

Subscribe to RSS
DOI: 10.1055/s-0036-1584203
Computed Tomographic Angiography for Cerebral Aneurysms in Spontaneous Subarachnoid Hemorrhage
Angiotomografia computadorizada para aneurismas cerebrais na hemorragia subaracnóidea espontâneaAuthors
Address for correspondence
Publication History
17 February 2016
23 March 2016
Publication Date:
18 May 2016 (online)


Abstract
Computed tomographic angiography (CTA) has recently gained popularity as an initial imaging test for spontaneous subarachnoid hemorrhage (SAH). This study evaluated 59 patients presenting aneurysmal SAH who underwent microsurgical clipping based on CTA findings alone and digital subtraction angiography (DSA) at postoperative follow-up. Multiple aneurysms were identified by CTA in 27% of patients and in 10% of patients, DSA identified aneurysms in addition to those diagnosed with CTA. The time between CTA and surgical treatment ranged from 0–4 days. Postoperative DSA revealed that 24% of patients had residual neck. The use of CTA alone may not be enough to detect small unruptured aneurysms in patients with multiple lesions or aneurysm remnants adjacent to an aneurysm clip. However, the advantages of CTA compared with DSA include its rapidity, reduced invasiveness, and lower cost, which allow us to proceed to ruptured aneurysm repair entirely on the basis of good-quality CTA studies.
Resumo
Angiotomografia computadorizada (ATC) ganhou popularidade como exame de imagem inicial na hemorragia subaracnoide (HSA). Este estudo retrospectivo, descritivo e observacional, avaliou 59 pacientes com HSA aneurismática. Todos foram submetidos à clipagem microcirúrgica apenas com base na ATC e no seguimento realizou-se avaliação com angiografia digital (AD). Em 27% dos pacientes encontramos múltiplos aneurismas na ATC e 10% tinham outros diferentes aneurismas diagnosticados pela AD. O intervalo entre ATC e tratamento cirúrgico variou de 0–4 dias. AD pós-operatória mostrou 24% dos pacientes com colo residual. A detecção de pequenos aneurismas não rotos em pacientes com múltiplos aneurismas e colo residual pós clipagem cirúrgica continuam a ser um problema quando a ATC é realizada isoladamente. No entanto, as vantagens da ATC incluem sua rapidez, menor invasão e custo, o que nos permite realizar o tratamento cirúrgico de aneurismas rotos apenas com os achados da ATC de boa qualidade.
Keywords
computed tomographic angiography - digital subtraction angiography - intracranial aneurysm - subarachnoid hemorrhagePalavras-chaves
angiotomografia computadorizada - angiografia digital por subtração - aneurisma intracraniano - hemorragia subaracnoideIntroduction
The high rebleeding rates following subarachnoid hemorrhage (SAH) warrant the diagnostic evaluation of its underlying causes. Aneurysmal SAH is a significant cause of morbidity and mortality, and its prompt and definitive treatment are crucial for the patient's outcome.[1] [2]
Cerebral digital subtraction angiography (DSA) is the gold standard for diagnosing ruptured aneurysms in patients presenting with spontaneous SAH. However, DSA is an invasive and time-consuming procedure and is associated with risks such as puncture site hematoma, contrast-induced nephropathy, and a less than 1% risk of permanent neurologic deficits.[2] [3] [4]
More recently, computed tomographic angiography (CTA) and three-dimensional (3D) CTA reconstruction have gained popularity as initial imaging tests in patients with SAH because of their reportedly high sensitivity and specificity for detecting ruptured aneurysms. The noninvasive nature of CTA and the ease and rapidity of their implementation are additional reasons for their acceptance in the workup of spontaneous SAH.[1] [2] [3]
This study sought to evaluate the use of CTA as the primary diagnostic tool for ruptured intracranial aneurysms and to assess whether aneurysm clipping can be safely based on CTA alone.
Material and Methods
This is a retrospective, descriptive, and observational cohort study involving 59 patients admitted to the neurosurgical vascular unit of our institution in the range of one year. Patients who had clinical symptoms of SAH confirmed by computed tomography (CT), Fisher II, III, and IV, or cerebrospinal fluid analysis, Fisher I, underwent CTA with 3D aneurysmal reconstruction on admission day.
