

Subscribe to RSS
DOI: 10.1055/a-2544-7919
Safety and Efficacy of Factor Xa Inhibitors in Atrial Fibrillation Patients on Dialysis: Evidence from Four Randomized Controlled Trials
Authors
Funding This study was funded by the National Natural Science Foundation of China (82370383, 82100273); Guangdong Natural Science Foundation (2024A1515013289; 2023A1515012798); Key R and D Projects of Guangzhou Science and Technology Program (2023B03J1243); and Young Doctor “Sailing” Project (SL2024A04J01866).

Abstract
Atrial fibrillation (AF) is prevalent in dialysis-dependent patients, who face higher risks of thromboembolism and bleeding. Although vitamin K antagonists (VKAs) are commonly used for anticoagulation, the benefits of factor Xa (FXa) inhibitors over VKAs in this population are unclear. This systematic review aims to compare the efficacy and safety of VKAs and FXa inhibitors based on randomized controlled trials (RCTs). We conducted a systematic search of PubMed and Embase for RCTs comparing FXa inhibitors and VKAs up to November 2024. The primary safety outcome was major bleeding, and the primary efficacy outcome was stroke or systemic embolism (SSE). Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using random-effects models. This meta-analysis included 486 dialysis-dependent AF patients from 4 RCTs, with a median follow-up of 26 weeks to 1.88 years. FXa inhibitors were associated with a reduced risk of major bleeding compared to VKAs (RR = 0.64, 95% CI = 0.42–0.99; p = 0.04), but no significant difference in SSE (RR = 0.46, 95% CI = 0.20–1.02; p = 0.06). FXa inhibitors also showed a significantly lower risk of intracranial bleeding (RR = 0.40, 95% CI = 0.17–0.96; p = 0.04), but no differences in other outcomes, including gastrointestinal bleeding, hemorrhagic stroke, ischemic stroke, acute coronary syndrome, and mortality. This systematic review and meta-analysis suggest that FXa inhibitors may offer a safer alternative to VKAs for AF patients on dialysis, with a lower risk of bleeding and similar risks of stroke and mortality.
Introduction
Atrial fibrillation (AF) is highly prevalent in patients with chronic kidney disease (CKD), affecting 15 to 20% of those in advanced CKD stages, with even higher rates observed in individuals on maintenance dialysis.[1] The coexistence of AF and CKD complicates management due to the increased risk of thromboembolic events and bleeding complications.
The vitamin K antagonists (VKAs) have traditionally been the oral anticoagulant (OAC) of choice, but they present challenges, including difficulty maintaining a therapeutic international normalized ratio (INR), an increased bleeding risk, and concerns regarding accelerated medial vascular calcification in patients with end-stage kidney disease (ESKD).[2] Although direct oral anticoagulants (DOACs)—including factor Xa (FXa) inhibitors (rivaroxaban, edoxaban, apixaban) and the direct thrombin inhibitor dabigatran—may offer potential advantages in AF patient, their reliance on renal clearance and limited data in dialysis-dependent patients make the optimal anticoagulation strategy for AF patients with advanced CKD uncertain.[3] [4] [5] As a result, current guidelines reflect uncertainty regarding the role of oral anticoagulation in this population.[6] [7] [8]
Recent multicenter RCTs (Valkyrie, Strategies for the Management of Atrial Fibrillation in patiEnts Receiving Dialysis [SAFE-D], Renal Hemodialysis Patients Allocated Apixaban versus Warfarin in Atrial Fibrillation [RENAL-AF], and Compare API and Vitamin K Antagonists in Patients With Atrial Fibrillation and End-Stage Kidney Disease [AXADIA-AFNET 8])[9] [10] [11] [12] have investigated anticoagulation strategies for hemodialysis patients with AF. The Valkyrie trial showed that reduced-dose rivaroxaban was superior to VKAs in reducing cardiovascular events and major bleeding. In contrast, the SAFE-D, RENAL-AF, and AXADIA-AFNET 8 trials found no significant differences in outcomes between apixaban and VKAs.[9] [11] [12]
Adding to the complexity, two prior meta-analyses on this topic have reported conflicting conclusions, with one including only non-randomized observational studies, while the other included data from the Valkyrie and RENAL-AF trials, which together had less than 1% of participants from RCTs.[13] [14] This further highlights the uncertainty in clinical decision-making. This raises important questions regarding the appropriateness of anticoagulation therapy for this vulnerable population.[15]
Therefore, we conducted a systematic review and meta-analysis of RCTs evaluating the safety and efficacy of FXa inhibitors versus VKAs in dialysis-dependent AF patients.
Methods
We conducted this systematic review and meta-analysis in accordance with the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (version 6.2).[16] The results are presented following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Statement,[17] an updated guideline for reporting systematic reviews.
Patient and Public Involvement
Patients were not involved in formulating the research question, selecting outcome measures, or designing and executing the study. Their input regarding interpretation or dissemination of the study's findings should have been sought. There were no plans to communicate the research outcomes to the study participants or the broader patient community. Ethical approval was not required for this study, as it was based exclusively on published research. The data supporting the findings of this meta-analysis are available from the corresponding authors upon reasonable request.
Literature Search
A comprehensive search was conducted in the PubMed and Embase databases until November 2024 to identify the relevant studies. The search terms included keywords related to (1) atrial fibrillation, (2) dialysis or hemodialysis or peritoneal dialysis, (3) direct oral anticoagulants or non-vitamin K antagonist oral anticoagulants or rivaroxaban or apixaban or edoxaban, (4) vitamin K antagonists or warfarin or coumadin or coumadine or phenprocoumon or acenocoumarol or fluindione, and (5) randomized controlled trial. The search terms were connected using the Boolean operator “AND.” The full search strategy is provided in [Supplementary Table S1] (available in the online version only). Additionally, a manual review of reference lists from previous review articles was performed to identify any relevant studies that may have been overlooked during the database search. In this study, we imposed no language restrictions during the literature search.
