

Subscribe to RSS
DOI: 10.1055/a-2517-8263
(Digital) Mind-Body Intervention to Promote Health and Subjective Well-Being of Residents in Nursing Homes: A Cluster-Randomized Controlled Pilot Study
(Digitale) Mind-Body Intervention zur Förderung der Gesundheit und des subjektiven Wohlbefindens von Bewohnenden in Pflegeeinrichtungen: Eine cluster-randomisierte kontrollierte PilotstudieAuthors

Abstract
Background
Nursing care insurance companies in Germany have the legal mandate to develop measures to strengthen the health resources of residents of nursing homes. The present study aimed to examine a mindfulness-informed mind-body intervention (on-site and app) adapted for residents in nursing homes regarding their effect on health-related parameters.
Methods
A pilot study (DRKS00030409) was carried out with three groups in twelve nursing homes (RCT). There was an on-site intervention in a group (O), an individual app application with technical support (A) and a passive control group (C). The participating residents (nO=28; nA=29; nC=19) were cluster-randomized. Before, after, and three months after the intervention period (December 2022 – January 2023), among other things, subjective well-being (WHO-5, primary outcome) and mindfulness (KIMS-D, including four subscales) were assessed. Differences within and between study groups and participants with different participation intensity were tested. In addition, a sensitivity analysis was carried out with people who did not have severe cognitive impairments at all three survey times.
Results
Indications of differences were found in subjective well-being during the intervention period between the study groups of medium size. While a decrease was observed in the control group, there was no change in the intervention groups. When the intensity of participation was taken into account, the difference between the groups became clearer. In addition, the app group showed an increase in mindfulness (subscale Observing) immediately after the intervention compared to the control group.
Conclusion
Although further studies with larger samples are needed, the results already indicate that the intervention improves the well-being and mindfulness of the target group. Individual support could explain the higher effectiveness in the app group. The influence of the Covid-19 pandemic and the season (winter) on effectiveness must also be examined.
Zusammenfassung
Hintergrund
Pflegeversicherungen in Deutschland haben den gesetzlichen Auftrag, Maßnahmenvorschläge zur Stärkung von Gesundheitsressourcen der Bewohnenden in stationären Pflegeeinrichtungen zu entwickeln. Ziel der vorliegenden Studie war es, für diese Zielgruppe eine partizipativ angepasste achtsamkeitsinformierte Mind-Body-Maßnahme (Präsenz und App) hinsichtlich ihrer Wirkung auf gesundheitsbezogene Parameter zu untersuchen.
Methodik
Es wurde eine Pilotstudie (DRKS00030409) als RCT mit drei Gruppen in zwölf Pflegeeinrichtungen durchgeführt. Hierbei gab es eine Präsenz-Gruppe (O), eine Gruppe mit App-Einzelanwendung und technischer Unterstützung (A) und eine passive Kontrollgruppe (C). Die teilnehmenden Bewohnenden (nO=28; nA=29; nC=19) wurden Cluster-randomisiert. Vor, nach und drei Monate nach dem Interventionszeitraum (Dezember 2022 - Januar 2023) wurde mittels eines Fragebogens u. a. das subjektive Wohlbefinden (WHO-5, primäres Outcome) und Achtsamkeit (KIMS-D, inkl. vier Subskalen) erhoben. Es wurde auf Unterschiede innerhalb und zwischen den Studiengruppen und entsprechend der Teilnahmeintensität getestet. Außerdem wurde eine Sensitivitätsanalyse mit Personen durchgeführt, die keine kognitiven Einschränkungen aufwiesen (T0-T2).
Ergebnisse
Es gab einen Hinweis auf eine unterschiedliche Entwicklung des subjektiven Wohlbefindens während des Interventionszeitraums von mittlerer Größe. Während in der Kontrollgruppe eine Verschlechterung zu beobachten war, lag in den Interventionsgruppen keine Reduktion vor. Bei Berücksichtigung der Teilnahmeintensität wurde der Unterschied deutlicher. Außerdem zeigte die App-Gruppe direkt nach der Intervention eine Erhöhung der Achtsamkeit (Subskala Beobachten) im Vergleich zur Kontrollgruppe.
Schlussfolgerung
Weitere Studien mit größeren Stichproben sind erforderlich. Die vorliegenden Ergebnisse weisen jedoch darauf hin, dass die Interventionen das Wohlbefinden und die Achtsamkeit der Zielgruppe verbessert. Die höhere Wirksamkeit in der App-Gruppe könnte durch die Einzelbetreuung erklärt werden. Der Einfluss von Corona-Maßnahmen sowie der Jahreszeit (Winter) auf die Wirksamkeit sind zu prüfen.
Schlüsselwörter
Gesundheitsförderung - Wohlbefinden - Senior:innen - Altenpflege - eHealth - mHealthBackground
Due to the ageing of societies and the increasing need for care, maintaining and promoting the health of those in need of care is gaining further relevance [1]. In 2019, there were 877,200 places in full inpatient long-term care in Germany [2]. Sixteen percent of people with a level of care requirements in Germany live in nursing homes [1]. In order to comply to this relevance, long-term care insurances in Germany have the legal mandate to develop proposals for interventions to strengthen the health resources of residents of nursing homes [3]. Comprehensive scientific evaluations of preventive interventions for residents of nursing homes according to SGB XI § 5 (The Eleventh Book of the German Social Code contains the law governing social care insurance in Germany.) recommend focusing on combined interventions from multiple areas of action (physical activity, violence prevention, cognitive resources, psychosocial health, nutrition) to achieve health-promoting effects [4].
