

Subscribe to RSS
DOI: 10.1055/s-0036-1586218
Prognostic Predictors of Decompressive Craniectomy in Traumatic Brain Injury: A Clinical Experience of 128 Cases
Authors
Address for correspondence
Publication History
22 March 2016
21 June 2016
Publication Date:
10 August 2016 (online)


Abstract
Objectives The objective of this study was to analyze different parameters such as clinicoradiological presentation, surgical outcome, and factors associated with prognosis of traumatic brain injury patients undergoing decompressive craniectomy (DC).
Materials and Methods This observational study was done on all the cases of DC undertaken in our hospital during July 2013 to June 2015. In all cases, the age, sex, mode of injury, severity of injury, associated injuries, indications, computed tomography (CT) finding, complications, and outcomes in the form of morbidity and mortality were analyzed.
Results Out of all head injury patients admitted, only 3.036% underwent DC. The most common age group affected was 19 to 40 years (n = 49; 43.75%; p-value < 0.001). Male to female ratio was 3.8:1; 66.07% presented with Glasgow coma scale (GCS) score ≤ 8. Pupillary abnormality was found in 34 (30.35%) patients. ASDH was the most common (n = 97; 86.66%) CT finding. Road traffic accident (RTA) was the most common mode of injury found in 69.64% of patients. Aspiration pneumonia and ventilator-associated pneumonia were the most common nonneurosurgical complication found in 14.28% of patients. Total number of deaths was 30 (26.78%). On analysis, patients with low admission GCS, pupillary dilatation, trauma due to RTA, associated injury, and aspiration pneumonia show high mortality (p < 0.05). Eighty-two (73.21%) patients survived and 54 (48.21%) patients discharged with good neurological condition.
Conclusion DC yields good results in traumatic brain injury. GCS score < 8, associated subarachnoid hemorrhage, midline shift, intraoperative brain bulge, associated chest injury and long bone fracture, cerebral infraction, old age > 40 years, male sex, alcoholics, pupillary dilation, and aspiration pneumonia are the independent factors for increased mortality and disability.
Keywords
decompressive craniectomy - good outcome - severe head injury - prognostic factors - clinicoradiological featuresIntroduction
Traumatic brain injury is one of the major health concerns causing morbidity and mortality in worldwide.[1] [2] It is currently a leading cause of death occurring in all kind of people irrespective of age, gender, different socioeconomic groups, in developed and developing countries.[3] Traumatic brain injury can be divided as localized or focal and diffuse injuries. The localized lesions, such as localized extradural hematoma, acute subdural hematoma, parenchymal hemorrhagic contusion, compound depressed fracture, etc., at specific sites are managed by localized craniotomy and decompression. All these cases with diffuse edema or multiple pathology produce raised intracranial pressure (ICP). These injuries may cause secondary insult causing raised ICP due to cerebral edema. Again, diffuse injury, such as multiple contusions, hemispheric or bilateral ASDH, diffuse axonal injury with cerebral edema, etc., causes both primary and secondary insults, producing cerebral edema and increased ICP in a vicious cycle ultimately yielding fatal outcome. Therefore, any lesion whether focal or diffuse produces raised ICP, which is the main factor predicting the outcome in a patient of traumatic brain injury (TBI). In many cases, the raised ICP is controlled by medical management alone or in combination with focal surgical intervention. In some cases, it is refractory to control ICP by the medical management.[1] [4] These cases are the ideal candidates for decompressive craniectomy (DC) with dural enhancement to allow the edematous bulging brain to enlarge and again subsided during the process of healing so as to be eligible for cranioplasty. It is not always mandatory to provide medical management to all before planning DC, it can be offered to patient of extensive parenchymal injury with edema or where expecting edema. In these cases, medical management should be used as a resuscitative measure to purchase time. Till date, DC is considered as a last resort in TBI to control the ICP.
In spite of different advent regarding DC, there are a lot of controversies about the procedure.[4] [5] Many authors described the effectiveness of DC producing good outcome,[6] [7] [8] [9] and some described about ineffectiveness or poor outcome.[5] [10] There are no supportive class I evidences and still it is a matter of debate with controversies, though a lot of neurosurgeons are adopting it. We conducted this study to analyze the different parameters such as demographic profile, clinical presentation, radiological features, mode of injury, types of injury, indications, surgical techniques, intraoperative findings, and outcome analysis to add some rays in the evidence-based surgery with review of literatures.
Materials and Methods
This observational study was conducted on all the patients of head injury who underwent DC during the period of July 2013 to June 2015 (2 years). All the patients irrespective of age and severity of injury, on whom DC was undertaken, were included in this study. The exclusion criteria were (1) patients underwent DC for other nontraumatic conditions such as tumors causing intraoperative brain swelling. (2) Patients underwent DC but whose follow-up and cranioplasty were not done in our hospital. (3) Patients left the hospital against the medical advice after DC were done.
A total of 4,128 patients of head injury were admitted to our hospital during the period of July 2013 to June 2015. Out of these, 128 cases of head injury patient underwent DC. In all cases, age, sex, initial presenting sign and symptoms at casualty, mechanism of injury, radiological diagnosis, severity of injury according to Glasgow coma scale (GCS), other associated injuries, preoperative condition, operative techniques, complications and difficulties, immediate postoperative condition, condition at discharge, length of hospital stay, outcome in the form of Glasgow outcome score (GOS), and follow-up conditions were recorded from the stored computerized master register, bed head tickets, computerized discharged tickets, patients profile, admission register and death register, etc. The patients underwent DC as per the standard protocol maintained in our department based on clinicoradiological parameters. The follow-up data were collected from outpatients visit and telephonic conversation personally. We used Microsoft Excel for data compilation and statistical analysis. Chi-square analysis was used to test the significance of the results and results were considered significant when p-value is < 0.05.