Eligibility Criteria
Inclusion criteria for the studies followed the PICOS framework as outlined: (1) Population: Patients with ESKD who were undergoing dialysis (either hemodialysis or peritoneal dialysis) and diagnosed with AF. (2) Intervention: Administration of FXa inhibitors, namely rivaroxaban, apixaban, or edoxaban. (3) Comparison: Any type of VKAs, including warfarin, coumadin, coumadine, phenprocoumon, acenocoumarol, and fluindione. (4) Outcomes: The primary safety outcome was major bleeding, while the primary efficacy outcomes were stroke or systemic embolism (SSE). Our secondary safety outcomes included gastrointestinal bleeding, intracranial bleeding, clinically relevant non-major bleeding, and hemorrhagic stroke, whereas secondary efficacy outcomes included ischemic stroke, acute coronary syndrome, all-cause mortality, cardiovascular (CV) mortality, and non-CV mortality. The outcomes and their definitions were based on those used in the studies originally included in the analysis. (5) Study design: only RCTs were included.
Studies classified as animal experiments, case reports, review articles, meta-analyses, editorials, or conference abstracts were excluded. Observational studies were also excluded from the analysis. Single-arm studies focused exclusively on FXa inhibitors were also excluded, as they did not provide a comparative analysis with VKAs. Additionally, studies that did not provide relevant data on efficacy or safety outcomes were excluded. In the case of duplicate studies, the one with the longer follow-up period or larger sample size was selected for inclusion.
Study Selection and Data Extraction
Two independent investigators screened the titles and abstracts of the identified studies, applying predefined exclusion criteria. After the initial screening, studies that met the eligibility criteria were subjected to full-text review. Discrepancies were resolved by consensus or discussion with a third reviewer.
Data extracted from each included study included the following: first author, publication year, study design, trial acronyms, location, dialysis characteristics, sample size, participant demographics, type and dosage of FXa inhibitors, time in therapeutic range (TTR) for the VKA group, CHA2DS2-VASc (congestive heart failure or left ventricular dysfunction [1 point]; hypertension [1 point]; age 75 years or older [2 point]; diabetes [1 point]; stroke or transient ischaemic attack or other thromboembolism [1 point]; vascular disease [previous myocardial infarction, peripheral artery disease, or aortic plaque; 1 point]; age 65–74 years [1 point]; and female sex [1 point]) and HAS-BLED (hypertension [1 point], abnormal renal and liver function [1 point each], stroke [1 point], bleeding [1 point], labile international normalized ratios [1 point], elderly [>65 years, 1 point], drugs or alcohol [1 point each] ) scores, follow-up duration, comorbidities, prior medications, and relevant outcomes.
Risk of Bias Assessment
The Risk of Bias 2 (RoB 2) tool was used to assess the methodological quality and potential biases in the included RCTs.[18] This tool offers a detailed evaluation across various domains critical to study integrity, including bias arising from the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Each domain is rated as having a low risk of bias, some concerns, or a high risk of bias.
The findings from our RoB 2 assessment were visually represented using the Robvis tool (https://mcguinlu.shinyapps.io/robvis/).
Heterogeneity Test
We used the p-value from the Cochrane Q test and the I 2 statistic to evaluate the heterogeneity among the studies included in our analysis. These indexes are instrumental in determining the degree of variability between the studies that could impact the reliability of a pooled estimate. Specifically, a p-value less than 0.10 from the Cochrane Q test or an I 2 value greater than 50% indicated the presence of significant heterogeneity.
Statistical Analysis and Data Synthesis
We collected data on sample sizes and event counts for both treatment arms from the included studies. We used a random-effects model for the primary pooled analysis to account for the anticipated clinical heterogeneity among the studies, such as differences in treatment strategies. Risk ratios (RRs) with 95% confidence intervals (CIs) were calculated for dichotomous data from RCTs. We reanalyzed the data above in the sensitivity analysis using a fixed-effects model. In addition, we performed a sensitivity analysis by pooling studies that used apixaban alone.
All statistical analyses were conducted using Review Manager version 5.4 software from the Cochrane Collaboration (2014, Nordic Cochrane Centre, Copenhagen, Denmark). The visual summary image was generated by plotting the forest plot in R (version 4.3.1) and then summarizing it using Microsoft PowerPoint. In this study, a p-value of <0.05 was considered statistically significant.
Quality of Evidence
The quality of evidence for the outcomes was evaluated using the GRADE (a systematic approach to rating the certainty of evidence in systematic reviews and other evidence syntheses) system.[19] Independent evaluations were conducted by two investigators, with consensus reached through discussion. The GRADEpro Guideline Development Tool (GRADEpro GDT: McMaster University and Evidence Prime, 2024) was used to generate the results (https://www.gradepro.org).
Results
Study Selection
The PRISMA flow diagram in [Fig. 1] illustrates the rigorous study selection process for the meta-analysis. A comprehensive search of the PubMed and Embase databases initially identified 2,159 studies ([Supplementary Table S1] [available in the online version only]). After removing 25 duplicate entries, the titles and abstracts of the remaining 2,134 studies were screened. This process led to the exclusion of 2,129 studies due to irrelevance or because they were not RCTs. Five RCTs remained and underwent full-text review. Upon closer examination, the APIDP2 (Safety and Efficacy of Apixaban Versus Warfarin in Peritoneal Dialysis Patients With Non Valvular Atrial Fibrillation) trial was excluded as it was only a study protocol.

Finally, four RCTs[9] [10] [11] [12] (AXADIA-AFNET 8, RENAL-AF, Valkyrie trial, and SAFE-D) were included in the meta-analysis.