Based on previous findings in health promotion for residents in nursing homes [4] [5] [6], the use of mind-body medicine (MBM), which is based on a connection between mind and body, appears promising [7]. This concept includes, among other things, areas of action such as exercise and nutrition as well as training in mindfulness and self-care. Mind-body interventions typically integrate measures that promote mindfulness indirectly (mindfulness-informed interventions, MII) or directly (mindfulness-based interventions, MBI) [8]. MII aim to improve specific parameters, such as physical flexibility through breathing exercises or yoga [9]. MBI rather “focus on learning or improving mindfulness” [10] (e. g., through breathing meditation or body-scan exercises) [9].
Positive effects on stress reduction and health promotion through MBM have been shown in numerous studies e. g. [11] [5] [12]. Initial tests of MBI have also been carried out for the target group of seniors in the setting of nursing homes [4] [6]. A study on the effectiveness of an MII for the target group of residents in nursing homes has shown that significant increases can be achieved with reference to physical health (subscale of SF-12) and depressive symptoms (GDS-12R). The authors conducted a non-randomized study without follow-up survey and emphasized the need for further adaptions of the course to the needs of seniors [5]. Thus, further insights into the effectiveness of interventions for the target group are still needed [11] [12].
The main aims of this pilot study were to develop a MBM-intervention for residents in nursing homes [13] and to explore the feasibility and effectiveness using qualitative [14] and quantitative methods. This paper describes the quantitative part of the pilot study and contains initial findings on the completetion rates, the effectiveness of the intervention and the expected effect sizes.
Methods
Study design
This pilot study is based on a cluster-randomized controlled study design (RCT). It was registered in the German Register of Clinical Studies (ID: DRKS00030409). Ethics vote (IRB) was obtained from the ethics committee of the University Witten/Herdecke (no. 233/2020).
Intervention
The basis for the participatory intervention development process [13] was the previously developed and evaluated MII health promotion course “BERN” (Behavior, Exercise, Relaxation, Nutrition). Exercises fostering skills in these areas (the BERN intervention) were adapted so that they were tailored to the resources of residents in nursing homes. BERN represents a typical MBM program [8] [15] [16]. The participatory intervention development process involved multiple stakeholders (target group, their relatives, nurses and other experts from nursing homes, health insurance representatives and app developers) and is described in detail by Michaelsen et al. [13].
The result of the intervention development was an eight week group course (on-site) and an one-on-one app intervention (video instruction) with identical content (Online-Appendix 1). The on-site course took place in small groups (3–7 residents). A trainer (qualified therapist for health promotion; experienced with the target group) came to the facilities for around 50–60 minutes once a week and led the exercises of the week in person. The app intervention was completed using the tablets provided. The first exercise of each module was activated on a weekly basis. The next exercise was unlocked when the previous one was either completed or skipped. The entire previous module was unlocked at latest at the start of the new week, i. e., at the beginning of the next module. Exercises could be skipped or repeated. Progress was saved in the individual, non-password-protected profiles. It was not possible to interact with other participants or see other participants´ progress via the app. Project employees offered technical assistance on an individual basis twice a week for approximately 20 minutes each session in the residents' rooms.
Study population
Recruitment
In the first step of recruitment, nursing facilities in North Rhine-Westphalia (Germany) were contacted (N ≈ 250). Facility employees then identified suitable residents. Potential participants were invited to an information event led by project employees.
Inclusion and exclusion criteria
Social service employees in the facilities assessed the inclusion and exclusion criteria (external assessment). The minimum required age of participants was 70 years. Participants had to be physically and cognitively (Mini-Mental Status Test/MMST≥20 at T0) capable of taking part in group activities, as they were required to follow group conversations, articulate themselves, and follow instructions. Furthermore, as a result of the participatory intervention development process, people with severe depression were excluded from participation: this assessment was made via accessing the relevant information in the resident´s file. There were no inclusion or exclusion criteria with regard to the length of time the persons had lived in the nursing home, level of care requirements or involvement of relatives.
Randomization
Twelve nursing homes took part in the research project. Facilities each were randomized to the on-site (O), app (A) and control (C) groups using the web program Jerrydalal by an independent researcher. The result of the randomization process was reported to the participants after T0.
Data collection
Three quantitative surveys (see [Fig. 1]) were conducted in person individually by project employees in the nursing homes using tablets. The pre-survey (T0) took place immediately before the intervention period (Nov 2022). The post-survey (T1) was carried out immediately after the intervention period (Feb 2023), and the follow-up survey (T2) was carried out three months after the end of the intervention period (April 2023). The eight-week intervention were performed between T0 and T1. The survey was performed in German. All outcomes were coded uniformly so that a higher level could be interpreted as more advantageous. In addition, the trainer and the technical support documented the participation every week (see As- treated analysis).

The following socio-demographic information were collected: gender, age, marital status, highest general school qualification, highest professional degree, level of care requirements (1=independence slightly impaired to 5=severe impairment of independence; assessed by nursing care insurance) and move-in dates.
Primary outcome
Subjective well-being [17] [18] was measured by five items, for example: “In the last two weeks I have felt calm and relaxed”. The items were rated on a six-point Likert scale ranging from (0) at no time to (5) all the time concerning the past two weeks. The score was: (0) no well-being to (100) maximum well-being.
Secondary outcomes
The Kentucky Inventory of Mindfulness Skills was used in its short form [19] to calculate an average score for the four fields of mindfulness (observing, describing, acting with attention, accepting without judgment) as well as an overall score ((1) never or very rarely applies/low mindfulness to (5) very often or always applies/high mindfulness).