Course in the Hospital
All the patients were provided preoperative medical management before undertaking DC. After screening at emergency department, preoperative intensive care unit (ICU) facility was provided to only patients with very low GCS score or prehospital aspiration, airway obstruction, or chest injury. Other patients who needed intubation are intubated and left with “T” piece in the trauma ward. Around 32 patients out of 74 patients in the GCS score of 3 to 8 provided preoperative ICU care. No patient was put under ICP monitoring before or after surgery. All the patients were clinically and radiologically evaluated for raised ICP and taken for DC. The clinical and radiological features taken as a guide for DC were as follows: (1) admitted with low GCS score and deteriorating neurologically or admitted with good GCS score but deteriorated subsequently, (2) initial midline shift of > 0.5 cm or thickness of ASDH > 1 cm with cerebral edema, (3) increasing midline shift and edema in repeat CT, (4) hemispheric frontotemporoparietal (F-T-P) contusion with mass effect and edema, (5) compound depressed fracture with underlying hemispheric contusion, ASDH, and mass effect, (6) above injuries with dilated and sluggishly reacting unilateral or bilateral pupil with bradycardia, (7) increased area of contusion and ASDH in repeat CT scans with diffuse cerebral edema, (8) the patients having moderate head injuries whose GCS score decreased by 2 to 3 points despite adequate antiedema measures to control ICP and radiological deterioration were taken for DC, and (9) uncontrollable brain swelling during craniotomy and surgery for other traumatic parenchymal lesions where DC was not planned earlier and undertaken incidentally.
We managed all the patients with our maintained protocol from emergency department up to ward and ICU. (1) ABC (airway, breathing, circulation) management includes endotracheal intubation, tracheostomy, O2 inhalation, circulation by normal saline, and ringer lactate. (2) Head rising position 30 to 45 degrees, catheterization of bladder, neutral position of head, avoidance of neck compression, and exclusion of other injuries, if needed whole blood transfusion preoperatively during or after operation. (3) Initial GCS assessment and subsequent 6 hourly assessments. (4) If ICU needed, then management at ICU was as per availability. (5) Complete blood investigation (HIV, HCV, HBSAg, DC, TLC, Hb%, PCV, Na+, K+, urea, and creatinine). (6) If planned for medical management, then aim was to evaluate the patient in ICU 4 hourly and 6 hourly in the ward for further deterioration/raised ICP. (7) Repeat CT scans as per need if deteriorated or routinely in every 72 hours. (8) In cases requiring immediate DC with management of pathologies, then surgery as per need with resuscitative measures and ICP lowering intravenous mannitol to buy time. (9) Continuous observation was done to control ICP by targeting systolic blood pressure (SBP) > 90 mm Hg, SPo 2 > 95%, and serum sodium between 145 and 155 MEq/L. (10) In our cases, we have used only 20% mannitol, 3% sodium chloride, furosemide, and sedation with lorazepam to control ICP. In no case, we used hyperventilation, or other sedatives such as propofol to control ICP except during intraoperative brain swelling. (11) In no cases, we used ICP monitor. (12) Clinicoradiological features were taken as guide for management. (13) Despite of these medical managements, refractory cases underwent DC.
Surgery was undertaken with written consent from the responsible attendants. The laterality of DC was decided by pathology concerned. Unilateral F-T-P DC was undertaken in 110 patients, whereas bilateral F-T-P DC was undertaken in only 2 cases. In no cases, we have done bilateral frontal DC. The extent of craniectomy was approximately 12 to 15 cm long in anteroposterior direction. The superior limit is approximately 2 to 3 cm away from midline vertex and at base always reaching the floor of the temporal fossa at the origin of zygomatic arch. The pathology was properly addressed like evacuation of ASDH and excision of contusion. In seven cases, interoptic cerebrospinal fluid (CSF) arachnoid cistern was punctured and drained in patients where brain is not relaxed and visible pulsation was not seen. Lax dural closure were done using G-dura patch in star-shaped manner in all cases. The free bone flaps were kept in subcutaneous abdominal pocket in most of the cases and discarded in nine cases of delayed contaminated compound depressed fracture, which underwent DC. About 36 cases needed tracheostomy during hospitalization from emergency department up to discharge from hospital. The cranioplasty was done with native bone preserved in abdominal pocket and in some cases, where bone found short titanium mesh was combined for better repair. In patients with discarded bones, titanium mesh repair was done. Out of 82 survivals, in 54 (65.85%) patients, cranioplasty was undertaken after 6 weeks up to 6 months postoperative.
Results
Demographic Profile
The total number of patients admitted with head injury during the period of July 2013 to June 2015 was 4,216. Out of these, only 128 (3.036%) cases underwent DC for TBI. Of these during the postoperative period of hospitalization, 5 patients left the hospital against the medical advice to some other hospitals, and 11 patients lost to follow-up after discharge from the hospital. Therefore, a total of 112 patients were included in this study.