Baseline Characteristics
[Table 1] provides the baseline characteristics from four RCTs comparing DOACs to VKAs in AF patients receiving dialysis. The Valkyrie study involved 132 AF patients on hemodialysis, randomized into three groups: VKA, rivaroxaban, or rivaroxaban plus vitamin K2 supplement.[10] The SAFE-D trial was a pilot study that enrolled 151 AF patients on dialysis randomized to apixaban, warfarin, or no oral anticoagulation.[12] The RENAL-AF trial compared apixaban with warfarin in 154 patients on hemodialysis with AF but was terminated early due to recruitment challenges.[11] The AXADIA-AFNET 8 study was an RCT that compared apixaban with phenprocoumon in 97 AF patients on dialysis.[9]
|
Studies |
Study type |
Trial acronyms |
Location |
Comparison |
Dialysis characteristics |
Sample size |
Age (years) |
Female (%) |
DOAC type and dosage |
TTR for VKA group |
Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Reinecke et al. (2023)[9] |
PROBE RCT |
AXADIA-AFNET 8 trial; NCT02933697 |
Germany; 2017–2022 |
Apixaban versus Phenprocoumon |
Hemodialysis: 93.8%; Peritoneal: 6.2% |
n = 97 API (48) and phenprocoumon (49) |
74.7 |
30% |
API; 2.5 mg BID |
50.7% |
API: 429 days VKA: 506 days |
|
Pokorney et al. (2022)[11]* |
Multicenter RCT; PROBE |
RENAL-AF trial; NCT02942407 |
42 U.S. clinical sites; 2017–2019 |
API versus Warfarin |
Hemodialysis |
n = 154 API (82) and warfarin (72) |
68.0 |
56% |
API; 5 mg BID (2.5 mg BID for patients ≥80 years, weight ≤60 kg) |
44% |
API: 330 days VKA: 340 days |
|
De Vriese et al. (2021)[10] |
Multicenter RCT |
Valkyrie trial; NCT03799822 |
3 sites in Belgium; 2015–2019 |
RIV versus VKA versus RIV + Vitamin K2 |
Hemodialysis |
n = 132 Rivaroxaban (88) and VKA (44) |
RIV: 79.9 and VKA: 80.3 |
33% |
RIV; 10 mg QD |
48% |
1.88 years |
|
Harel et al. (2024)[12] |
Pilot RCT |
SAFE-D trial; NCT03987711 |
28 centers in Canada and Australia; 2019–2022 |
API versus Warfarin versus No OAC |
Hemodialysis: 93%; Peritoneal: 7% |
n = 103 API (51) and warfarin (52) |
API: 72 and VKA: 71 |
22.3% |
API; 5 mg BID (2.5 mg BID for patients ≥80 years, weight ≤60 kg) |
58% |
26 weeks |
Abbreviations: API, apixaban; AXADIA-AFNET 8, Compare API and Vitamin K Antagonists in Patients With Atrial Fibrillation and End-Stage Kidney Disease; BID, twice daily; DOAC, direct oral anticoagulant; INR, international normalized ratio; OAC, oral anticoagulation; PROBE, Prospective Randomized Open Blinded End point; QD, once daily; RCT, randomized controlled trial; RENAL-AF, Renal Hemodialysis Patients Allocated API versus Warfarin in Atrial Fibrillation; RIV, rivaroxaban; SAFE-D, Strategies for the Management of Atrial Fibrillation in patiEnts Receiving Dialysis; TTR, time in therapeutic range; VKA, vitamin K antagonist.
a Prematurely stopped due to enrollment challenges.
[Table 2] shows a comparative analysis of baseline characteristics between patients with AF on dialysis who were randomized to receive DOACs versus VKAs. This included demographics, time since dialysis initiation, CHA2DS2-VASc and HAS-BLED scores, comorbidities, and previous medications.
|
Studies |
Reinecke et al. (2023)[9] |
Pokorney et al. (2022)[11] |
De Vriese et al. (2021)[10] |
Harel et al. (2024)[12] |
|
|---|---|---|---|---|---|
|
Comparison |
API versus Phenprocoumon |
API versus Warfarin |
RIV versus VKA versus RIV |
API versus Warfarin |
|
|
Age, y |
DOAC |
76.5 (68–81) |
69.0 (61.0–76.0) |
79.9 (74.4–83.9) |
72 (64–81) |
|
VKA |
77 (70–80) |
68.0 (60.5–72.5) |
79.6 (73.2–83.1) |
71 (67–78) |
|
|
Females |
DOAC |
17 (35.4) |
34 (41.5) |
11 (24.9) |
14 (28) |
|
VKA |
12 (24.5) |
22 (30.6) |
19 (43.2) |
9 (17) |
|
|
Time since dialysis initiation, y |
DOAC |
2.3 (1.0–7.2) |
2.8 (1.6–5.7) |
2.7 (0.9–5.9) |
2.2 (1.1–5.2) |
|
VKA |
2.9 (0.8–5.0) |
3.0 (1.2–6.3) |
1.8 (0.4–5.5) |
2.5 (1.1, 4.1) |
|
|
CHA2DS2-VASc |
DOAC |
5 (3.5–5) |
4 (3–5) |
5 (4–5) |
4 (3–5) |
|
VKA |
4.5 (4–6) |
4 (3–5) |
5 (4–6) |
4 (3–5) |
|
|
HAS-BLED |
DOAC |
4 (3.5–5) |
NA |
4 (4–5) |
NA |
|
VKA |