Cognitive performance was assessed using the mini-mental status test (MMST) [20], which includes everyday questions and action-related tasks. One point was awarded for each correct answer. A maximum of 30 points (sum score) could be achieved [21] [22]
Two items of the Salience and Happiness Database (ESH) was included to measure the current state of happiness (G-1; 21) and life satisfaction (L-1; 22) ((0) not at all happy or satisfied to (10) very happy or satisfied; see also [23]).
The Geriatric Depression Scale in its short form GDS-8 [24] was used to assess mental health (dichotomous response scale; sum score: (0) lowest mental health to (8) highest mental health).
The health-related quality of life was assessed with the first item of the SF-12 ((1) bad to (5) excellent) [25].
Stress warning signals (SWS) were identified with different items (binary coded: (1) yes/applicable (0) no/not applicable) of physical, emotional, cognitive, social and behavioral symptoms (if a SWS occurred: frequency (1) very rare to (10) always) [16].
Data analysis
The analysis was performed using IBM software SPSS Statistics. Pairwise case exclusion was carried out in the analyses. Only a few cases were missing. If a value was missing (WHO-5, KIMS-D, SWS), the single imputation method was used by adding the mean of the remaining answers of the (sub-)scale for the respective collection date.
First, a mean comparison was carried out between the three time points for each group (one-way repeated measures ANOVAs or Friedman test depending on the distribution), which indicated a temporal change (Online-Appendix 2a). If these comparisons were significant, we conducted pairwise comparisons (post hoc tests: Bonferroni or Dunn-Bonferroni) and estimated the effect size Hedges´ g for each pair (Online-Appendix 2b).
Second, change scores (ΔT1-T0, ΔT2-T0: positive sign indicates increase) were calculated for each group to test for differences between groups. Therefore, a mean comparison (one-factorial ANOVA or Welch-ANOVA depending on the variance given a normal distribution for all groups or Kruskal-Wallis test without normal distribution) was carried out between the three groups (study groups or participation intensity) (Online-Appendix 3a). If these comparisons were significant, we conducted pairwise comparisons (post hoc tests: Tukey-Kramer, Games-Howell or Dunn-Bonferroni) and estimated the effect size Hedges´ g for each pair (Online-Appendix 3b).
The significance level was set at p<.05. For the primary outcome, results with p<.1 or values close to this threshold were interpreted as indications. Here |g|=0.2-.49 represents a small effect, |g|=0.5-.79 for a medium effect and |g|≥.8 for a large effect.
Intention-to-treat analysis (ITT)
The ITT aimed to examine the effects of the intervention by group according to cluster randomization. No participants were excluded.
As-treated analysis (AT)
The AT aimed to investigate whether people, regardless of the intervention group, with higher participation intensity (7–8 modules completed) differ from people with low participation intensity (0–6 modules completed) or people in the control group. All randomized participants were included.
Sensitivity analysis
During the study, it became apparent that some participant's cognitive performance decreased to the point below the limit defined in the inclusion criteria. The sensitivity analyses aimed to check how the results differ if only people with long-term sufficient cognitive performance were included. In this sense, the ITT and AT analyses were repeated with the subgroup that achieved at least 20 points on the cognitive performance test (MMST) at all three survey times.
Results
The results are presented below. Outcomes not mentioned did not yield any significant results (MMST, L-1, SF-12) or were evaluated descriptively (SWS).
Description of the sample
Study groups
85 residents were interviewed at T0, of which 77 residents met the inclusion criteria and 76 were randomized (nO=28; nA=29; nC=19). 73.7% of participants completed all three surveys (n=56) (see [Fig. 2]).

Completion rate
Overall, 70.2% (n=40) of the participants in the intervention groups completed the intervention, 59.6% (n=34; nO=13; 46.4%; nA=21; 72.4%) participated in 7–8 modules.
Sociodemographic data
The mean age was 85.66 years (SD: 6.62; range: 71–100). Most participants were widowed (n=51; 67.1%) and had children (n=63; 82.9%). Level of care requirements 2 to 5 were represented in the sample, with care level 3 being the most common (n=39; 51.3%) (see [Tab. 1]). A majority had an equivalent qualification to a secondary or primary school qualification (n=49; 64.5%). Vocational training was most frequently cited as the highest level of training (n=33; 43.4%).
|
Variable |
Total n (%) |
On-site n (%) |
App n (%) |
Control n (%) |
|---|---|---|---|---|
|
Study participants |
76 (100.0%) |
28 (36.8%) |
29 (38.2%) |
19 (25.0%) |
|
Gender |
||||
|
female |
57 (75.0%) |
18 (64.3%) |
24 (82.8%) |
15 (78.9%) |
|
male |
19 (25.0%) |
10 (35.7%) |
5 (17.2%) |
4 (21.1%) |
|
Age |
||||
|
70 to 79 years |
12 (15.8%) |
5 (17.9%) |
2 (6.9%) |
5 (26.3%) |
|
80 to 89 years |
40 (52.6%) |
14 (50.0%) |
17 (58.6%) |
9 (47.4%) |
|
90 to 99 years |
23 (30.3%) |
8 (28.6%) |
10 (34.5%) |
5 (26.3%) |
|
Over 100 years |
1 (1.3%) |
1 (3.6%) |
0 (0.0%) |
0 (0,0%) |
|
Care Level |
||||
|
1 |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
2 |
27 (35.5%) |
13 (46.4%) |
10 (34.5%) |
4 (21.1%) |
|
3 |
39 (51.3%) |
13 (46.4%) |
11 (37.9%) |
15 (78.9%) |
|
4 |
9 (11.84%) |
2 (7.1%) |
7 (24.1%) |
0 (0.0%) |
|
5 |
1 (1.3%) |
0 (0.0%) |
1 (3.4%) |
0 (0.0%) |
|
Marital status |
||||
|
widowed |
51 (67.1%) |
19 (67.9%) |
20 (69.0%) |
12 (63.2%) |
|
Married or registered civil partnership |
10 (13.2%) |
4 (14.3%) |
3 (10.3%) |
3 (15.8%) |
|
Separated/divorced/civil partnership annulled |
6 |
1 (3.6%) |
3 (10.3%) |
2 (10.5%) |
|
single |
9 (11.8%) |
4 (14.3%) |
3 (10.3%) |
2 (10.5%) |
Main analyses
Differences at T0
There were no differences at T0 except for the mindfulness subscale Observing (p=0.006). The post hoc test showed that the on-site group differed significantly from the app group (p=0.024) and from the control group (p=0.028). The T0-mean was highest in the on-site group.