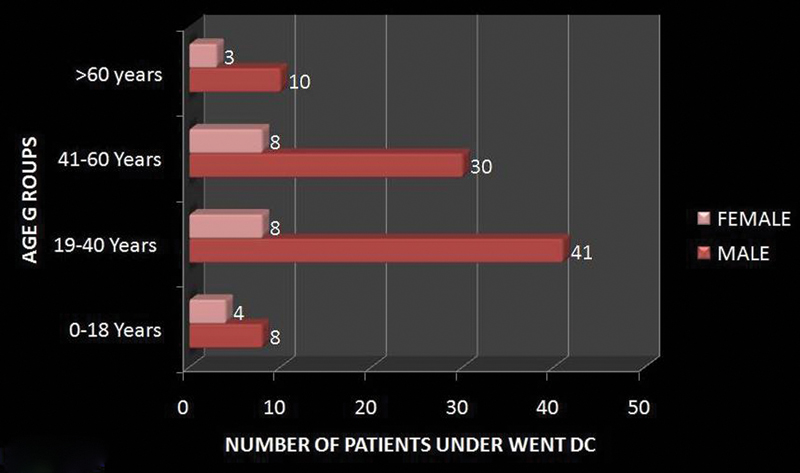
The patients who underwent DCs were divided into four groups: 0 to 18 years (pediatrics), 19 to 40 years (adults), 41 to 60 years (elderly), and > 60 years (old), for more specific agewise analysis and better understanding of clinicopathology. Number of patients in each group was 12 (10.71%), 49 (43.75%), 38 (33.92%), and 13 (11.60%) in the age group of 0 to 18, 19 to 40, 40 to 60, and > 60 years, respectively. The youngest age of patient who underwent DC in our study was a 14-year-old boy and oldest age of patient was a 77-year-old man. Most of the persons with head injury needing DC were in the age group of 19 to 40 years (p-value < 0.001). Male to female ratio was 3.8:1 with 79.46% (n = 89) males and 20.53% (n = 23) females. Males in the age group of 19 to 40 years were more affected than females with a ratio of 5.12:1. However, females in the age group of 0 to 18 years found more affected than the other group of females in a ratio of 1:2. The detail of age and sex distribution is given in [Fig. 1].
Presenting Features
In our study, the most common presentation was altered sensorium found in all cases. The agewise details of the different parameters are described in [Table 1].
Abbreviation: GCS, Glasgow coma scale.
Types of Injury (Radiological Features)
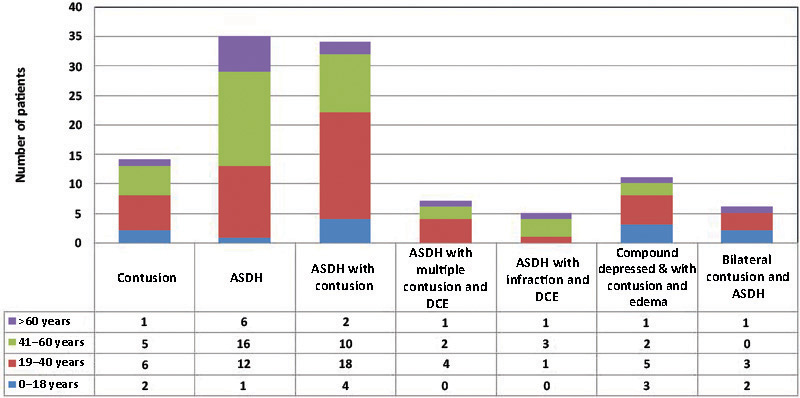
It is found that ASDH was the most common CT finding found in patients who underwent DC. ASDH along with contusion, multiple contusion, and compound depressed fracture with contusion, SAH, or other lesion such as extradural hematoma and diffuse cerebral edema was found in 97 (86.66%) cases. However, ASDH alone with diffuse cerebral edema and mass effect was responsible for 35 (31.25%) cases. On further study, it is found that ASDH alone was the most common pathology needing DC in the age group of 41 to 60 years and older than 60 years, whereas ASDH with underlying contusion was the most common CT finding needing DC in the age group of 19 to 40 years. The details of types of injury are given in [Fig. 2] and [Table 2].
Abbreviations: CT, computed tomography; RTA, road traffic accident.
Associated Injuries
After necessary screening at casualty during admission, patients requiring active neurosurgical intervention despite of having other associated injuries were admitted to neurotrauma department after primary care given by the concerned departments. As a result, there were 30 patients admitted with other associated injuries along with head injury underwent DC. Facial injury was the most common associated injury found in 17 patients. Fracture of clavicle was found in eight patients, long bone fracture was found in seven patients, and chest injury with fracture ribs was found in nine patients. The patients associated with fracture long bone and chest injuries showed more morbidity and mortality. Out of nine patients of chest injuries who underwent DC, five (55.55%) patients died in ICU, even after chest tube insertion, and out of seven patients of long bone fractures, three (42.85%) patients died during their postoperative hospital stay. The details of other associated injury are shown in [Table 2].
Modes of Injury
The most common mode of injury was road traffic accident (RTA) found in 78 (69.64%) patients, next to it was fall from height in 14 (12.50%) patients. Out of 78 patients, RTA under influence of alcohol was found in 24 cases. Fall on ground and assault was mostly found as a mode of injury in the age group of 41 to 60 years. Out of 49 patients, 40 (81.63%) in the age group of 19 to 40 years sustained head injury due to RTA, which was the most common group that encountered DC. The detail agewise modes of injury are shown in [Table 2].
Timing of Surgery since Trauma
The mean time interval from trauma to surgery was 64.28 hours (2.67 days), with shortest interval of 4 hours and longest interval of 336 hours (14 days). It is found that approximately 42 (37.5%) cases underwent surgery within 48 hours and 83 (74.10%) within 72 hours of trauma. Only 18 (16.07%) patients underwent DC within 24 hours. Around 102 (91.07%) of patients underwent DC within 5 days of trauma.
Complications
The most common and important intraoperative complication was brain swelling found in 23 (20.53%) patients. The postoperative complications are shown in [Table 3].
Abbreviation: CSF, cerebrospinal fluid; PCA, posterior cerebral artery; MCA, middle cerebral artery.
Duration of Hospitalization
The mean duration of hospital stay was 16.93 days, ranging from 7 to 58 days. This hospitalization period was only during the DC. During cranioplasty, rehospitalization was found in all cases. The mean postcranioplasty duration of hospitalization was 7 days, ranging from 5 to 27 days.
Follow-up
All the patients were followed up 1 monthly till cranioplasty and then at third month, sixth month, and 1 year. The average follow-up duration was 6 months ranging from 3 to 12 months.