4.0 (3.5–5) |
NA |
5 (4–5) |
NA |
|
|
Previous MI |
DOAC |
9 (18.8) |
16 (19.5) |
21 (45.7) |
12 (24.0) |
|
VKA |
12 (24.5) |
22 (30.6) |
21 (47.7) |
11 (21.0) |
|
|
Heart failure |
DOAC |
NA |
43 (52.4) |
9 (37.0) |
19 (37.0) |
|
VKA |
NA |
41 (56.9) |
17 (20.5) |
20 (38.0) |
|
|
History of stroke |
DOAC |
NA |
24 (29.2) |
15 (32.6) |
7 (14.0) |
|
VKA |
NA |
15 (20.9) |
16 (36.4) |
7 (14.0) |
|
|
Diabetes |
DOAC |
NA |
42 (51.2) |
20 (43.5) |
35 (69) |
|
VKA |
NA |
47 (65.3) |
20 (45.5) |
33 (64) |
|
|
PAD |
DOAC |
NA |
15 (18.3) |
NA |
4 (8) |
|
VKA |
NA |
11 (15.3) |
NA |
10 (19) |
|
|
Hypertension |
DOAC |
NA |
79 (96.3) |
NA |
46 (90) |
|
VKA |
NA |
67 (93.1) |
NA |
42 (81) |
|
|
NYHA III–IV classification |
DOAC |
16 (33.3) |
9 (21.4) |
NA |
NA |
|
VKA |
11 (22.5) |
4 (10.5) |
NA |
NA |
|
|
Previous NOAC therapy |
DOAC |
8 (16.7) |
19 (23.2) |
NA |
3 (6) |
|
VKA |
3 (6.1) |
21 (29.2) |
NA |
0 (0) |
|
|
Previous VKA therapy |
DOAC |
25 (52.1) |
NA |
28 (60.9) |
18 (35) |
|
VKA |
31 (63.3) |
NA |
30 (68.2) |
22 (42) |
|
|
Aspirin |
DOAC |
16 (33.3) |
29 (36.7) |
15 (32.6) |
14 (28) |
|
VKA |
17 (34.7) |
32 (45.7) |
14 (31.8) |
16 (31) |
|
|
P2Y12 inhibitors |
DOAC |
NA |
2 (2.5) |
NA |
4 (8) |
|
VKA |
NA |
1 (1.4) |
NA |
1 (2) |
|
|
NSAIDs |
DOAC |
NA |
4 (5.1) |
NA |
1 (2) |
|
VKA |
NA |
7 (10) |
NA |
0 (0) |
|
Abbreviations: AF, atrial fibrillation; API, apixaban; DOAC, direct oral anticoagulant; IQR, interquartile range; NA, not available; NSAID, nonsteroidal anti-inflammatory drug; PAD, peripheral artery disease; RIV, rivaroxaban; MI, myocardial infarction; VKA, vitamin K antagonist; y, years.
Median (25th and 75th percentiles) are displayed for continuous variables. Counts (percentages) are displayed for categorical variables.
Risk of Bias Assessment
The risk of bias assessment is shown in [Fig. 2]. Overall, among the four RCTs included in our analysis, two were classified as having a low risk of bias (AXADIA-AFNET 8 trial and Valkyrie trial)[9] [10] while the other two study were categorized as some concerns risk of bias (RENAL-AF trial and SAFE-D trial).[11] [12] The study deemed to have some concerns and risk of bias were primarily affected by their premature termination due to challenges in patient enrollment.

Primary Outcomes
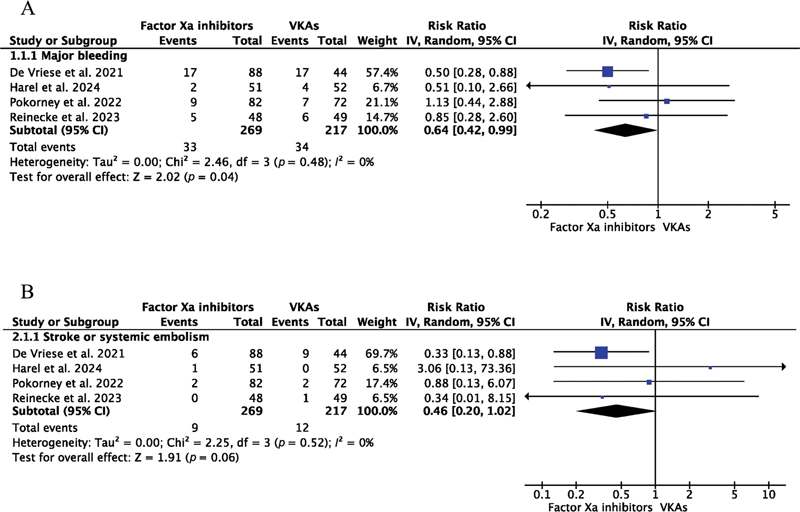
Across the four RCTs, 269 patients receiving FXa inhibitors experienced 33 major bleeding events, while 217 patients treated with VKAs had 34 major bleeding events ([Fig. 3A]). The pooled analysis demonstrated a statistically significant reduction in the risk of major bleeding with FXa inhibitors compared to VKAs (RR = 0.64, 95% CI = 0.42–0.99; p = 0.04). In patients with AF on hemodialysis, FXa inhibitors showed a trend toward reducing the risk of SSE compared to VKAs ([Fig. 3B] and Visual Summary), though this difference was not statistically significant (RR = 0.46; 95% CI = 0.20–1.02; p = 0.06).
Secondary Outcomes
In the analysis of secondary safety outcomes, no significant differences were observed between FXa inhibitors and VKAs for gastrointestinal bleeding (RR = 0.95; 95% CI = 0.54–1.67; p = 0.86), clinically relevant non-major bleeding (RR = 1.10; 95% CI = 0.71–1.70; p = 0.67), or hemorrhagic stroke (RR = 0.50; 95% CI = 0.02–12.09; p = 0.67) in patients with AF on hemodialysis ([Fig. 4] and Visual Summary). Also, FXa inhibitors were associated with a significantly lower risk of intracranial bleeding compared to VKAs (RR = 0.40; 95% CI = 0.17–0.96; p = 0.04).

In the analysis of secondary efficacy outcomes ([Fig. 5] and Visual Summary), no significant differences were observed between FXa inhibitors and VKAs for ischemic stroke (RR = 0.33; 95% CI = 0.06–1.88; p = 0.21), acute coronary syndrome (RR = 0.87; 95% CI = 0.40–1.91; p = 0.73), all-cause mortality (RR = 0.88; 95% CI = 0.58–1.35; p = 0.57), cardiovascular mortality (RR = 1.13; 95% CI = 0.61–2.10; p = 0.70), or non-cardiovascular mortality (RR = 0.38; 95% CI = 0.12–1.22; p = 0.10) in patients with AF receiving dialysis.