Intention-to-treat analysis
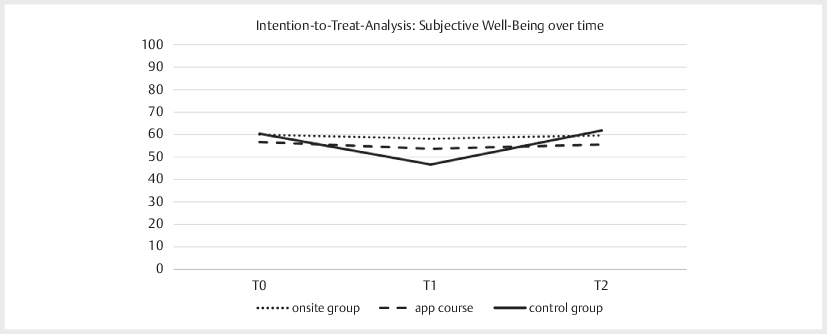
Primary outcome
There was an indication of a different development for subjective well-being (ΔT0-T1) of medium effect size (p=0.112). In addition, there was a temporal change in the control group (p=0.052). The associated post hoc test revealed a significant decrease between T0 and T1 (p=0.03; |g|=0.82) and indicated an increase between T1 and T2 (p=0.073; |g|=0.60). The intervention groups had no significant change over time (see [Fig. 3]).
Secondary outcomes
The change scores ΔT0-T1 for mindfulness subscale Observing were different between the three study groups (p=0.014). Participants with app access showed an increase in the mindfulness subscale Observing compared to the minimally decreased control group (p=0.011; |g|=0.91) and to the almost unchanged on-site group (p=0.052; |g|=0.72).
As- treated analysis
Primary outcome
When considering the intensity of participation, there was a significant difference between the three groups (ΔT0-T1, p=0.036), particularly between participants with high participation intensity and those in the control group (p=0.039; |g|=0.78), whereas the values in the latter decreased between T0 and T1 as in the ITT analysis (see [Fig. 4]).

Secondary outcomes
The development of mental health between T0 and T2 differed between the three groups (p=0.027), particularly between participants with low (decrease) and high (increase) participation intensity (p=0.010; |g|=0.80).
Sensitivity analysis
Seven people (nO=4; nA=3) achieved less than 20 points on the MMST at minimum one survey point after T0. The results in the control group remain consistent because none of the participants met the exclusion criteria for the sensitivity analysis.
Differences at T0
Groups did not differ at T0 except for the mindfulness overall score (p=0.029) and the subscale Observing (p=0.028). The post hoc test showed for both results that the on-site group had significantly higher values than the app group (overall score: p=0.024; subscale Observing: p=0.029).
Intention-to-treat analysis
The sensitivity analysis showed some deviations from reported results of the main analysis. Differences of subjective well-being (ΔT0-T1) increased between the study groups. Further, there were minor deviations from the main analysis regarding the mindfulness subscale Observing (ΔT0-T1; p=0.019). The increased app group differed significantly from the minimally decreased control group (p=0.018; |g|=0.93) and on-site group (p=0.022; |g|=0.80).
In addition, the three study groups exhibited a significant difference in mindfulness (overall score) (ΔT0-T1: p=0.034, ΔT0-T2: p=0.03). The post hoc tests revealed a significant difference between the on-site group (minimally decrease) and the app group (increase) (ΔT0-T1: p=0.044; |g|=0.774). The post hoc tests at ΔT0-T2 were not significant. Additionally, there was a temporal change regarding the mindfulness score (overall score) within the app group (p=0.014). The post hoc test demonstrated a short term increase (ΔT0-T1: p=0.035; |g|=0.572).
As-treated analysis
Almost identical results were found in the sensitivity analysis based on the as-treated samples with regard to subjective well-being (ΔT0-T1; p=0.038). The difference regarding mental health, however, was no longer visible.
In the sensitivity analyses, a difference in happiness was identified (ΔT0-T2; p=0.03). Residents with a low participation intensity experienced a decrease and residents with a high participation intensity showed an increase in happiness (p=0.008; |g|=1.039).
Discussion
We developed and evaluated a MII (on-site and app) for residents in nursing homes. The aim of the present RCT was to assess the influence of this intervention on subjective well-being and other health-related outcomes considering the study group (on-site, app, control), the participation intensity and the cognitive resources.
It can be summarized that the on-site and app intervention appear to “cushion” a decrease in subjective well-being that was observed in the control group. Subjective well-being in the control group worsened during the intervention period (|g|=0.82). Additionally, the app group showed an increase in mindfulness (subscale Observing) during the intervention period in comparison to the control group (slight decrease; |g|=0.91) and the on-site group (unchanged values; |g|=0.72).