Outcome and Mortality
Total number of deaths out of 4,216 TBI cases in our hospital were 618 (14.65%) during the period of study. However, the total number of deaths during the period of hospitalization in patient who underwent DC were 30 (26.78%) out of 112 cases, with male to female ratio of 7:3. The percentage of death found more in the age groups of > 60 is 38.46%; next to it was 41 to 60 years, 34.21%; 0 to 18 years, 25%; and 19 to 40 years, 18.36%.
The outcome was analyzed using GOS. The overall mortality in our study was (30/112) 26.78%. Eighty-two (73.21%) patients survived and 28 (34.14%) patients discharged from hospital with severe neurological compromise. Fifty-four (48.21%) patients discharged with good neurological condition so as to perform their daily activity. After discharge it was found that with better home care, all the patient of mild disability group and 40% of severe neurologically compromised patients improved to mild disability state at 3 months follow-up. Two patients from vegetative state group, 17-year-old man who underwent bilateral FTP decompression and 32-year-old man, were improved and now able to take orally by some assistant. It was found that two patients of severe disability group in the age group of 19 to 40 years, having hemiparesis improved after cranioplasty and doing his normal duties. It is found that patients presented with GCS score < 8, associated subarachnoid hemorrhage (SAH), midline shift, intraoperative brain bulge, associated chest injury and long bone fracture, cerebral infraction, old age > 40 years, male sex, alcoholics, and delayed cranioplasty have poor prognosis as compared with others. The outcome and mortality are described in [Table 4].
Abbreviations: GCS, Glasgow coma scale; GOS, Glasgow outcome score.
Prognostic Factors Analysis for Mortality
The different prognostic factors with their significance are described in [Table 5]. It is found that each parameter such as age between 19 and 40 years, male sex, RTA, pupillary abnormality, initial GCS, associated injuries, and intraoperative and postoperative complications constitutes individual risk factors for mortality and morbidity.
Abbreviations: CSF, cerebrospinal fluid; GCS, Glasgow coma scale; RTA, road traffic accident.
Discussion
DC is still a matter of debate in the management of uncontrollable raised ICP.[5] [6] [7] [8] [9] [10] Kocher in 1901 was the first person to propose DC as a palliative measure to control ICP in TBI having uncontrollable raised ICP.[11] Since then, there are a lot of controversies regarding the procedure.[5] [6] [7] [10] Till date, there has been no class I evidence related to DC for management of refractory raised ICP in TBI. However, currently, most of the neurosurgeons are practicing DC in TBI. This study is conducted to add some experiences encountered by us in this evidence-based surgery. As stated by Aarabi et al,[6] 10.7% of severe head injury patient underwent DC. In our study, it is found that approximately 3.036% of patient of TBI patient admitted underwent DC. This study correlates our finding as we included all patients irrespective of severity of injury, admitted as per the admission criteria.
In our study, we divided the patients who underwent DC into four groups: 0 to 18 years (pediatrics), 19 to 40 years (adults), 41 to 60 years (elderly), and > 60 (old) years for more specific, agewise analysis for better understanding of clinicopathology and outcome. It is found that most of the patients (43.7%) undergoing DC are adults in the age group of 19 to 40 years and next to it is in the age group of 41 to 60 years (33.92%). This may be due to the fact that these groups of persons are more exposed to outdoor activities and suffered severe head injury in a large numbers due to RTA. This is also compatible with the study done by Aarabi et al,[6] where they described as one half of the patient underwent DC was 22 to 46 years old. In our study, it is also found that none younger than the age of 14 years underwent DC. It suggests that pediatric head injuries are less severe and their brain and skull have better compliance than adult one.[12]
In our study, it is found that male to female ratio was 3.8:1 with 79.46% males and 20.53% females and it is also comparable to other studies.[6] [13] [14] [15] Males in the age group of 19 to 40 years are more affected than females with a ratio of 5.12:1. However, females in the age group of 0 to 18 years are more affected than other group of females in a ratio of 1:2. Therefore, it can be opined that occurrence of severe head injury is more among the male sex of the age group of 19 to 40 years, resulting more number of DCs.
In our study, the most common presentation was altered sensorium, found in all cases. It signifies that none of the patient with admission GCS score of 15/15 required DC. Therefore, it suggests that initial condition is also an independent factor for patients requiring DCs. Most of the patient who underwent DC had presenting GCS score of less than 12/15. More specifically, it can be described as two-thirds (66.07%) of the patients undergoing DCs have initial GCS of less than 8/15 (p-value < 0.05). This finding is also comparable with other study.[6] A very small proportion of patients from minor head injury group deteriorates and required the last resort, the DCs for their refractory raised ICP. In our study, vomiting was found in 67 (59.82%) patients. The bleeding from nose were found in 24 (21.42%) and bleeding from ear were found in 47 (41.96%) cases. Monoplegia was found in three cases and hemiplegia was found in two cases. Third nerve palsy was found in three cases. Posttraumatic immediate convulsion was found in six patients, whereas posttraumatic early convulsion was found in seven cases. Pupillary condition was found normal in most of our patient. Bilateral normal size and readily reacting to light pupils were found in around 78 (69.64%) patients. Remaining 34 (30.35%) patients showed pupillary abnormality. Out of these, 20 (17.85%) patients had unilateral dilated sluggishly reacting pupils, 9 (8.03%) had bilateral dilated sluggishly reacting pupils, and 5 patients had constricted less than 3 mm with sluggishly reacting pupils. It is seen that the patients with bilateral and unilateral dilated pupil in any type of head injury group such as severe or moderate showed highest mortality in comparison to patients having no pupillary abnormality (p-value < 0.05).
It is found that ASDH is the most common CT finding found in patients who underwent DC. ASDH along with contusion, multiple contusion, and compound depressed fracture with contusion, SAH, or other lesion such as extradural hematoma and diffuse cerebral edema was found in 97 (86.66%) cases. However, ASDH alone with diffuse cerebral edema and mass effect was responsible for 35 (31.25%) cases who underwent DC. On further study, it is found that ASDH with cerebral edema alone is the most common pathology needing DC in the age group of 41 to 60 years, whereas ASDH with underlying contusion was the most common CT finding needing DC in the age group of 19 to 40 years.