Sensitivity Analysis
When pooling data from the three apixaban RCTs—AXADIA-AFNET 8 (apixaban 2.5 mg twice daily [BID]), RENAL-AF (apixaban 5 mg BID), and SAFE-D (apixaban 5 mg BID)—there were no statistically significant differences in the primary and secondary safety and efficacy outcomes between apixaban and VKAs ([Supplementary Figs. S1–S3] [available in the online version only]).
The sensitivity analysis also used a fixed-effects model to account for the expected clinical heterogeneity among the studies. The primary and secondary safety and efficacy outcomes results showed no notable changes ([Supplementary Figs. S4–S6] [available in the online version only]), indicating that the findings are robust and not significantly influenced by variability across the included studies.
Quality of Evidence
We used GRADEpro GDT to assess the quality of evidence for the following primary and secondary outcomes: The quality of evidence for hemorrhagic stroke in the included RENAL-AF, Valkyrie trial, and SAFE-D studies was rated as moderate due to relatively high heterogeneity ([Supplementary Table S2] [available in the online version only]). The remaining outcomes were rated as high-quality evidence due to good performance in terms of study design, risk of bias, inconsistency, indirectness, and imprecision.
Discussion
This meta-analysis, which included four RCTs comparing FXa inhibitors to VKAs in AF patients on dialysis, demonstrated that FXa inhibitors were associated with a statistically significant reduction in major bleeding risk compared to VKAs, particularly for intracranial bleeding. Second, no significant differences were observed for other secondary safety outcomes, including gastrointestinal bleeding, clinically relevant non-major bleeding, and hemorrhagic stroke. Third, FXa inhibitors showed a non-significant trend toward reducing stroke or SSE, and no significant differences were found for all-cause mortality or secondary efficacy outcomes.
These findings contribute valuable evidence to clinical uncertainty and suggest that FXa inhibitors may offer a safer alternative to VKAs for anticoagulation in dialysis-dependent AF patients, especially in reducing severe bleeding risks.
AF increases the risk of SSE by five-fold compared to individuals without AF.[20] In a meta-analysis of 25 studies, Zimmerman et al. found that the annual stroke incidence in ESKD patients with AF was two to three times higher than in those without AF (5.2/100 versus 1.9/100 patient-years).[21] This highlights the dual challenge in this population, as the use of anticoagulants such as low-molecular-weight heparin or citrate during dialysis may elevate bleeding risks,[22] potentially offsetting some of the thromboembolic risks associated with AF. In addition, declining kidney function affects the metabolism and pharmacokinetics of drugs, necessitating dose adjustments for DOACs based on renal function, particularly in patients with more advanced kidney disease (glomerular filtration rate <30 mL/min).[23] [24] In addition, dialysis-dependent AF patients face an elevated risk of stroke and thrombosis, not only due to the increased stroke risk associated with AF but also because hemodialysis contributes to thrombosis through chronic platelet activation caused by repeated contact with artificial surfaces during the dialysis process.[25]
Among the RCTs included in our meta-analysis, the Valkyrie trial contributed the most to the overall results,[10] with the greatest weight in the pooled analysis, exceeding 50% in almost all subgroups. Although it was not the trial with the largest sample size, the Valkyrie trial stands out for its longest follow-up period of 1.88 years. The SAFE-D trial,[12] while smaller, provided valuable insight as a pilot trial that demonstrated the feasibility of recruitment and adherence in a study comparing different anticoagulation strategies in patients with AF receiving dialysis. However, due to the low number of events in both groups, the confidence intervals for all measured endpoints were quite wide, limiting the precision of the findings.
In the AXADIA-AFNET 8 trial,[9] the control group received phenprocoumon, whereas the other three trials used warfarin as the comparator. Both phenprocoumon and warfarin are VKAs, with phenprocoumon being the most commonly used VKA in Austria, Germany, and Switzerland, accounting for over 90% of all VKA-treated patients.[26] [27] Phenprocoumon has different pharmacokinetic features compared to warfarin, including its metabolism and plasma half-life, which result in varying plasma concentrations.[28] A recent retrospective multicenter study found that phenprocoumon provided better anticoagulation quality than warfarin; however, factors such as female gender, longer INR testing intervals, the absence of beta blockers, and preimplant gastrointestinal bleeding were associated with an increased risk of hemocompatibility-related adverse events in left ventricular assist device patients.[29] In our meta-analysis, phenprocoumon and warfarin were grouped as VKAs for analysis, which was a necessity due to the limited number of studies available comparing these agents separately.
The RCTs included in our analysis showed balanced baseline characteristics between the FXa inhibitors and VKAs groups, including CHA2DS2-VASc and HAS-BLED scores.[9] [10] [11] [12] Among the DOAC regimens, the Valkyrie trial (rivaroxaban 10 mg once daily [QD]) and the AXADIA-AFNET 8 trial (apixaban 2.5 mg bid) employed reduced-dose DOACs. In contrast, the RENAL-AF and SAFE-D trials utilized standard doses (apixaban 5 mg bid), except in cases of advanced age (>80 years) or low body weight (<60 kg), where dose reductions were applied. In contrast, the TTR for VKAs was consistently suboptimal, ranging from 44 to 58%.
The trial patient profile aligns closely with findings from a large study of U.S. veterans with AF, where ESKD patients had a TTR of 43%.[30] Notably, in the Valkyrie trial (TTR of 44%) and RENAL-AF trial (TTR of 48%), patients were three-fold more likely to have subtherapeutic INR values (<2.0) compared to supratherapeutic levels (>3.0).[10] [11] The pooled analysis of the four RCTs demonstrated that DOACs, compared with VKAs, showed no significant difference in SSE (stroke or SSE) or all-cause mortality but were associated with a lower incidence of major bleeding events in dialysis-dependent AF patients. Considering these findings occurred despite the suboptimal TTR observed in the VKA group, these results favor the use of FXa inhibitors as a more reliable anticoagulation strategy in this population.
