Keywords
vertebral spine - intervertebral disc dislocation - outcome evaluation (healthcare) - endoscopy
Introduction
The standard treatment for symptomatic lumbar disc herniation without instability is microdiscectomy decompression (MDL).[1] Other less aggressive techniques have been developed, such as percutaneous endoscopic lumbar discectomy (DEPL), which shows sufficient evidence of similar medium- and long-term safety and effectiveness when compared to MDL.[2]
[3]
[4] There is no consensus or definitive scientific evidence regarding the superiority of this technique over MDL. When comparing medium- and long-term (6 months and more than 2 years), primary outcomes (pain improvement, complication incidence, and functional outcomes) some studies show similar results,[5]
[6] whereas others demonstrate DEPL superiority over MDL in both primary[7]
[8]
[9] and secondary outcomes (surgical time, length of stay and bleeding volume).[10]
[11] Supported by studies with earlier initial assessment,[12]
[13] we have designed a patient evaluation protocol that starts much earlier than most studies on DEPL, beginning 48 hours after surgery, while the first assessment usually takes place within 4 to 6 weeks. Since the technique's medium- and long-term safety and effectiveness are proven,[14]
[15]
[16]
[17]
[18] we want to verify when clinical improvement actually begins, which may be a determining factor in choosing between surgical techniques with similar results.
Materials and Methods
We retrospectively evaluated prospectively collected data from 32 consecutive patients undergoing DEPL. All patients had single lumbar disc hernia, with symptoms for more than 3 months, accompanied by radiculopathy or not, and failed conservative treatment. All patients underwent elective surgeries, either interlaminar or transforaminal (in cases with foraminal disc disease), performed at private or accredited clinics and hospitals in São Paulo, SP, Brazil, between 2014 and 2017. Patients received postoperative analgesia, consisting in nimesulide 100 mg, every 12 hours for 7 days, dipyrone 1 g, every 8 hours for 10 days, and tramadol hydrochloride 50 mg up to every 8 hours, as required.
Patients with spondylolisthesis, previous lumbar surgeries, and spinal stenosis were excluded.
In addition to the time of hospital discharge, the visual analog scale (VAS, for both axial and irradiated pain), Oswestry disability index (ODI) and Roland-Morris questionnaire scores were recorded preoperatively, at 2 days, and at 1, 2, 4, 6, and 12 weeks postoperatively.
This research was approved by the ethics committee of the institution under number CAAE 90766918.8.0000.5449.
Results
The study included 21 men and 11 women (N = 32) aged between 22 and 71 years (mean age, 39.8 years). The average scores at each questionnaire are shown in [Figures 1], [2], and [3] and [Table 1].
 Fig. 1 Visual analog scale.
Fig. 1 Visual analog scale.
 Fig. 2 Oswestry questionnaire.
Fig. 2 Oswestry questionnaire.
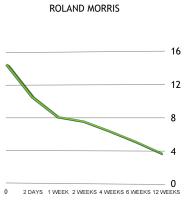 Fig. 3 Roland-Morris questionnaire.
Fig. 3 Roland-Morris questionnaire.
Table 1
|
VAS for axial pain
|
VAS for irradiated pain
|
Oswestry
|
Roland-Morris
|
|
0
|
6.63
|
6.66
|
44.59
|
14.03
|
|
2 DAYS
|
3.31
|
2.75
|
33.17
|
10.34
|
|
1 WEEK
|
2.84
|
2.84
|
30.22
|
8.06
|
|
2 WEEKS
|
2.38
|
2.63
|
28.38
|
7.56
|
|
4 WEEKS
|
2.31
|
2.19
|
25.31
|
6.47
|
|
6 WEEKS
|
2.28
|
2
|
19.39
|
5.28
|
|
12 WEEKS
|
1.94
|
1.78
|
14.31
|
3.97
|
The mean results showed a statistically significant reduction in scores between preoperative values and those obtained 2 days after surgery; the VAS for axial pain went from 6.63 to 3.31; the VAS for irradiated pain went from 6.66 to 2.75; the Oswestry scorewent from 44.59 to 33.17%, and the Roland-Morris score went from 14.03 to 10.34. This difference progressively improved up to 12 weeks postoperatively. Regarding the Oswestry score, minimum disability values (19.39%) were observed at 6 weeks.