We evaluated patients with suspected SAH with non-contrast CT. After SAH confirmation, all patients were submitted to 3D CTA using a General Electric Light-Speed Advantage CT scanner (General Electric, Milwaukee, WI, USA). Non-contrast CT scans were performed with 5 mm contiguous axial sections through the posterior fossa followed by 10 mm contiguous axial sections to the vertex. We performed CTA using an injection of nonionic contrast at a rate of 3 mL/s for 80 mL initiated with a 15-second pre-scan delay. A 1 mm collimated helical scan with a 1:1 pitch was obtained from the cavernous carotid cephalic for at least 3.5 cm. On average, a total dose of 24 g of iodine was administered. For all patients, a general radiologist processed and analyzed the images using an Advantage Windows 3D workstation (General Electric, Milwaukee, WI, USA) and a senior neuroradiologist confirmed findings.
CTA was the primary diagnostic and pretreatment planning exam performed in this group of patients presenting with SAH. After diagnosis, we performed microsurgical treatment (clipping) of the ruptured aneurysms in all patients. During the post-operative follow-up, DSA was used in all 59 patients to evaluate the presence of other aneurysms that may not have been identified with CTA as well as the residual neck of clipped aneurysms.
We recorded data on spreadsheets and saved them in a database developed for the study. These included patient characteristics such as gender and age, clinical and radiological features, aneurysms identified by CTA and DSA, aneurysms undiagnosed by CTA and identified by DSA, aneurysm location, and presence of residual neck.
Data were subjected to descriptive analyses performed with the SPSS software, version 22. The project was approved by our department's ethics committee.
Results
This study examined a total of 59 patients with SAH by ruptured cerebral aneurysm that underwent surgical treatment using 3D-CTA for diagnosis and preoperative planning. Mean age was 48.85 ± 12.08 years (range: 18–85 years) and 46 patients (78%) were over 40 years old. Twenty-eight were men (47%) and 31 were women (53%).
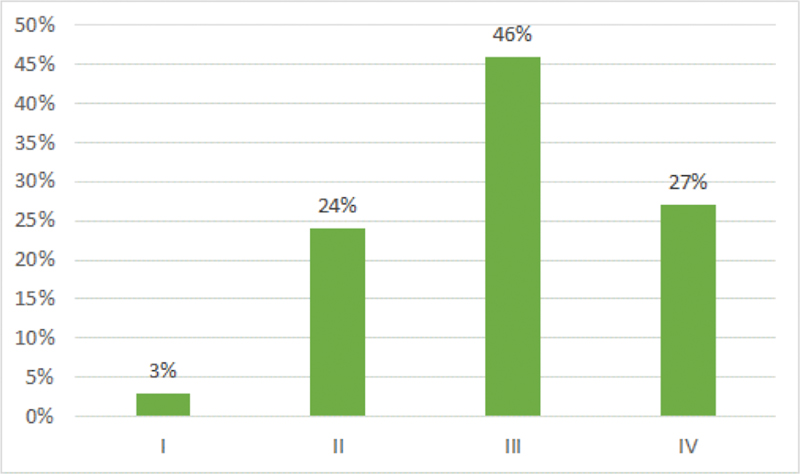
Twenty-seven patients (46%) in this study presented as Fisher III, 16 patients (27%) as Fisher IV, 14 (24%) as Fisher II, and two patients (3%) as Fisher I ([Fig. 1]).
We found the following distribution for the location of operated aneurysms identified by CTA ([Table 1]): communicating anterior artery (AComA): 24 patients (41%); middle cerebral artery (MCA): 20 patients (34%); posterior communicating artery (PComA): 14 patients (24%); pericallosal: 2 (3%); beyond the amount of additional unruptured aneurysms seen by CTA ([Table 1]). In 16 patients (27%), CTA identified multiple aneurysms.
Abbreviations: AComA, communicating anterior artery; ICA, internal carotid artery; MCA, middle cerebral artery; PComA, posterior communicating artery.
The interval between 3D-CTA and surgical treatment ranged from 0 (surgery performed on the day of admission) to four days, with a median of one day.
DSA was performed during the late postoperative period and 53 patients (90%) showed no new aneurysms, while the remaining 10% had aneurysms that were not detected originally, all of them smaller than 3mm.