Regarding the outcomes of our study, major bleeding and SSE, among 486 patients, 68 experienced major bleeding while only 21 had SSE. Clearly, major bleeding occurred significantly more often than SSE (p < 0.01). Effective risk stratification (CHA2DS2-VASc) is a prerequisite for adequately preventing AF-related strokes. For the general population, the increased baseline stroke risk is sufficient to benefit from anticoagulation therapy. However, this may not be applicable when evaluating AF patients on dialysis using the same criteria, as in a substantial proportion of AF dialysis patients, the high risk of death due to bleeding may outweigh the stroke risk.[31] In real-life practice, almost all patients with hemodialysis and AF meet the criteria for OAC therapy based on the same scoring assessments.[32] In this bleeding-prone population, risk stratification must consider the inherent bleeding risks associated with dialysis.
Limitations
Although this study provides a comprehensive evaluation of the safety and efficacy of FXa inhibitors compared to VKAs in anticoagulant therapy for dialysis-dependent AF patients, there are several limitations to consider. First, the sample size of the included studies is relatively small, with only 486 patients, which may impact the generalizability and statistical power of the results. Additionally, despite performing sensitivity analyses to test the robustness of the findings, the heterogeneity in study design, treatment protocols, and follow-up periods across the four RCTs included in the analysis may introduce bias into the results. Notably, the RENAL-AF trial was prematurely terminated due to recruitment challenges, which could affect the accuracy of the overall conclusions. Moreover, the follow-up periods in all included studies were relatively short, ranging from 26 weeks to 1.88 years, which is insufficient to assess the long-term safety and efficacy of FXa inhibitors, particularly with regard to chronic complications that may arise in dialysis-dependent patients. While we excluded observational and single-arm studies, all the included trials focused on specific FXa inhibitors (such as apixaban and rivaroxaban), which limits the external validity of the findings and may not fully represent other FXa inhibitors or the broader population of dialysis-dependent AF patients. Finally, the included RCTs were based on white European populations, with limited representation from other ethnic groups. Given the reported ethnic differences in thromboembolism and bleeding, further studies in ethnically diverse cohorts are needed.[33] [34]
Conclusion
This systematic review and meta-analysis suggest that FXa inhibitors may offer a safer alternative to VKAs for AF patients on dialysis, with a lower risk of bleeding and similar risks of stroke and death.
Conflict of Interest
None declared.
Data Availability Statement
The data supporting the findings of this meta-analysis are available from the corresponding author upon reasonable request. The original datasets from the included RCTs (AXADIA-AFNET 8, RENAL-AF, Valkyrie trial, and SAFE-D) can be accessed via the respective trial databases or through direct contact with the authors of the studies.
Authors' Contribution
W.K. and Y.C. contributed equally to the study design, data collection, and manuscript drafting. Y.C. and C.L. assisted with data analysis and literature review. G.Y.H.L. provided input on study methodology and clinical interpretation. W.Z. supervised the study and reviewed the manuscript. All authors approved the final manuscript.
* These authors contributed as co-first authors.
The review process for this paper was fully handled by Christian Weber, Editor in Chief.
-
References
- 1 Wizemann V, Tong L, Satayathum S. et al. Atrial fibrillation in hemodialysis patients: clinical features and associations with anticoagulant therapy. Kidney Int 2010; 77 (12) 1098-1106
- 2 Yang F, Chou D, Schweitzer P, Hanon S. Warfarin in haemodialysis patients with atrial fibrillation: what benefit?. Europace 2010; 12 (12) 1666-1672
- 3 De Vriese AS, Caluwé R, Raggi P. The atrial fibrillation conundrum in dialysis patients. Am Heart J 2016; 174: 111-119
- 4 De Vriese AS, Heine G. Anticoagulation management in haemodialysis patients with atrial fibrillation: evidence and opinion. Nephrol Dial Transplant 2022; 37 (11) 2072-2079
- 5 Van Gelder IC, Rienstra M, Bunting KV. , et al. ; ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024; 45 (36) 3314-3414
- 6 Joglar JA, Chung MK, Armbruster AL. , et al. ; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024; 149 (01) e1-e156
- 7 Hindricks G, Potpara T, Dagres N. , et al. ; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021; 42 (05) 373-498
- 8 Chao TF, Joung B, Takahashi Y. et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive summary. Thromb Haemost 2022; 122 (01) 20-47
- 9 Reinecke H, Engelbertz C, Bauersachs R. et al. A randomized controlled trial comparing apixaban with the vitamin K antagonist phenprocoumon in patients on chronic hemodialysis: The AXADIA-AFNET 8 Study. Circulation 2023; 147 (04) 296-309
- 10 De Vriese AS, Caluwé R, Van Der Meersch H, De Boeck K, De Bacquer D. Safety and efficacy of vitamin K antagonists versus rivaroxaban in hemodialysis patients with atrial fibrillation: a multicenter randomized controlled trial. J Am Soc Nephrol 2021; 32 (06) 1474-1483