In the comparison between average results obtained at 2 days and 12 weeks after surgery, there was a statistically significant reduction in the VAS for axial pain, which went from 3.31 to 1.94; in the Oswestry score, which went from 33.17 to 14.31%, and in the Roland-Morris score, which went from 10.34. to 3.97; the reduction of VAS for irradiated pain from 2.75 to 1.78, however, showed no statistical difference.
All patients were discharged within 6 hours. There was no readmission or supplementary surgery. Two patients (6.45%) presented de novo disc herniation without neurological deficit; both decided on conservative treatment, with progressive improvement.
There were no cases of significant bleeding, dural injury, or motor neurological deficit. There was one case (3.13%) of orthostatic headache with no dural lesion identified at the procedure, with resolution at 6 weeks, without fistula formation or cerebrospinal fluid collection. In addition, there was one case (3.13%) of dysesthesia at the operated dermatome, with resolution in 3 weeks with medication and physical therapy.
Statistical analysis was performed at Minitab 18.1 (Minitab, Inc, State College, PA, USA), with analysis of variance in a generalized linear model and Tukey paired comparisons for time variables. Grouping was performed using the Tukey method and a 95% confidence interval.
Discussion
Among the minimally invasive spinal surgeries, DEPL has advantages, including the possibility of performing it under local anesthesia, paraspinal structures preservation, and minimal postoperative pain.[19] Although these characteristics favor early discharge and faster recovery, previous studies began their evaluations only 4 or 6 weeks after surgery, losing the chance to assess whether there is an earlier improvement of the symptoms, one of the real benefits of this method.[14]
[15]
[16]
[17]
[18]
The improvement observed in the present study, when preoperative pain and functional questionnaires scores were compared with those obtained 12 weeks after surgery, is compatible with that of other published series.[19]
[20] Choi et al[4] showed parameters improvement starting at the 1st month. However, the confirmation of a significant reduction in pain and functional questionnaires scores beginning at 2 days after surgery is unprecedented, thus demonstrating an even earlier symptom improvement with DEPL.
In a literature review, Birkenmaier et al[11] only considered the last functional evaluation, with 2 or more years of follow-up. Other authors[17] do not specify when questionnaires were applied. Therefore, despite the existence of studies demonstrating the superiority of DEPL over MDL due to lesser tissue injury,[7] expressive pain relief and reduced complication incidence,[8] reduced surgical time and better disc height preservation,[18]
[21] we still do not know for sure when pain improves and the required length of stay, since published results are conflicting. This work intends to confirm that DEPL-induced improvement is earlier than usually reported.
The earliest improvement was observed in pain-related questionnaires, followed by functional questionnaires; this may be the result of a postoperative fear, from both patients and physicians, in resuming usual activities due to the risk of a de novo disc herniation.
Hospital discharge in less than 6 hours for 100% of the cases is consistent with the description of DEPL as an outpatient surgery. Most studies describe early discharges but fail to quantify its exact timing. In 2009, Lee et al[19] described a series of 25 patients who underwent DELP with a mean length of stay of 0.9 day; however, other series reported later discharges.[22] The literature shows recurrence rates ranging from 0 to 11.1%,[23] with up to 20.9% of reoperation rate;[4] our results are consistent with such findings, with a recurrence rate of 6.45%, and a reoperation rate of 0%.
Conclusion
All 32 patients from this series were discharged within 6 hours of the end of the procedure. Patients present significant improvement of painful and functional symptoms starting at 48 hours postoperatively. Pain and functional scores continued to improve up to 12 weeks after surgery. In this series, functional and pain scores improved earlier than described in the literature for patients undergoing DEPL.