In our study, it is found that facial injury was the most common associated in patients undergoing DC. The patients associated with fracture long bone and chest injuries showed more morbidity and mortality (p-value < 0.05). About 55.55% of patients associated with chest injuries and 50% of patients with associated long bone fractures died in ICU among the patients undergoing DC.
In our study, it is also found that the most common mode of injury was RTA found in 69.64% patients, and next to it was fall from height in 112.50% patients. This is also comparable to other studies.[6] [14] [15] RTA under influence of alcohol was found in around one-third (30.76%) cases. Fall on ground and assault was mostly found as a mode of injury in the age group of 41 to 60 years. About 81.63% patients in the age group of 19 to 40 years suffered severe head injury due to RTA, which was the most common group encountered DC. It signifies that RTA (p-value < 0.05), alcoholism, and age group of 19 to 40 years suffered more severe head injury requiring more number of DCs.
In our study, it is found that all the patients were provided preoperative medical management before undertaking DC. No patient was put under ICP monitoring before or after surgery. Though some recent studies support use of ICP monitor in TBI is beneficial but a lot of studies described the use of ICP monitor does not have any impact on outcome. Haddad and Arabi described that although there is no randomized, controlled trial that has been performed demonstrating that ICP monitoring improves outcome or supporting its use as standard, ICP monitoring has become an integral part in the management of patients with severe TBI in most trauma centers. However, there is contradicting evidence about whether ICP monitoring improves outcome.[16] Several studies have demonstrated that ICP monitoring reduced the overall mortality rate of severe TBI.[17] [18] [19] [20] [21] Other studies have not shown any benefits from ICP monitoring.[22] [23] [24] Moreover, a few studies have demonstrated that ICP monitoring was associated with worsening of survival.[25] [26] Potential complications of ICP monitoring include infection, hemorrhage, malfunction, obstruction, or malposition. In the Cochrane database, a recent systematic review found no randomized control trials that can clarify the role of ICP monitoring in acute coma whether traumatic or nontraumatic.[26] Nevertheless, there is evidence, and most clinicians agree, to support the use of ICP monitoring in severe TBI patients at risk for intracranial hypertension. In a recent larger study done by Alkhoury and Kyriakides described that despite current Brain Trauma Foundation guidelines, ICP monitoring is used infrequently in the pediatric population. The data suggest that there is a small, yet statistically significant, survival advantage in patients who have ICP monitors and a GCS score of 3. However, all patients with ICP monitors experienced longer hospital length of stay, longer ICU stay, and more ventilator days compared with those without ICP monitors.[27] All the patients were clinically and radiologically evaluated for raised ICP and taken for DC. In all cases, we have done F-T-P craniectomy. Dural augmentation was done by G-patch. We have done an additional interoptic cisternal puncture in some cases where brain pulsation was not found intraoperatively. It is found that approximately 42 (37.5%) cases underwent surgery within 48 hours of trauma. Only 18 (16.07%) patients underwent DC within 24 hours. Around 102 (91.07%) of patients underwent DC within 5 days of trauma. This delay in operation, in comparison to other studies,[6] is mostly due to delayed presentation of the patients to our hospital being referred from different peripheral hospitals and lack of good transport system.
Treating TBI by DC is to prevent secondary injury and the establishment of a vicious cycle. It also improves cerebral perfusion pressure and cerebral blood flow.[4] [28] However, post-DC is associated with several complications, which adversely affect the clinical outcome. Most of the complications develop from normal pathophysiologic changes in ICP, CSF circulation, and cerebral blood flow (CBF), due to the removal of a large portion of skull. In our study, the most common postoperative complication of DC was subdural hygroma and the majority of patients affected resolved spontaneously which concurs with other studies.[1] [29] [30] The subdural in two cases was drained by burr hole and evacuation in other cases after cranioplasty subsided.
However, in our study, intraoperative brain swelling was most common complication encountered during surgery. In one case of 78-year-old male patient with hemispheric ASDH with SAH and diffuse cerebral edema having GCS E2 V1 M2, it was a devastating experience that the brain swelling was so malignant that it was not possible to control brain bulge. Increase size of previously small contusion with development of intracranial hematoma after DC and rebleeding was found in nine patients (8.03%). This complication may occur because of a reduction or loss of the tamponade effect after decompression.[29] Due to rebleeding in three cases with enlargement of contusion, reoperation was done after postoperative diagnosis on CT. Therefore, early detection and appropriate management is the key. Nine of our patients (8.03%) developed postoperative epilepsy. The mechanism of postoperative epilepsy is still not fully understood but graded increases in hyperexcitability and a reduced epileptogenic threshold have been suggested to be potential causes of seizure.[31] In the present study, cerebral herniation and fungation occurred in eight patients (7.14%) although craniectomy of larger than 12 to 15 cm in diameter had been performed. This may be due to initial increase edema and raised ICP. However, surgical intervention, such as debridement of necrotic herniated brain was done in three patients, out of these, two died within few months of surgery. Postoperative wound infection was found in 10 (8.92%) patients who were managed by daily dressing and antibiotics. CSF leak postoperatively from wound site is found in three cases. One case of CSF leak from the wound site which did not subside even after conservative treatment of 7 days reopened on day 8. It was found to be no specific leak site but CSF were coming out as effusion from G-patch pores which was again closed only applying some blooded gel foam and closed. The patient was advised acetazolamide tablets and after another 10 days, it subsides completely. In our study, five patients (4.46%) developed postdecompressive sink brain with trephination syndrome and the symptoms were improved after early cranioplasty. Other studies also support early cranioplasty once syndrome is developed.[29] [30] Postcranioplasty wound infection with exposure of mesh was found in two cases. One case of exposed mesh with infected wound was debrided with extraction of mesh and after 2 months, he again repaired with titanium mesh. Early cranioplasty within 6 weeks of DC was done in only 28 cases. Others are done from 6 weeks to 6 months duration. It is found that no such significant difference revealed between these groups. However, in patients with complications such as trephination syndrome, hydrocephalus, contralateral subdural effusion, early cranioplasty resulted good outcome. In the present study, analysis showed patients without complications were more likely to achieve functional recovery (GOS 4–5) after surgery, but the patients with complications such as intraoperative brain swelling, fungation and brain bulge, rebleeding, and expansion of contusion show high mortality rate (p-value < 0.001) Therefore, it is important to prevent these complications and to detect them at the earliest opportunity after DC.