- 11 Pokorney SD, Chertow GM, Al-Khalidi HR. , et al. ; RENAL-AF Investigators. Apixaban for patients with atrial fibrillation on hemodialysis: a multicenter randomized controlled trial. Circulation 2022; 146 (23) 1735-1745
- 12 Harel Z, Smyth B, Badve SV. et al. Anticoagulation for patients with atrial fibrillation receiving dialysis: a pilot randomized controlled trial. J Am Soc Nephrol 2025; 36 (05) 901-910
- 13 Elfar S, Elzeiny SM, Ismail H, Makkeyah Y, Ibrahim M. Direct oral anticoagulants vs. warfarin in hemodialysis patients with atrial fibrillation: a systematic review and meta-analysis. Front Cardiovasc Med 2022; 9: 847286
- 14 Kuno T, Takagi H, Ando T. et al. Oral anticoagulation for patients with atrial fibrillation on long-term hemodialysis. J Am Coll Cardiol 2020; 75 (03) 273-285
- 15 Chen X, Zhu W, Lin M. Comparison of factor X inhibitors versus vitamin K antagonists in atrial fibrillation patients on dialysis. Eur J Intern Med 2024; 127: 154-156
- 16 Higgins J, Thomas J, Chandler J. , et al. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated August 2024). Cochrane, 2024. . Accessed March 4, 2025; available at: www.training.cochrane.org/handbook
- 17 Page MJ, McKenzie JE, Bossuyt PM. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372 (71) n71
- 18 Sterne JAC, Savović J, Page MJ. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898
- 19 Guyatt GH, Oxman AD, Vist GE. et al; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008; 336 (7650) 924-926
- 20 Lip G, Freedman B, De Caterina R, Potpara TS. Stroke prevention in atrial fibrillation: Past, present and future. Comparing the guidelines and practical decision-making. Thromb Haemost 2017; 117 (07) 1230-1239
- 21 Zimmerman D, Sood MM, Rigatto C, Holden RM, Hiremath S, Clase CM. Systematic review and meta-analysis of incidence, prevalence and outcomes of atrial fibrillation in patients on dialysis. Nephrol Dial Transplant 2012; 27 (10) 3816-3822
- 22 Shen JI, Winkelmayer WC. Use and safety of unfractionated heparin for anticoagulation during maintenance hemodialysis. Am J Kidney Dis 2012; 60 (03) 473-486
- 23 Steffel J, Collins R, Antz M. et al; External reviewers. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021; 23 (10) 1612-1676
- 24 Mavrakanas TA, Charytan DM, Winkelmayer WC. Direct oral anticoagulants in chronic kidney disease: an update. Curr Opin Nephrol Hypertens 2020; 29 (05) 489-496
- 25 Seliger SL, Gillen DL, Longstreth Jr WT, Kestenbaum B, Stehman-Breen CO. Elevated risk of stroke among patients with end-stage renal disease. Kidney Int 2003; 64 (02) 603-609
- 26 Jobski K, Hoffmann F, Herget-Rosenthal S, Dörks M. Use of oral anticoagulants in German nursing home residents: drug use patterns and predictors for treatment choice. Br J Clin Pharmacol 2018; 84 (03) 590-601
- 27 Haas S, Camm JA, Harald D. , et al. ; GARFIELD-AF Investigators. GARFIELD-AF: risk profiles, treatment patterns and 2-year outcomes in patients with atrial fibrillation in Germany, Austria and Switzerland (DACH) compared to 32 countries in other regions worldwide. Clin Res Cardiol 2023; 112 (06) 759-771
- 28 Verhoef TI, Redekop WK, Daly AK, van Schie RM, de Boer A, Maitland-van der Zee AH. Pharmacogenetic-guided dosing of coumarin anticoagulants: algorithms for warfarin, acenocoumarol and phenprocoumon. Br J Clin Pharmacol 2014; 77 (04) 626-641
- 29 Schlöglhofer T, Marschütz A, Combs P. et al. Quality of anticoagulation with phenprocoumon and warfarin in left ventricular assist device patients: A multicenter study. ASAIO J 2023; 69 (06) 595-601
- 30 Yang F, Hellyer JA, Than C. et al. Warfarin utilisation and anticoagulation control in patients with atrial fibrillation and chronic kidney disease. Heart 2017; 103 (11) 818-826
- 31 Ocak G, Noordzij M, Rookmaaker MB. et al. Mortality due to bleeding, myocardial infarction and stroke in dialysis patients. J Thromb Haemost 2018; 16 (10) 1953-1963
- 32 Pokorney SD, Black-Maier E, Hellkamp AS. et al. Oral anticoagulation and cardiovascular outcomes in patients with atrial fibrillation and end-stage renal disease. J Am Coll Cardiol 2020; 75 (11) 1299-1308
- 33 Kang DS, Yang PS, Kim D. et al. Racial differences in bleeding risk: An ecological epidemiological study comparing Korea and United Kingdom subjects. Thromb Haemost 2024; 124 (09) 842-851
- 34 Kang DS, Yang PS, Kim D. et al. Racial differences in ischemic and hemorrhagic stroke: An ecological epidemiological study. Thromb Haemost 2024; 124 (09) 883-892
Address for correspondence
Publication History
Received: 09 January 2025
Accepted: 22 February 2025
Accepted Manuscript online:
24 February 2025
Article published online:
24 March 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Wizemann V, Tong L, Satayathum S. et al. Atrial fibrillation in hemodialysis patients: clinical features and associations with anticoagulant therapy. Kidney Int 2010; 77 (12) 1098-1106
- 2 Yang F, Chou D, Schweitzer P, Hanon S. Warfarin in haemodialysis patients with atrial fibrillation: what benefit?. Europace 2010; 12 (12) 1666-1672
- 3 De Vriese AS, Caluwé R, Raggi P. The atrial fibrillation conundrum in dialysis patients. Am Heart J 2016; 174: 111-119
- 4 De Vriese AS, Heine G. Anticoagulation management in haemodialysis patients with atrial fibrillation: evidence and opinion. Nephrol Dial Transplant 2022; 37 (11) 2072-2079
- 5 Van Gelder IC, Rienstra M, Bunting KV. , et al. ; ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024; 45 (36) 3314-3414
