State of North Rhine-Westphalia (NRW), ovarian, vulvar, and vaginal cancers were overrepresented [14]:
-
Breast cancer, n = 3638/66.4% (Cancer Registry of NRW: 73.8%)
-
Ovarian cancer, n = 964 /17.6% (Cancer Registry of NRW: 7.7%)
-
Uterine cancer, n = 779/14.2% (Cancer Registry of NRW: 14.3%)
-
Vulvar cancer, n = 233/4.3% (Cancer Registry of NRW: 3.8%)
-
Vaginal cancer, n = 41/0.7% (Cancer Registry of NRW: 0.4%)
This circumstance could also be explained by the fact that experience has shown that these tumor entities have clinically higher symptom burdens, analogous to the above-mentioned longer survival times for vulvar and vaginal cancer.
The documentation quality of the data varies. On the one hand, these are routine clinical data, some of which were entered under time pressure and in emergency situations by different service providers. One example of this is the recording of the symptom burden. Whenever possible, assessment of the burden was done by the patient herself, but as the patient’s overall condition had increasingly deteriorated towards the end of treatment, this was often no longer possible, meaning that self-assessment of the burden was switched without further ado to assessment by relatives or care providers. On the other hand, the availability of digital terminals to collect point-of-care data, quality management instruments, and the staffing ratios of SAPV service providers are often better than in other outpatient care facilities, which is why, although the dataset may suffer from the known limitations of clinical data collection, it is probably of a high quality compared to other routinely collected data.
Summary
In relation to its declared objectives SAPV is successful: most patients were able to die at home as they had wanted; palliative medicine successfully controlled symptom complexes; and relatives and care providers reported high to very high levels of satisfaction with the care.
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgement
We would like to thank the Association of SAPV Teams from Nordrhein e.V. and all SAPV service providers who provided the data: SAPV Team NoPain Frechen, Gesundheitsnetzwerk Leverkusen, HomeCare Viersen, SAPV Wesel rechtsrheinisch, SAPV Wuppertal, SAPV Oberberg, SAPV Krefeld, SAPV Team Solingen, HomeCare Aachen, Palliative Care Team Düsseldorf, Palliative Care Duisburg, Palliativteam SAPV Rhein-Erft, SAPV Niederrhein UG, Palliativteam SAPV Köln Rheinisch-Bergischer Kreis, Palliativteam SAPV Köln linksrheinisch, Palliativteam SAPV Köln, Palliativnetzwerk Niederrhein, Palliativteam Oberhausen, Palliativnetzwerk Rhein-Maas. This study was produced in the context of the doctoral thesis of Katharina Ladermann.
-
References/Literatur
- 1 Dasch B, Zahn PK. Place of Death Trends and Utilization of Outpatient Palliative Care at the End of Life—Analysis of Death Certificates (2001, 2011, 2017) and Pseudonymized Data From Selected Palliative Medicine Consultation Services (2017) in Westphalia, Germany. Dtsch Arztebl Int 2021; 118: 331-338
- 2 Ditscheid B, Krause M, Lehmann T. et al. [Palliative care at the end of life in Germany: Utilization and regional distribution]. Bundesgesundheitsbl 2020; 63: 1502-1510
- 3 Geist M, Keßler J, Bardenheuer H. Analyse der medizinischen Versorgung onkologischer und nichtonkologischer Palliativpatienten in der spezialisierten ambulanten Palliativversorgung (SAPV). Z Palliativmedizin 2018; 19: 149-155
- 4 Kratel U. Fortschritte in der ambulanten Palliative Care-Versorgung in Deutschland − Eine Bestandsaufnahme. Dtsch Z Onkol 2014; 46: 8-15
- 5 Weckbecker K, Puth M-T, Just J. et al. [Specialized Outpatient Palliative Care: Results of a Cross-Sectional Study]. Gesundheitswesen 2021; 83: 993-997
- 6 Just J, Schmitz M-T, Grabenhorst U. et al. Factors influencing length of survival in ambulatory palliative care – a cross sectional study based on secondary data. BMC Palliat Care 2021; 20: 1-9
- 7 Statistik NRW. Webseite: Sterblichkeitsstatistik NRW. Accessed September 02, 2024 at: https://statistik.nrw/gesellschaft-und-staat/gebiet-und-bevoelkerung/geburten-und-sterbefaelle/lebendgeborene-und-gestorbene
- 8 Zwiener I, Blettner M, Hommel G. Survival Analysis. Dtsch Arztebl Int 2011; 108: 163-169