A high participation was associated with the maintenance or increase of health-relevant parameters. On the one hand, the difference in subjective well-being (ΔT0-T1) was identified between the control group and residents with a high participation intensity (|g|=0.78). On the other hand, residents with low participation intensity showed a decrease in mental health over the entire study period (ΔT0-T2), while an increase was observed in the control group (|g|=0.87) and group of high participation intensity (|g|=0.80).
The discrepancies between the results of the main and sensitivity analyses suggest that the intervention was particularly more useful for individuals who possess a sufficient level of cognitive ability, as assessed by the MMST. The described beneficial effect of the app intervention regarding the mindfulness subscale Observing (ΔT0-T1), for example, seems to be particularly applicable for people without decreased cognitive abilities (sensitivity analysis: app and control group: |g|=0.64; app and on-site group: |g|=0.77). In this sample, a high participation intensity was also associated with an increase in happiness, while participants with a low participation intensity experienced a decrease (|g|=1.04).
Lastly, none of the analyses of the mindfulness subscales Describing, Acting with attention and Accepting without evaluation, as well as cognitive performance, life satisfaction, and health-related quality of life indicated a significant effect of the intervention for the target group.
The high standardization (on-site courses by one qualified trainer; uniform video instructions in the app) of the intervention should be positively highlighted.
The results does not prove, but already indicate that the intervention improves the subjective well-being and mindfulness of the target group. Individual support could explain the higher effectiveness in the app group. The effectiveness of the intervention is consistent with results in other target groups. For example, Compen et al. (2020) also found that group-based and digital MBI are effective in reducing psychological stress compared to passive control groups [26].
The participant completion rate of over 70% can be seen as an indication of the high level of acceptance and feasibility of the intervention. A comparative study shows that in a mindfulness intervention the completion rate is higher for people with stress symptoms than for pain patients [27]. Ernst et al. (2008) noticed that the study population of older people is more characterized by chronic complaints, which is how the authors explain the higher dropout rate in their study. In relation to the vulnerable target group at hand, the authors already consider a completion rate of 60% to be acceptable [5].
The “cushioning” effect on residents regarding a psychosocial outcome (here: subjective well-being) was also observed in preventive exercise interventions – here, although depressive symptoms were not reduced by the intervention, these remained constant for six months in comparison to a decline in the control group [28]. However, in our RCT, the subjective well-being of the control group almost settled back to the original level at T2. This development could potentially be explained by a seasonal effect (winter). Long-term studies remain necessary.
The results of the as-treated analysis confirm one of the mindfulness principles of the necessity of regular practice to achieve desired outcomes [29]. Parsons et al. (2017) reported in their meta-analysis small to moderate effects of exercise units in mindfulness interventions [30]. Contrary, Keng et al. (2022) found no significant relationship between training duration and changes in the parameters examined [31]. Overall, the dose-response relationship in meditation warrants further research.
A plausible explanation for the slightly better results of the app intervention regarding mindfulness (subscale Observing), in addition to the lower initial level (see differences from T0), could be the individual technical support available to these participants. A meta-analysis of digital-based mindfulness interventions showed, based on 97 included RCTs, that the stress-reducing effect was higher when the intervention was accompanied by specialist staff [32].
Limitations
The generalizability of the results to all residents is limited because most of the participants had care levels 2–3 (86.8%), whereas in Germany only 54% of those in need of care in inpatient facilities have these care levels [1]. Most residents in Germany have higher care levels. It would be useful to develop an adapted intervention or alternative health promotion intervention for residents with care level 4 and 5. The sample size also limits generalizability. However, due to the nature of a pilot study, the analyses are exploratory in nature and must be interpreted accordingly.
The study was conducted in the context of the Covid-19 pandemic, which had a potential impact on the results. Political regulations, such as quarantine measures, were also present in the context of the study. For example, in one nursing facility (control group), a quarantine was prescribed immediately before T0, as in one of the on-site groups immediately after module 7, which meant that the last module could not be offered and the T1 survey was postponed. A systematic review shows that Covid-related visitor restrictions, in general, led to increased loneliness among residents [33].
It should be taken into account that the originally planned double-blinding (participants and interviewer) could not be implemented due to structural constraints. However, our alternative cluster-randomization enabled better feasibility: this also ensured that there was no mutual influence within an institution.
The randomization was largely successful, as shown by the differences from T0. However, for taking assumed differences into account, we used the reported change scores.
Limitations with regard to the data collection process apply because the surveys were provided in person, which could have led to socially desirable answers. This is, however, generally difficult to rule out in psychosocial studies [34]. The additional use of objective measurements (e. g., for stress processing: salivary cortisol, etc.) could improve the reliability of the results in future studies.
Another limitation is that there can be daily fluctuations in the parameters collected (e. g., MMST) [35]. It should also not be neglected that the request for a break during the survey was fulfilled (T0: n=3; T1: n=1). In such a case, the survey was continued on another day.
With respect to data preparation and statistical analysis, the single imputation method can be criticized, among other things, because replacing missing values can reduce the actual variance of the data. [36]
Another methodological limitation in this study concerns the multiple testing problem, we only corrected for post hoc testing. This was accepted, because the RCT is a pilot study (exploratory).