- 6 Joglar JA, Chung MK, Armbruster AL. , et al. ; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024; 149 (01) e1-e156
- 7 Hindricks G, Potpara T, Dagres N. , et al. ; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021; 42 (05) 373-498
- 8 Chao TF, Joung B, Takahashi Y. et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive summary. Thromb Haemost 2022; 122 (01) 20-47
- 9 Reinecke H, Engelbertz C, Bauersachs R. et al. A randomized controlled trial comparing apixaban with the vitamin K antagonist phenprocoumon in patients on chronic hemodialysis: The AXADIA-AFNET 8 Study. Circulation 2023; 147 (04) 296-309
- 10 De Vriese AS, Caluwé R, Van Der Meersch H, De Boeck K, De Bacquer D. Safety and efficacy of vitamin K antagonists versus rivaroxaban in hemodialysis patients with atrial fibrillation: a multicenter randomized controlled trial. J Am Soc Nephrol 2021; 32 (06) 1474-1483
- 11 Pokorney SD, Chertow GM, Al-Khalidi HR. , et al. ; RENAL-AF Investigators. Apixaban for patients with atrial fibrillation on hemodialysis: a multicenter randomized controlled trial. Circulation 2022; 146 (23) 1735-1745
- 12 Harel Z, Smyth B, Badve SV. et al. Anticoagulation for patients with atrial fibrillation receiving dialysis: a pilot randomized controlled trial. J Am Soc Nephrol 2025; 36 (05) 901-910
- 13 Elfar S, Elzeiny SM, Ismail H, Makkeyah Y, Ibrahim M. Direct oral anticoagulants vs. warfarin in hemodialysis patients with atrial fibrillation: a systematic review and meta-analysis. Front Cardiovasc Med 2022; 9: 847286
- 14 Kuno T, Takagi H, Ando T. et al. Oral anticoagulation for patients with atrial fibrillation on long-term hemodialysis. J Am Coll Cardiol 2020; 75 (03) 273-285
- 15 Chen X, Zhu W, Lin M. Comparison of factor X inhibitors versus vitamin K antagonists in atrial fibrillation patients on dialysis. Eur J Intern Med 2024; 127: 154-156
- 16 Higgins J, Thomas J, Chandler J. , et al. (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated August 2024). Cochrane, 2024. . Accessed March 4, 2025; available at: www.training.cochrane.org/handbook
- 17 Page MJ, McKenzie JE, Bossuyt PM. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372 (71) n71
- 18 Sterne JAC, Savović J, Page MJ. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898
- 19 Guyatt GH, Oxman AD, Vist GE. et al; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008; 336 (7650) 924-926
- 20 Lip G, Freedman B, De Caterina R, Potpara TS. Stroke prevention in atrial fibrillation: Past, present and future. Comparing the guidelines and practical decision-making. Thromb Haemost 2017; 117 (07) 1230-1239
- 21 Zimmerman D, Sood MM, Rigatto C, Holden RM, Hiremath S, Clase CM. Systematic review and meta-analysis of incidence, prevalence and outcomes of atrial fibrillation in patients on dialysis. Nephrol Dial Transplant 2012; 27 (10) 3816-3822
- 22 Shen JI, Winkelmayer WC. Use and safety of unfractionated heparin for anticoagulation during maintenance hemodialysis. Am J Kidney Dis 2012; 60 (03) 473-486
- 23 Steffel J, Collins R, Antz M. et al; External reviewers. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021; 23 (10) 1612-1676
- 24 Mavrakanas TA, Charytan DM, Winkelmayer WC. Direct oral anticoagulants in chronic kidney disease: an update. Curr Opin Nephrol Hypertens 2020; 29 (05) 489-496
- 25 Seliger SL, Gillen DL, Longstreth Jr WT, Kestenbaum B, Stehman-Breen CO. Elevated risk of stroke among patients with end-stage renal disease. Kidney Int 2003; 64 (02) 603-609
- 26 Jobski K, Hoffmann F, Herget-Rosenthal S, Dörks M. Use of oral anticoagulants in German nursing home residents: drug use patterns and predictors for treatment choice. Br J Clin Pharmacol 2018; 84 (03) 590-601
- 27 Haas S, Camm JA, Harald D. , et al. ; GARFIELD-AF Investigators. GARFIELD-AF: risk profiles, treatment patterns and 2-year outcomes in patients with atrial fibrillation in Germany, Austria and Switzerland (DACH) compared to 32 countries in other regions worldwide. Clin Res Cardiol 2023; 112 (06) 759-771
- 28 Verhoef TI, Redekop WK, Daly AK, van Schie RM, de Boer A, Maitland-van der Zee AH. Pharmacogenetic-guided dosing of coumarin anticoagulants: algorithms for warfarin, acenocoumarol and phenprocoumon. Br J Clin Pharmacol 2014; 77 (04) 626-641
- 29 Schlöglhofer T, Marschütz A, Combs P. et al. Quality of anticoagulation with phenprocoumon and warfarin in left ventricular assist device patients: A multicenter study. ASAIO J 2023; 69 (06) 595-601
- 30 Yang F, Hellyer JA, Than C. et al. Warfarin utilisation and anticoagulation control in patients with atrial fibrillation and chronic kidney disease. Heart 2017; 103 (11) 818-826
- 31 Ocak G, Noordzij M, Rookmaaker MB. et al. Mortality due to bleeding, myocardial infarction and stroke in dialysis patients. J Thromb Haemost 2018; 16 (10) 1953-1963
- 32 Pokorney SD, Black-Maier E, Hellkamp AS. et al. Oral anticoagulation and cardiovascular outcomes in patients with atrial fibrillation and end-stage renal disease. J Am Coll Cardiol 2020; 75 (11) 1299-1308
- 33 Kang DS, Yang PS, Kim D. et al. Racial differences in bleeding risk: An ecological epidemiological study comparing Korea and United Kingdom subjects. Thromb Haemost 2024; 124 (09) 842-851
- 34 Kang DS, Yang PS, Kim D. et al. Racial differences in ischemic and hemorrhagic stroke: An ecological epidemiological study. Thromb Haemost 2024; 124 (09) 883-892