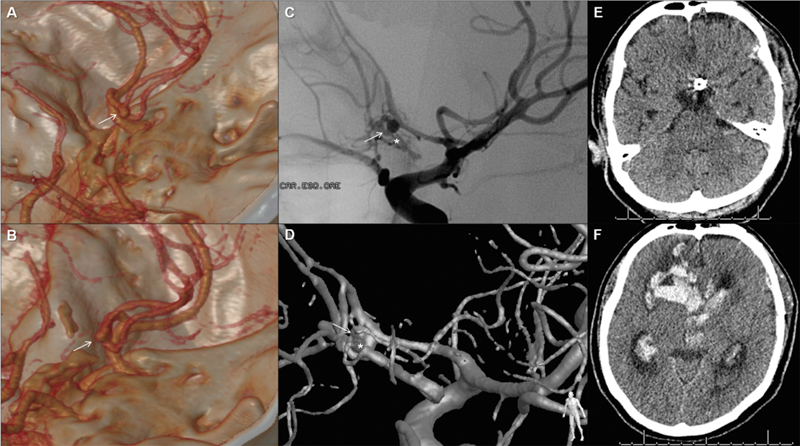
In addition, DSA showed residual neck in 14 patients (24%): 5 were intentional due to intraoperative technical difficulties, and 9 were unintentional (5 in AComA and 4 in PComA). Among these 14 patients, 10 were treated expectantly, 2 were treated electively (one by endovascular approach and the other by microsurgical repositioning of the clip; both were without residual neck after these procedures) and two patients had rebleeding from the residual neck for up to 30 days. Of these last two patients, one was an AComA aneurysm residual neck and the patient died from rebleeding complication ([Fig. 2]), while the other was an MCA aneurysm residual neck that required reoperation to reposition the clip and evacuate a temporal lobe hematoma (SAH Fisher IV). Residual neck was observed according to the following distribution: AComA: 6 patients (43%); PComA: 4 patients (29%); MCA: 3 patients (21%); and Carotid cave: one patient (7%) ([Fig. 3]).

Discussion
Aneurysms are one of the most important causes of SAH, accounting for roughly 75 to 85% of cases, with a fatality rate between 40 and 60%. Misdiagnosis is associated with further increased morbidity and mortality. The advent of CTA has changed the ease and promptness with which treating physicians can identify and characterize a ruptured intracranial aneurysm. As a result, the use of CTA as the initial screening test for an aneurysm in the setting of a spontaneous SAH has been increasing.[1] [5]
DSA is the gold standard for the assessment of intracranial aneurysms and for the preoperative treatment planning of patients suffering from SAH.[2] [4] [6] Results obtained with DSA are considered to be definite, although the reported rate of negative angiography in SAH ranges from 10 to 20%. Nonetheless, DSA is an invasive imaging method and may be time-consuming; moreover, it is operator-dependent and carries a 4% complication risk with 1% rate of persistent neurologic deficits. In addition, the resulting subtracted images may sometimes fail to delineate important morphological features of the aneurysm that facilitate the neurosurgeon's ability to perform a safe operation, such as the neck, vessels arising from the sac, and mural calcifications or luminal thrombus.[1] [2] [6]
In our study, patients underwent 3D-CTA immediately after SAH detection. The time between 3D-CTA and surgery ranged from 0 to 4 days, with a median of one day. This is an important issue in aneurysmal SAH, since rebleeding and vasospasms are severe early complications that directly influence morbidity and mortality. Therefore, definitively treating aneurysms as fast as possible can help avoid rebleeding and treat vasospasms more aggressively.
3D-CTA allows three-dimensional visualization of the aneurysmal neck, the anatomic relationships between skull base bones and the aneurysm, as well as aneurysms in deep planes, thus facilitating the surgical approach ([Fig. 4]).[2] [3] [7] CTA is a rapid, minimally invasive, and convenient method of detecting cerebral aneurysms after a plain CT scan identifies a SAH. In some patients, the quality of the CTA images is good enough to avoid the risks, delays, and costs associated with DSA.[8] [9]

The literature presents a wide range of sensitivity (70–100%) and specificity (50–100%) values for the detection of aneurysms with 3D-CTA.[2] For example, in a series of 40 patients with SAH, Anderson et al[9] reported sensitivity and specificity of 86 and 90%, respectively. Vieco et al[10] reported sensitivity of 97% and specificity of 100%. In a series of 113 patients, Wang et al[4] reported sensitivity and specificity values of 98.9 and 100%, respectively. Pechlivanis et al[2] reported a strong correlation between CTA and intra-operative findings in 92 of 100 patients, as well as between CTA and DSA in 60 of 61 patients (98%). Finally, CTA and DSA had equal sensitivity for the detection of intracranial aneurysms >3 mm in a study by Karamessini et al.[6]
The main disadvantage of CTA is its low sensitivity for detecting small aneurysms (<3 mm). In our study, six patients (10%) had aneurysms detected by DSA which had been missed with CTA. These aneurysms were mainly incidental discoveries on postoperative DSA, and in no patients did they require treatment. Also, CTA does not facilitate the delineation of perforating arteries smaller, which are less than 1.0mm in diameter (the recurrent artery of Heubner, the anterior choroidal artery, and thalamoperforating arteries),[2] [7] [8] [9] and cannot be used to determine aneurysm fillings.[2] [9]
While some believe that incomplete aneurysm treatment may result in recurrent hemorrhage with serious or fatal consequences, others have suggested that 1- to 2-mm residual necks seen in postoperative DSA pose little risk.[11] In recent years, several cases have been presented in which this seemingly unimportant remnant of the neck dilated to become a dangerous aneurysm.[11] [12]
Postoperative DSA is routinely used to evaluate patients who have undergone surgical obliteration of an aneurysm. It provides information on the results of clipping, the presence of residual unclipped aneurysms, other unclipped aneurysms, and the occlusion of major vessels.[11] [12] [13] In a series of 102 patients harboring a total of 167 aneurysms, David et al[12] found a small but significant risk of de novo aneurysm formation, particularly in patients with multiple aneurysms. Most residual aneurysms appear to remain stable, although a subset may enlarge or rupture. These findings support the rationale for late angiographic follow-up in patients with aneurysms. In our study, we found 14 patients (24%) with residual neck (9 unintentional). Of these patients, two had rebleeding and severe complications, and one patient died ([Fig. 2]).