The results of the AT, unlike those of the ITT, cannot be interpreted as a cause-and-effect relationship because the allocation for the AT was not randomized. It can be assumed that confounders had an influence on the residents' participation intensity and effectiveness: For example, individuals with a low participation intensity showed a greater reduction in mental health (ΔT0-T2). It is possible that individuals practiced less because of this health development. It should also be taken into account that peers and companions (e. g., project employees, social service employees) could have influenced the motivation to participate in both directions.Further research with larger samples and a wider variety of participants is needed to improve the generalizability and robustness of the findings. In future research, it would be helpful to introduce a waiting control group and an active control group as comparison with another behavioral prevention intervention to see whether the results can be explained by the MII or mainly by, e. g., the increased personal attention.
Moreover, it can also be assumed that the structural conditions of the nursing homes have an influence on the intervention. Opportunities (e. g. technical support) and obstacles (e. g. missing group room) to the implementation of the intervention and the influence on effectiveness were discussed as part of the qualitative sub-study [14]. In a further evaluation, those results of individual interviews should also be taken into account when constructing questionnaires.
Conclusion
Our RCT aimed to explore the feasibility and effectiveness of an eight-week mindfulness-informed mind-body intervention, which focuses on physical activity, strengthening of mental/cognitive resources, psychosocial health, and nutrition in residents of nursing homes. The results indicate, among others, that the intervention (on-site and app) is effective, e. g., by buffering against negative influences on subjective well-being, particularly when participation intensity was high. In addition, there was an increase regarding mindfulness (subscale Observing) in the app group immediately after the intervention. In addition to its effectiveness, there was also a high level of feasibility and acceptance (over 70% completion rate) among residents. Further evidence-based development and scientific evaluation of MBM interventions in the setting of nursing homes is recommended. Nevertheless, the present pilot study provides suitable initial indications for the positive health promoting effect of mind-body medicine interventions on residents in nursing homes and give a solid basis for a subsequent effectiveness study including sample size calculation.
Fundref Information
gefördert durch den Verband der Ersatzkassen e. V. (vdek) im Namen und Auftrag der Techniker Krankenkasse (TK), BARMER, DAK-Gesundheit, KKH Kaufmännische Krankenkasse, hkk – Handelskrankenkasse und der HEK – Hanseatische Krankenkasse
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgement
Das Projekt wurde vom Verband der Ersatzkassen e. V. (vdek) im Namen und im Auftrag der Ersatzkassen finanziert. Wir danken dem vdek sehr herzlich für die Unterstützung und die wertvolle Zusammenarbeit. Die Geldgeber hatten keinen Einfluss auf das Studiendesign, die Datenerhebung, die Datenanalyse und -interpretation sowie das Verfassen des Manuskripts.
-
References
- 1 Destatis/Statistisches Bundesamt. Hrsg Pflegebedürftige nach Versorgungsart, Geschlecht und Pflegegrade; 2022. Verfügbar unter https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Tabellen/pflegebeduerftige-pflegestufe.html
- 2 Rothgang H, Müller R. Barmer Pflegereport 2021. Wirkungen der Pflegereformen und Zukunftstrends. Berlin; 2021. Schriftenreihe zur Gesundheitsanalyse. 32. Verfügbar unter: https://www.bifg.de/media/dl/Reporte/Pflegereporte/2021/barmer-pflegereport-2021.pdf
- 3 GKV-Spitzenverband. Leitfaden Prävention in stationären Pflegeeinrichtungen nach § 5 SGB XI. 2018
- 4 Vollmer J, Altmann N, Huschik G. et al. Wissenschaftliche Evaluation der präventiven Leistungen der Pflegekassen nach § 5 SGB XI. 2022
- 5 Ernst S, Welke J, Heintze C. et al. Effects of mindfulness-based stress reduction on quality of life in nursing home residents: a feasibility study. Forsch Komplementmed 2008; 15: 74-81
- 6 McBee L. Mindfulness-based elder care: A CAM model for frail elders and their caregivers. New York, NY 10036: Springer Publishing Company, LLC; 2008
- 7 Esch T, Brinkhaus B. Neue Definitionen der Integrativen Medizin: Alter Wein in neuen Schläuchen. Complement Med Res 2020; 27: 67-69
- 8 Esch T. Der Nutzen von Selbstheilungspotenzialen in der professionellen Gesundheitsfürsorge am Beispiel der Mind-Body-Medizin. Bundesgesundheitsbl 2020; 63: 577-585
- 9 Michaelsen MM, Graser J, Onescheit M. et al. Mindfulness-Based and Mindfulness-Informed Interventions at the Workplace: A Systematic Review and Meta-Regression Analysis of RCTs. Mindfulness 2023; 1-34
- 10 Michaelsen MM, Graser J, Onescheit M. et al. Wirksamkeit von Achtsamkeitstechniken im Arbeitskontext. Dresden; 2021. iga.report 45
- 11 Khoury B, Sharma M, Rush SE. et al. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J Psychosom Res 2015; 78: 519-528
- 12 Jayewardene WP, Lohrmann DK, Erbe RG. et al. Effects of preventive online mindfulness interventions on stress and mindfulness: A meta-analysis of randomized controlled trials. Prev Med Rep 2017; 5: 150-159
- 13 Michaelsen MM, Uhl J, Mindrup L. et al. Development of a (digital) mindfulness-informed intervention for the elderly in nursing homes: Description and reflection of a person-based co-design approach submitted.
- 14 Uhl J, Meyer L, Reus A. et al. Barriers and Potentials of Implementing a Mind-Body Intervention in Residential Care Facilities – A Qualitative Interview Study submitted.