Among the nonsurgical complication, prehospitalization aspiration pneumonia and ventilator-associated pneumonia were the most common complication found in 14.28% of patients. Next to it was central venous (CV) line induced hemopneumothorax in 4.46%. Postoperative sepsis was found in 7.14% of patients. It is revealed that patients with these complications have longer hospital stay, morbidity, and mortality (p-value < 0.001).
Total number of deaths during the period of hospitalization in patient who underwent DC were 30 (26.78%) out of 112 cases, with male to female ratio of 7:3 (n = 21, n = 9). The death rate in patients who underwent DC is around just double of death rate of all TBI patients admitted. The percentage of death found more in the age groups of > 60 is 38.46%, next to it was 41 to 60 years, 28.94%; 0 to 18 years, 25%; and 19 to 40 years, 22.44%. It showed that more number of patients in the age group of more than 40 years, particularly in the age group of more than 60 years died after DC. The mortality rate is less in the age group of 19 to 40 years. Most of the deaths were occurred in patients presented with GCS score of less than 8. The most common causes in these cases were preoperative and postoperative aspiration pneumonia. Two cases in the age group of 41 to 60 years died due to associated chest injury and hemothorax. Two patients having multiple long bone fracture died after DC. About 18 patients with GCS score 3 or 4 with dilated unilateral or bilateral pupil underwent DC. Out of these, only five patients survived, with survivability after surgery was 27.77% and mortality rate of 72.23%. Intraoperative malignant brain swelling was cause of death in one patient. Postoperative detection of hemopneumothorax due to CV line was managed by chest tube but one patient detected late was died even after chest tube insertion, due to irreversible brain damage due to decreased lung compliance and sepsis.
Most of the patients in the age group of older than 40 years with comorbid factors and low GCS score spent more than 3 weeks of hospitalization. Postoperative CSF leaks, wound infection, and ventilator-associated pneumonia were the additional factors for more than 3 weeks of hospitalization.
The outcome was analyzed using GOS. The overall mortality in our study was (30/112) 26.78% and 28 (34.14%) patients discharged from hospital with severe neurological compromise. Fifty-four (48.21%) patients discharged with good neurological condition so as to perform their daily activity. After discharge it was found that with better home care, all the patient of mild disability group and 40% of severe neurologically compromised patients improved to mild disability state at 3 months follow-up. Two patients from vegetative state group, 17-year-old boy who underwent bilateral FTP decompression and 32-year-old man were improved and now able to take orally by some assistant. It is found that two patients of severe disability group in the age group of 19 to 40 years, having hemiparesis improved after cranioplasty and doing their normal duties. It is found that patients presented with GCS score < 8, associated SAH, intraoperative brain bulge, associated chest injury and long bone fracture, cerebral infraction, old age > 40 years, and alcoholics have poor prognosis as compared with others (p-value < 0.001).
In March 2011, investigators from Australia and several other countries published the results of the DECRA[5] trial (DC in patients with severe TBI) in the New England Journal of Medicine. This was a randomized trial comparing DC to best medical therapy run between 2002 and 2010 to assess the optimal management of patients with medically refractory ICP following diffuse nonpenetrating head injury. The study investigators found that DC was associated with worse functional outcomes, as measured by a standard metric, than best medical care. There were no differences in deaths between groups. However, the results of the DECRA trial have been rejected or at least questioned by many practicing neurosurgeons, and a concurrently published editorial raises several study weaknesses.[5] From our study, it is also found that DC improves patient outcome, produces positive results in severe TBI, and protects preventable deaths. A mortality rate of 26.78%, disability rate of 34.14%, and good life of 48.21% with survivable of 73.21% shows that DC yields good results.
Conclusion
DC yields good results in severe TBI. The mortality rate in patient undergoing DC for uncontrollable raised ICP is around twice of the overall mortality rate of total TBI. Also, patients presented with GCS score < 8, associated SAH, intraoperative brain bulge, associated chest injury and long bone fracture, cerebral infraction, old age >40 years, male sex, alcoholics, pupillary dilation at surgery, and aspiration pneumonia are the independent factors for increased mortality, disability, and long hospital stay. It can be suggested that DC should be little liberal to manage extensive parenchymal injury where the development of edema is expected even if the GCS score is more than 8. Waiting till incompatible raised ICP or deterioration from mild and moderate head injury to severe head injury by GCS, to undertake DC provides bad outcome. We fill that ICP monitoring is not mandatory in decision making for DC.
Disclosure
All authors have none to declare.