Although many authors have reported that 3D-CTA can be used instead of DSA in all but a few cases, very few centers use CTA as the primary diagnostic tool in daily routine for planning aneurysm surgery. The percentage of patients who have been operated solely based on 3D-CTA data in centers across the world ranges between 33% and 93%.[2] [4] [5]
Limitations
The reliability of the radiological findings in our study could have been improved by having two or more neuroradiologists evaluating each image. Also, a detailed comparative analysis of aneurysm morphology would have allowed us to better understand the role of CTA. Unfortunately, the retrospective nature of our study did not give us access to this type of information. Despite these limitations, we believe our results provide preliminary yet valuable information regarding the use of CTA for SAH patients. Future studies with larger numbers of patients and blind comparisons should be conducted to address the questions beyond the scope of the present study.
Conclusions
When good quality CTA images are available for SAH, it is possible to proceed with ruptured aneurysm repair. However, detection of small unruptured aneurysms in patients with multiple lesions and aneurysm remnants adjacent to an aneurysm clip remain a problem. The advantages of CTA compared with DSA include its rapidity, reduced invasiveness, and lower cost.
Based on these observations, it is our continued practice to operate on the basis of CTA alone in most cases. In fact, we believe postoperative DSA should be mandatory for all patients. It is likely that continued refinement of CTA and greater experience with its use will increase its sensitivity for detecting small aneurysms.
-
References
- 1 Jethwa PR, Gandhi CD, Prestigiacomo CJ. Cost-effectiveness of computed tomographic angiography in screening for aneurysm in spontaneous subarachnoid hemorrhage. Neurosurgery 2014; 61 (Suppl. 01) 137-144
- 2 Pechlivanis I, Schmieder K, Scholz M, König M, Heuser L, Harders A. 3-Dimensional computed tomographic angiography for use of surgery planning in patients with intracranial aneurysms. Acta Neurochir (Wien) 2005; 147 (10) 1045-1053 , discussion 1053
- 3 Franklin B, Gasco J, Uribe T, VonRitschl RH, Hauck E. Diagnostic accuracy and inter-rater reliability of 64-multislice 3D-CTA compared to intra-arterial DSA for intracranial aneurysms. J Clin Neurosci 2010; 17 (5) 579-583
- 4 Wang YC, Liu YC, Hsieh TC, Lee ST, Li ML. Aneurysmal subarachnoid hemorrhage diagnosis with computed tomographic angiography and OsiriX. Acta Neurochir (Wien) 2010; 152 (2) 263-269 , discussion 269
- 5 McKinney AM, Palmer CS, Truwit CL, Karagulle A, Teksam M. Detection of aneurysms by 64-section multidetector CT angiography in patients acutely suspected of having an intracranial aneurysm and comparison with digital subtraction and 3D rotational angiography. AJNR Am J Neuroradiol 2008; 29 (3) 594-602
- 6 Karamessini MT, Kagadis GC, Petsas T , et al. CT angiography with three-dimensional techniques for the early diagnosis of intracranial aneurysms. Comparison with intra-arterial DSA and the surgical findings. Eur J Radiol 2004; 49 (3) 212-223
- 7 Kato Y, Sano H, Katada K , et al. Application of three-dimensional CT angiography (3D-CTA) to cerebral aneurysms. Surg Neurol 1999; 52 (2) 113-121 , discussion 121–122
- 8 Anderson GB, Steinke DE, Petruk KC, Ashforth R, Findlay JM. Computed tomographic angiography versus digital subtraction angiography for the diagnosis and early treatment of ruptured intracranial aneurysms. Neurosurgery 1999; 45 (6) 1315-1320 , discussion 1320–1322