- 15 Michaelsen MM, Esch T. Understanding health behavior change by motivation and reward mechanisms: a review of the literature. Front Behav Neurosci 2023; 17: 1151918
- 16 Esch T, Esch S. Stressbewältigung. Mind-Body-Medizin, Achtsamkeit, Resilienz. 4. Aufl. Berlin: Medizinisch Wissenschaftliche Verlagsgesellschaft; 2024
- 17 Topp CW, Østergaard SD, Søndergaard S. et al. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother Psychosom 2015; 84: 167-176
- 18 WHO Regional Office for Europe. Hrsg Wellbeing measures in primary health care/the DEPCARE project. Stockholm 1998
- 19 Höfling V, Ströhle G, Michalak J. et al. A short version of the Kentucky Inventory of Mindfulness Skills. J Clin Psychol 2011; 67: 639-645
- 20 Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189-198
- 21 Esch T. Die Neurobiologie des Glücks: Wie die Positive Psychologie die Medizin verändert. Stuttgart, New York: Georg Thieme Verlag; 2012
- 22 Beierlein C, Kovaleva A, László Z. et al. Kurzskala zur Erfassung der Allgemeinen Lebenszufriedenheit (L-1).
- 23 Karwetzky C, Michaelsen MM, Werdecker L. et al. The U-Curve of Happiness Revisited: Correlations and Differences in Life Satisfaction Over the Span of Life-An Empirical Evaluation Based on Data From 1,597 Individuals Aged 12-94 in Germany. Front. Psychol. 2022; 13: 837638
- 24 Allgaier A-K, Kramer D, Mergl R. et al. Validität der Geriatrischen Depressionsskala bei Altenheimbewohnern: Vergleich von GDS-15, GDS-8 und GDS-4. Psychiatr Prax 2011; 38: 280-286
- 25 Morfeld M, Kirchberger I, Bullinger M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche version des short Form-36 health survey. Hogrefe; 2011
- 26 Compen F, Adang E, Bisseling E. et al. Cost-utility of individual internet-based and face-to-face Mindfulness-Based Cognitive Therapy compared with treatment as usual in reducing psychological distress in cancer patients. Psycho-Oncology 2020; 29: 294-303
- 27 Kabat-Zinn J, Chapman-Waldrop A. Compliance with an outpatient stress reduction program: rates and predictors of program completion. J Behav Med 1988; 11: 333-352
- 28 Diegelmann M, Jansen C-P, Wahl H-W. et al. Does a physical activity program in the nursing home impact on depressive symptoms? A generalized linear mixed-model approach. Aging & mental health 2018; 22: 784-793
- 29 Kabat-Zinn J. Mindfulness for beginners. Boulder. Colorado: Sounds True; 2006
- 30 Parsons CE, Crane C, Parsons LJ. et al. Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants‘ mindfulness practice and its association with outcomes. Behaviour research and therapy 2017; 95: 29-41
- 31 Keng S-L, Chin JWE, Mammadova M. et al. Effects of Mobile App-Based Mindfulness Practice on Healthcare Workers: a Randomized Active Controlled Trial. Mindfulness 2022; 13: 2691-2704
- 32 Sommers-Spijkerman M, Austin J, Bohlmeijer E. et al. New Evidence in the Booming Field of Online Mindfulness: An Updated Meta-analysis of Randomized Controlled Trials. JMIR Ment Health 2021; 8: e28168
- 33 Benzinger P, Kuru S, Keilhauer A. et al. Psychosoziale Auswirkungen der Pandemie auf Pflegekräfte und Bewohner von Pflegeheimen sowie deren Angehörige – Ein systematisches Review. Z Gerontol Geriat 2021; 54: 141-145
- 34 Paulhus DL. Measurement and Control of Response Bias. In: Measures of Personality and Social Psychological Attitudes. Elsevier; 1991. S. 17-59
- 35 Frölich L. S3-Leitlinie „Demenzen“. Symptomatische Therapie der Demenzen. Nervenarzt 2010; 81: 796-798 800-2, 804-6
- 36 Eekhout I, de Vet HCW, Twisk JWR. et al. Missing data in a multi-item instrument were best handled by multiple imputation at the item score level. J Clin Epidemiol 2014; 67: 335-342
Correspondence
Publication History
Received: 22 August 2024
Accepted after revision: 11 December 2024
Accepted Manuscript online:
15 January 2025
Article published online:
03 March 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Destatis/Statistisches Bundesamt. Hrsg Pflegebedürftige nach Versorgungsart, Geschlecht und Pflegegrade; 2022. Verfügbar unter https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Tabellen/pflegebeduerftige-pflegestufe.html
- 2 Rothgang H, Müller R. Barmer Pflegereport 2021. Wirkungen der Pflegereformen und Zukunftstrends. Berlin; 2021. Schriftenreihe zur Gesundheitsanalyse. 32. Verfügbar unter: https://www.bifg.de/media/dl/Reporte/Pflegereporte/2021/barmer-pflegereport-2021.pdf
- 3 GKV-Spitzenverband. Leitfaden Prävention in stationären Pflegeeinrichtungen nach § 5 SGB XI. 2018
- 4 Vollmer J, Altmann N, Huschik G. et al. Wissenschaftliche Evaluation der präventiven Leistungen der Pflegekassen nach § 5 SGB XI. 2022
- 5 Ernst S, Welke J, Heintze C. et al. Effects of mindfulness-based stress reduction on quality of life in nursing home residents: a feasibility study. Forsch Komplementmed 2008; 15: 74-81
- 6 McBee L. Mindfulness-based elder care: A CAM model for frail elders and their caregivers. New York, NY 10036: Springer Publishing Company, LLC; 2008
- 7 Esch T, Brinkhaus B. Neue Definitionen der Integrativen Medizin: Alter Wein in neuen Schläuchen. Complement Med Res 2020; 27: 67-69
- 8 Esch T. Der Nutzen von Selbstheilungspotenzialen in der professionellen Gesundheitsfürsorge am Beispiel der Mind-Body-Medizin. Bundesgesundheitsbl 2020; 63: 577-585
- 9 Michaelsen MM, Graser J, Onescheit M. et al. Mindfulness-Based and Mindfulness-Informed Interventions at the Workplace: A Systematic Review and Meta-Regression Analysis of RCTs. Mindfulness 2023; 1-34
- 10 Michaelsen MM, Graser J, Onescheit M. et al. Wirksamkeit von Achtsamkeitstechniken im Arbeitskontext. Dresden; 2021. iga.report 45
- 11 Khoury B, Sharma M, Rush SE. et al. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J Psychosom Res 2015; 78: 519-528
- 12 Jayewardene WP, Lohrmann DK, Erbe RG. et al. Effects of preventive online mindfulness interventions on stress and mindfulness: A meta-analysis of randomized controlled trials. Prev Med Rep 2017; 5: 150-159
- 13 Michaelsen MM, Uhl J, Mindrup L. et al. Development of a (digital) mindfulness-informed intervention for the elderly in nursing homes: Description and reflection of a person-based co-design approach submitted.