- 9 Geist M, Keßler J, Bardenheuer H. Analyse der medizinischen Versorgung onkologischer und nichtonkologischer Palliativpatienten in der spezialisierten ambulanten Palliativversorgung (SAPV). Z Palliativmedizin 2018; 19: 149-155
- 10 Just J, Schmitz M-T, Grabenhorst U. et al. Factors influencing length of survival in ambulatory palliative care – a cross sectional study based on secondary data. BMC Palliat Care 2021; 20: 1-9
- 11 Just J, Schmitz M-T, Grabenhorst U. et al. Specialized Outpatient Palliative Care—Clinical Course and Predictors for Living at Home Until Death. Dtsch Arztebl Int 2022; 119: 327-332
- 12 Dasch B, Blum K, Gude P. et al. Place of Death: Trends Over the Course of a Decade: A Population-Based Study of Death Certificates From the Years 2001 and 2011. Dtsch Arztebl Int 2015; 112: 496-504
- 13 Dasch B, Zahn PK. Place of Death Trends and Utilization of Outpatient Palliative Care at the End of Life—Analysis of Death Certificates (2001, 2011, 2017) and Pseudonymized Data From Selected Palliative Medicine Consultation Services (2017) in Westphalia, Germany. Dtsch Arztebl Int 2021; 118: 331-338
- 14 Landeskrebsregister NRW. Jahresinzidenz. Accessed September 02, 2024 at: https://www.landeskrebsregister.nrw/online-jahresbericht/%23/tables/incidence
Correspondence
Publication History
Received: 23 September 2024
Accepted after revision: 22 November 2024
Article published online:
23 January 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References/Literatur
- 1 Dasch B, Zahn PK. Place of Death Trends and Utilization of Outpatient Palliative Care at the End of Life—Analysis of Death Certificates (2001, 2011, 2017) and Pseudonymized Data From Selected Palliative Medicine Consultation Services (2017) in Westphalia, Germany. Dtsch Arztebl Int 2021; 118: 331-338
- 2 Ditscheid B, Krause M, Lehmann T. et al. [Palliative care at the end of life in Germany: Utilization and regional distribution]. Bundesgesundheitsbl 2020; 63: 1502-1510
- 3 Geist M, Keßler J, Bardenheuer H. Analyse der medizinischen Versorgung onkologischer und nichtonkologischer Palliativpatienten in der spezialisierten ambulanten Palliativversorgung (SAPV). Z Palliativmedizin 2018; 19: 149-155
- 4 Kratel U. Fortschritte in der ambulanten Palliative Care-Versorgung in Deutschland − Eine Bestandsaufnahme. Dtsch Z Onkol 2014; 46: 8-15
- 5 Weckbecker K, Puth M-T, Just J. et al. [Specialized Outpatient Palliative Care: Results of a Cross-Sectional Study]. Gesundheitswesen 2021; 83: 993-997
- 6 Just J, Schmitz M-T, Grabenhorst U. et al. Factors influencing length of survival in ambulatory palliative care – a cross sectional study based on secondary data. BMC Palliat Care 2021; 20: 1-9
- 7 Statistik NRW. Webseite: Sterblichkeitsstatistik NRW. Accessed September 02, 2024 at: https://statistik.nrw/gesellschaft-und-staat/gebiet-und-bevoelkerung/geburten-und-sterbefaelle/lebendgeborene-und-gestorbene
- 8 Zwiener I, Blettner M, Hommel G. Survival Analysis. Dtsch Arztebl Int 2011; 108: 163-169
- 9 Geist M, Keßler J, Bardenheuer H. Analyse der medizinischen Versorgung onkologischer und nichtonkologischer Palliativpatienten in der spezialisierten ambulanten Palliativversorgung (SAPV). Z Palliativmedizin 2018; 19: 149-155
- 10 Just J, Schmitz M-T, Grabenhorst U. et al. Factors influencing length of survival in ambulatory palliative care – a cross sectional study based on secondary data. BMC Palliat Care 2021; 20: 1-9
- 11 Just J, Schmitz M-T, Grabenhorst U. et al. Specialized Outpatient Palliative Care—Clinical Course and Predictors for Living at Home Until Death. Dtsch Arztebl Int 2022; 119: 327-332
- 12 Dasch B, Blum K, Gude P. et al. Place of Death: Trends Over the Course of a Decade: A Population-Based Study of Death Certificates From the Years 2001 and 2011. Dtsch Arztebl Int 2015; 112: 496-504
- 13 Dasch B, Zahn PK. Place of Death Trends and Utilization of Outpatient Palliative Care at the End of Life—Analysis of Death Certificates (2001, 2011, 2017) and Pseudonymized Data From Selected Palliative Medicine Consultation Services (2017) in Westphalia, Germany. Dtsch Arztebl Int 2021; 118: 331-338
- 14 Landeskrebsregister NRW. Jahresinzidenz. Accessed September 02, 2024 at: https://www.landeskrebsregister.nrw/online-jahresbericht/%23/tables/incidence