- 9 Anderson GB, Findlay JM, Steinke DE, Ashforth R. Experience with computed tomographic angiography for the detection of intracranial aneurysms in the setting of acute subarachnoid hemorrhage. Neurosurgery 1997; 41 (3) 522-527 , discussion 527–528
- 10 Vieco PT, Shuman WP, Alsofrom GF, Gross CE. Detection of circle of Willis aneurysms in patients with acute subarachnoid hemorrhage: a comparison of CT angiography and digital subtraction angiography. AJR Am J Roentgenol 1995; 165 (2) 425-430
- 11 Lin T, Fox AJ, Drake CG. Regrowth of aneurysm sacs from residual neck following aneurysm clipping. J Neurosurg 1989; 70 (4) 556-560
- 12 David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg 1999; 91 (3) 396-401
- 13 Macdonald RL, Wallace MC, Kestle JRW. Role of angiography following aneurysm surgery. J Neurosurg 1993; 79 (6) 826-832
Address for correspondence
-
References
- 1 Jethwa PR, Gandhi CD, Prestigiacomo CJ. Cost-effectiveness of computed tomographic angiography in screening for aneurysm in spontaneous subarachnoid hemorrhage. Neurosurgery 2014; 61 (Suppl. 01) 137-144
- 2 Pechlivanis I, Schmieder K, Scholz M, König M, Heuser L, Harders A. 3-Dimensional computed tomographic angiography for use of surgery planning in patients with intracranial aneurysms. Acta Neurochir (Wien) 2005; 147 (10) 1045-1053 , discussion 1053
- 3 Franklin B, Gasco J, Uribe T, VonRitschl RH, Hauck E. Diagnostic accuracy and inter-rater reliability of 64-multislice 3D-CTA compared to intra-arterial DSA for intracranial aneurysms. J Clin Neurosci 2010; 17 (5) 579-583
- 4 Wang YC, Liu YC, Hsieh TC, Lee ST, Li ML. Aneurysmal subarachnoid hemorrhage diagnosis with computed tomographic angiography and OsiriX. Acta Neurochir (Wien) 2010; 152 (2) 263-269 , discussion 269
- 5 McKinney AM, Palmer CS, Truwit CL, Karagulle A, Teksam M. Detection of aneurysms by 64-section multidetector CT angiography in patients acutely suspected of having an intracranial aneurysm and comparison with digital subtraction and 3D rotational angiography. AJNR Am J Neuroradiol 2008; 29 (3) 594-602
- 6 Karamessini MT, Kagadis GC, Petsas T , et al. CT angiography with three-dimensional techniques for the early diagnosis of intracranial aneurysms. Comparison with intra-arterial DSA and the surgical findings. Eur J Radiol 2004; 49 (3) 212-223
- 7 Kato Y, Sano H, Katada K , et al. Application of three-dimensional CT angiography (3D-CTA) to cerebral aneurysms. Surg Neurol 1999; 52 (2) 113-121 , discussion 121–122
- 8 Anderson GB, Steinke DE, Petruk KC, Ashforth R, Findlay JM. Computed tomographic angiography versus digital subtraction angiography for the diagnosis and early treatment of ruptured intracranial aneurysms. Neurosurgery 1999; 45 (6) 1315-1320 , discussion 1320–1322
- 9 Anderson GB, Findlay JM, Steinke DE, Ashforth R. Experience with computed tomographic angiography for the detection of intracranial aneurysms in the setting of acute subarachnoid hemorrhage. Neurosurgery 1997; 41 (3) 522-527 , discussion 527–528
- 10 Vieco PT, Shuman WP, Alsofrom GF, Gross CE. Detection of circle of Willis aneurysms in patients with acute subarachnoid hemorrhage: a comparison of CT angiography and digital subtraction angiography. AJR Am J Roentgenol 1995; 165 (2) 425-430
- 11 Lin T, Fox AJ, Drake CG. Regrowth of aneurysm sacs from residual neck following aneurysm clipping. J Neurosurg 1989; 70 (4) 556-560
- 12 David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg 1999; 91 (3) 396-401
- 13 Macdonald RL, Wallace MC, Kestle JRW. Role of angiography following aneurysm surgery. J Neurosurg 1993; 79 (6) 826-832