- 14 Uhl J, Meyer L, Reus A. et al. Barriers and Potentials of Implementing a Mind-Body Intervention in Residential Care Facilities – A Qualitative Interview Study submitted.
- 15 Michaelsen MM, Esch T. Understanding health behavior change by motivation and reward mechanisms: a review of the literature. Front Behav Neurosci 2023; 17: 1151918
- 16 Esch T, Esch S. Stressbewältigung. Mind-Body-Medizin, Achtsamkeit, Resilienz. 4. Aufl. Berlin: Medizinisch Wissenschaftliche Verlagsgesellschaft; 2024
- 17 Topp CW, Østergaard SD, Søndergaard S. et al. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother Psychosom 2015; 84: 167-176
- 18 WHO Regional Office for Europe. Hrsg Wellbeing measures in primary health care/the DEPCARE project. Stockholm 1998
- 19 Höfling V, Ströhle G, Michalak J. et al. A short version of the Kentucky Inventory of Mindfulness Skills. J Clin Psychol 2011; 67: 639-645
- 20 Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189-198
- 21 Esch T. Die Neurobiologie des Glücks: Wie die Positive Psychologie die Medizin verändert. Stuttgart, New York: Georg Thieme Verlag; 2012
- 22 Beierlein C, Kovaleva A, László Z. et al. Kurzskala zur Erfassung der Allgemeinen Lebenszufriedenheit (L-1).
- 23 Karwetzky C, Michaelsen MM, Werdecker L. et al. The U-Curve of Happiness Revisited: Correlations and Differences in Life Satisfaction Over the Span of Life-An Empirical Evaluation Based on Data From 1,597 Individuals Aged 12-94 in Germany. Front. Psychol. 2022; 13: 837638
- 24 Allgaier A-K, Kramer D, Mergl R. et al. Validität der Geriatrischen Depressionsskala bei Altenheimbewohnern: Vergleich von GDS-15, GDS-8 und GDS-4. Psychiatr Prax 2011; 38: 280-286
- 25 Morfeld M, Kirchberger I, Bullinger M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche version des short Form-36 health survey. Hogrefe; 2011
- 26 Compen F, Adang E, Bisseling E. et al. Cost-utility of individual internet-based and face-to-face Mindfulness-Based Cognitive Therapy compared with treatment as usual in reducing psychological distress in cancer patients. Psycho-Oncology 2020; 29: 294-303
- 27 Kabat-Zinn J, Chapman-Waldrop A. Compliance with an outpatient stress reduction program: rates and predictors of program completion. J Behav Med 1988; 11: 333-352
- 28 Diegelmann M, Jansen C-P, Wahl H-W. et al. Does a physical activity program in the nursing home impact on depressive symptoms? A generalized linear mixed-model approach. Aging & mental health 2018; 22: 784-793
- 29 Kabat-Zinn J. Mindfulness for beginners. Boulder. Colorado: Sounds True; 2006
- 30 Parsons CE, Crane C, Parsons LJ. et al. Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants‘ mindfulness practice and its association with outcomes. Behaviour research and therapy 2017; 95: 29-41
- 31 Keng S-L, Chin JWE, Mammadova M. et al. Effects of Mobile App-Based Mindfulness Practice on Healthcare Workers: a Randomized Active Controlled Trial. Mindfulness 2022; 13: 2691-2704
- 32 Sommers-Spijkerman M, Austin J, Bohlmeijer E. et al. New Evidence in the Booming Field of Online Mindfulness: An Updated Meta-analysis of Randomized Controlled Trials. JMIR Ment Health 2021; 8: e28168
- 33 Benzinger P, Kuru S, Keilhauer A. et al. Psychosoziale Auswirkungen der Pandemie auf Pflegekräfte und Bewohner von Pflegeheimen sowie deren Angehörige – Ein systematisches Review. Z Gerontol Geriat 2021; 54: 141-145
- 34 Paulhus DL. Measurement and Control of Response Bias. In: Measures of Personality and Social Psychological Attitudes. Elsevier; 1991. S. 17-59
- 35 Frölich L. S3-Leitlinie „Demenzen“. Symptomatische Therapie der Demenzen. Nervenarzt 2010; 81: 796-798 800-2, 804-6
- 36 Eekhout I, de Vet HCW, Twisk JWR. et al. Missing data in a multi-item instrument were best handled by multiple imputation at the item score level. J Clin Epidemiol 2014; 67: 335-342