-
References
- 1 Chibbaro S, Tacconi L. Role of decompressive craniectomy in the management of severe head injury with refractory cerebral edema and intractable intracranial pressure. Our experience with 48 cases. Surg Neurol 2007; 68 (6) 632-638
- 2 Martins ET, Linhares MN, Sousa DS , et al. Mortality in severe traumatic brain injury: a multivariated analysis of 748 Brazilian patients from Florianópolis city. J Trauma 2009; 67 (1) 85-90
- 3 Hyder AA, Aggarwal A. The increasing burden of injuries in Eastern Europe and Eurasia: making the case for safety investments. Health Policy 2009; 89 (1) 1-13
- 4 Kunze E, Meixensberger J, Janka M, Sörensen N, Roosen K. Decompressive craniectomy in patients with uncontrollable intracranial hypertension. Acta Neurochir Suppl (Wien) 1998; 71 (Supplement): 16-18
- 5 Cooper DJ, Rosenfeld JV, Murray L , et al; DECRA Trial Investigators; Australian and New Zealand Intensive Care Society Clinical Trials Group. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 2011; 364 (16) 1493-1502
- 6 Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg 2006; 104 (4) 469-479
- 7 Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ. Surgical decompression for traumatic brain swelling: indications and results. J Neurosurg 1999; 90 (2) 187-196
- 8 Huang AP, Tu YK, Tsai YH , et al. Decompressive craniectomy as the primary surgical intervention for hemorrhagic contusion. J Neurotrauma 2008; 25 (11) 1347-1354
- 9 Kim KH. Predictors for functional recovery and mortality of surgically treated traumatic acute subdural hematomas in 256 patients. J Korean Neurosurg Soc 2009; 45 (3) 143-150
- 10 Hossain-Ibrahim MK, Tarnaris A, Wasserberg J. Decompressive craniectomy –friend or foe?. Trauma 2012; 14 (1) 16-38
- 11 Alvis-Miranda H, Castellar-Leones SM, Moscote-Salazar LR. Decompressive craniectomy and traumatic brain injury: a review. Bull Emerg Trauma 2013; 1 (2) 60-68
- 12 Nath PC, Mishra SS, Deo RC, Jena SP. Spectrum of pediatric head injury with management and outcome: a single tertiary care center study. Indian J Neurotrauma 2015; 12 (1) 10-18
- 13 Skoglund TS, Eriksson-Ritzén C, Jensen C, Rydenhag B. Aspects on decompressive craniectomy in patients with traumatic head injuries. J Neurotrauma 2006; 23 (10) 1502-1509
- 14 Sinha S, Raheja A, Garg M , et al. Decompressive craniectomy in traumatic brain injury: a single-center, multivariate analysis of 1,236 patients at a tertiary care hospital in India. Neurol India 2015; 63 (2) 175-183
- 15 Qiu W, Guo C, Shen H , et al. Effects of unilateral decompressive craniectomy on patients with unilateral acute post-traumatic brain swelling after severe traumatic brain injury. Crit Care 2009; 13 (6) R185
- 16 Haddad SH, Arabi YM. Critical care management of severe traumatic brain injury in adults. Scand J Trauma Resusc Emerg Med 2012; 20: 12
- 17 Saul TG, Ducker TB. Effect of intracranial pressure monitoring and aggressive treatment on mortality in severe head injury. J Neurosurg 1982; 56 (4) 498-503
- 18 Saul TG, Ducker TB. Intracranial pressure monitoring in patients with severe head injury. Am Surg 1982; 48 (9) 477-480
- 19 Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD. High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg 1988; 69 (1) 15-23
- 20 Howells T, Elf K, Jones PA , et al. Pressure reactivity as a guide in the treatment of cerebral perfusion pressure in patients with brain trauma. J Neurosurg 2005; 102 (2) 311-317
- 21 Bulger EM, Nathens AB, Rivara FP, Moore M, MacKenzie EJ, Jurkovich GJ ; Brain Trauma Foundation. Management of severe head injury: institutional variations in care and effect on outcome. Crit Care Med 2002; 30 (8) 1870-1876
- 22 Mauritz W, Steltzer H, Bauer P, Dolanski-Aghamanoukjan L, Metnitz P. Monitoring of intracranial pressure in patients with severe traumatic brain injury: an Austrian prospective multicenter study. Intensive Care Med 2008; 34 (7) 1208-1215
- 23 Stocchetti N, Penny KI, Dearden M , et al; European Brain Injury Consortium. Intensive care management of head-injured patients in Europe: a survey from the European brain injury consortium. Intensive Care Med 2001; 27 (2) 400-406
- 24 Cremer OL, van Dijk GW, van Wensen E , et al. Effect of intracranial pressure monitoring and targeted intensive care on functional outcome after severe head injury. Crit Care Med 2005; 33 (10) 2207-2213
- 25 Cremer OL. Does ICP monitoring make a difference in neurocritical care?. Eur J Anaesthesiol Suppl 2008; 42 (Suppl. 42) 87-93
- 26 Shafi S, Diaz-Arrastia R, Madden C, Gentilello L. Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma 2008; 64 (2) 335-340
- 27 Alkhoury F, Kyriakides TC. Intracranial pressure monitoring in children with severe traumatic brain injury: National Trauma Data Bank-based review of outcomes. JAMA Surg 2014; 149 (6) 544-548
- 28 Schneider GH, Bardt T, Lanksch WR, Unterberg A. Decompressive craniectomy following traumatic brain injury: ICP, CPP and neurological outcome. Acta Neurochir Suppl (Wien) 2002; 81 (Supplement): 77-79
- 29 Yang XF, Wen L, Shen F , et al. Surgical complications secondary to decompressive craniectomy in patients with a head injury: a series of 108 consecutive cases. Acta Neurochir (Wien) 2008; 150 (12) 1241-1247 , discussion 1248
- 30 Yang XJ, Hong GL, Su SB, Yang SY. Complications induced by decompressive craniectomies after traumatic brain injury. Chin J Traumatol 2003; 6 (2) 99-103
- 31 Chen JW, Ruff RL, Eavey R, Wasterlain CG. Posttraumatic epilepsy and treatment. J Rehabil Res Dev 2009; 46 (6) 685-696
Address for correspondence
-
References
- 1 Chibbaro S, Tacconi L. Role of decompressive craniectomy in the management of severe head injury with refractory cerebral edema and intractable intracranial pressure. Our experience with 48 cases. Surg Neurol 2007; 68 (6) 632-638
- 2 Martins ET, Linhares MN, Sousa DS , et al. Mortality in severe traumatic brain injury: a multivariated analysis of 748 Brazilian patients from Florianópolis city. J Trauma 2009; 67 (1) 85-90
- 3 Hyder AA, Aggarwal A. The increasing burden of injuries in Eastern Europe and Eurasia: making the case for safety investments. Health Policy 2009; 89 (1) 1-13
- 4 Kunze E, Meixensberger J, Janka M, Sörensen N, Roosen K. Decompressive craniectomy in patients with uncontrollable intracranial hypertension. Acta Neurochir Suppl (Wien) 1998; 71 (Supplement): 16-18
- 5 Cooper DJ, Rosenfeld JV, Murray L , et al; DECRA Trial Investigators; Australian and New Zealand Intensive Care Society Clinical Trials Group. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 2011; 364 (16) 1493-1502
- 6 Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg 2006; 104 (4) 469-479
- 7 Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ. Surgical decompression for traumatic brain swelling: indications and results. J Neurosurg 1999; 90 (2) 187-196
- 8 Huang AP, Tu YK, Tsai YH , et al. Decompressive craniectomy as the primary surgical intervention for hemorrhagic contusion. J Neurotrauma 2008; 25 (11) 1347-1354
- 9 Kim KH. Predictors for functional recovery and mortality of surgically treated traumatic acute subdural hematomas in 256 patients. J Korean Neurosurg Soc 2009; 45 (3) 143-150
- 10 Hossain-Ibrahim MK, Tarnaris A, Wasserberg J. Decompressive craniectomy –friend or foe?. Trauma 2012; 14 (1) 16-38
- 11 Alvis-Miranda H, Castellar-Leones SM, Moscote-Salazar LR. Decompressive craniectomy and traumatic brain injury: a review. Bull Emerg Trauma 2013; 1 (2) 60-68
- 12 Nath PC, Mishra SS, Deo RC, Jena SP. Spectrum of pediatric head injury with management and outcome: a single tertiary care center study. Indian J Neurotrauma 2015; 12 (1) 10-18
- 13 Skoglund TS, Eriksson-Ritzén C, Jensen C, Rydenhag B. Aspects on decompressive craniectomy in patients with traumatic head injuries. J Neurotrauma 2006; 23 (10) 1502-1509
- 14 Sinha S, Raheja A, Garg M , et al. Decompressive craniectomy in traumatic brain injury: a single-center, multivariate analysis of 1,236 patients at a tertiary care hospital in India. Neurol India 2015; 63 (2) 175-183
- 15 Qiu W, Guo C, Shen H , et al. Effects of unilateral decompressive craniectomy on patients with unilateral acute post-traumatic brain swelling after severe traumatic brain injury. Crit Care 2009; 13 (6) R185
- 16 Haddad SH, Arabi YM. Critical care management of severe traumatic brain injury in adults. Scand J Trauma Resusc Emerg Med 2012; 20: 12
- 17 Saul TG, Ducker TB. Effect of intracranial pressure monitoring and aggressive treatment on mortality in severe head injury. J Neurosurg 1982; 56 (4) 498-503
- 18 Saul TG, Ducker TB. Intracranial pressure monitoring in patients with severe head injury. Am Surg 1982; 48 (9) 477-480
- 19 Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD. High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg 1988; 69 (1) 15-23
- 20 Howells T, Elf K, Jones PA , et al. Pressure reactivity as a guide in the treatment of cerebral perfusion pressure in patients with brain trauma. J Neurosurg 2005; 102 (2) 311-317
- 21 Bulger EM, Nathens AB, Rivara FP, Moore M, MacKenzie EJ, Jurkovich GJ ; Brain Trauma Foundation. Management of severe head injury: institutional variations in care and effect on outcome. Crit Care Med 2002; 30 (8) 1870-1876
- 22 Mauritz W, Steltzer H, Bauer P, Dolanski-Aghamanoukjan L, Metnitz P. Monitoring of intracranial pressure in patients with severe traumatic brain injury: an Austrian prospective multicenter study. Intensive Care Med 2008; 34 (7) 1208-1215
- 23 Stocchetti N, Penny KI, Dearden M , et al; European Brain Injury Consortium. Intensive care management of head-injured patients in Europe: a survey from the European brain injury consortium. Intensive Care Med 2001; 27 (2) 400-406
- 24 Cremer OL, van Dijk GW, van Wensen E , et al. Effect of intracranial pressure monitoring and targeted intensive care on functional outcome after severe head injury. Crit Care Med 2005; 33 (10) 2207-2213
- 25 Cremer OL. Does ICP monitoring make a difference in neurocritical care?. Eur J Anaesthesiol Suppl 2008; 42 (Suppl. 42) 87-93
- 26 Shafi S, Diaz-Arrastia R, Madden C, Gentilello L. Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma 2008; 64 (2) 335-340
- 27 Alkhoury F, Kyriakides TC. Intracranial pressure monitoring in children with severe traumatic brain injury: National Trauma Data Bank-based review of outcomes. JAMA Surg 2014; 149 (6) 544-548
- 28 Schneider GH, Bardt T, Lanksch WR, Unterberg A. Decompressive craniectomy following traumatic brain injury: ICP, CPP and neurological outcome. Acta Neurochir Suppl (Wien) 2002; 81 (Supplement): 77-79
- 29 Yang XF, Wen L, Shen F , et al. Surgical complications secondary to decompressive craniectomy in patients with a head injury: a series of 108 consecutive cases. Acta Neurochir (Wien) 2008; 150 (12) 1241-1247 , discussion 1248
- 30 Yang XJ, Hong GL, Su SB, Yang SY. Complications induced by decompressive craniectomies after traumatic brain injury. Chin J Traumatol 2003; 6 (2) 99-103
- 31 Chen JW, Ruff RL, Eavey R, Wasterlain CG. Posttraumatic epilepsy and treatment. J Rehabil Res Dev 2009; 46 (6) 685-696