Keywords
meningioma - chordoid - brain neoplasms - pathology
Palavras-chave
meningioma - cordóide - tumor cerebral - patologia
Introduction
Chordoid meningioma (CM) is a rare variant of meningioma that bears a striking histological
resemblance to chordoma and has a greater likelihood of recurrence. The differential
diagnosis includes chordomas, myxoid chondrosarcoma and chordoid glioma.[1] In the present study, we report a case of a female patient with a diagnosis of a
recent onset of headache and visual cloudiness. Meningiomas represent almost 30% of
primary intracranial neoplasms.
Chordoid meningioma is a rare subtype of meningioma, accounting to 0.5% of all meningiomas
and associated with different behavior.[2]
Chordoid meningiomas are classified in Grade II by the World Health Organization (WHO).[3] Chordoid meningioma has a similar distribution between men and women. Chordoid meningioma
can have a large distribution in the age range, and may range from 4 to 77 years old.[4] A little more than 100 cases of chordoid meningioma have been described in the English
language literature, the majority of which are in the pathology and neurosurgery literature.
Material and Methods
Case Report
Female, 42-year-old, with complaints of sudden onset of headache and visual impairment.
Upon neurological examination, the patient presented paresis of the left medial rectus
muscle. The neurosurgery team requested a magnetic resonance imaging (MRI) exam, which
showed an expansive lesion in the left frontotemporal topography. The lesion was causing
an important compression of the medial rectus muscle ([Fig. 1]). We opted for a left frontotemporal craniotomy, since it was possible to resect
the lesion. The patient progressed well during surgery and, after the postoperative
period, was discharged from the hospital feeling well and with no neurological deficits.
([Fig. 2])
 Fig. 1 Magnetic Resonance Imaging (MRI): Axial FLAIR showed an expansive lesion in the left
frontotemporal topography. The lesion presented with important compression of the
medial rectus muscle.
Fig. 1 Magnetic Resonance Imaging (MRI): Axial FLAIR showed an expansive lesion in the left
frontotemporal topography. The lesion presented with important compression of the
medial rectus muscle.
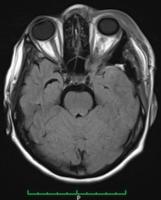 Fig. 2 Magnetic Resonance Imaging: Axial FLAIR - Evidence of satisfactory resection of the
lesion.
Fig. 2 Magnetic Resonance Imaging: Axial FLAIR - Evidence of satisfactory resection of the
lesion.
We sent the material for pathological analysis, which revealed mesenchymal neoplasia
with chordoid pattern in the left temporal frontographic topography ([Figs. 1] and [2]). Therefore, the diagnosis was of chordoid meningioma. The immunohistochemistry
analysis was positive for epithelial membrane antigen, therefore being typical of
the chordoid meningioma ([Figs. 3] and [4]). The literature review involved clinical case reports, randomized controlled trials
and a series of cases describing clinical and epidemiological treatments for chordoid
meningioma. The search was performed using the PubMed database and targeting all English
language publications available involving chordoid meningioma. This review was organized
applying the MeSH terms chordoid meningioma, meningioma and chordoid. The search about chordoid meningioma at PubMed/Medline retrieved 83 articles. For
all these articles, we applied filters such as species (humans) and age (19 to 65
years old). Then, we retrieved 59 papers. Analyzing the titles of the articles, 59
were selected for summary review, considering relevance and relation to the present
paper. Among those 59, 31 were selected and examined.
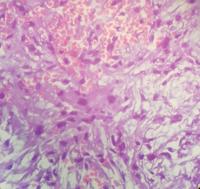 Fig. 3 Histology: Neoplastic cells in cordonal arrangement in the middle of an abundant
mucoid matrix. Cells may be vacuolated, increasing the resemblance to the bullous
appearance of chordoma cells.
Fig. 3 Histology: Neoplastic cells in cordonal arrangement in the middle of an abundant
mucoid matrix. Cells may be vacuolated, increasing the resemblance to the bullous
appearance of chordoma cells.
 Fig. 4 Immunohistochemistry: Membrane epithelial antigen marks neoplastic cells. The interstitial
material appears pale. Here it marks the cytoplasm of the neoplastic cells, with reinforcement
at the cellular membrane level in areas.
Fig. 4 Immunohistochemistry: Membrane epithelial antigen marks neoplastic cells. The interstitial
material appears pale. Here it marks the cytoplasm of the neoplastic cells, with reinforcement
at the cellular membrane level in areas.
Results
Meningiomas have preponderance for convexities. For instance, 17 to 25% occur in a
frontobasal location. Within the frontobasal region, the olfactory grooves, the tuberculum
sellae, the parasellar region and the petrous bone are preferred sites.[5] On the other hand, 5% occur along the cerebellar convexity, 2 to 4% at the tentorium
cerebelli, and 2 to 4% within the cerebellopontine angle (CPA).[6]
Chordoid meningioma is an uncommon histopathological variant of meningioma frequently
mistaken as chordoma, due to its histological similarity. Couce et al related 42 clinicopathologic
studies about CM during the period of 1975 to 1997, and this study concluded that
it was more common in the supratentorial region and in adults.[6]
[7]
There are only two studies about genetic alterations in CMs. The majority of meningiomas
is known to have deletion at many chromosomal loci not yet studied in CMs, such as
22q, 18p, 14q and 1p. All of the literature cases showed to have either complete or
partial deletion at 22q, 14q and 1p loci.[8]
[9] Additionally, all cases were variably positive for epithelial membrane antigen (EMA)
and showed strong positive staining for vimentin, but were completely negative for
glial fibrillary acidic protein (GFAP), in support of the diagnosis.[9] Because of the similarity between CMs and other lesions, especially tumors, careful
assessment of each case is required. The main diagnoses are chondroid choroid, chordoid
glioma, paraganglioma, metastatic mucinous carcinoma or metastatic renal cell carcinoma,
among others.[10]
The goal of the therapy in CM is relieving the compression of critical anatomic structures
as well as preventing tumor spread and recurrence.[11] The therapeutic preference for aggressive meningiomas are surgical resection, radiotherapy
(RT) and chemotherapy, in cases of anaplastic meningioma.[10]
[11] Neurosurgery is the treatment of choice for meningiomas and, preferentially, with
total resection.[10]
Discussion
Meningiomas are the second most common central nervous system neoplasm in adults and
account for 15 to 20% of all primary brain tumors. Meningiomas are benign tumors;
however 10% of the cases demonstrate a more aggressive clinical behavior, such as
chordoid meningioma, which is a type of non-benign meningioma.[12] First described by Kepes in 1988, chordoid meningiomas are characterized by cords
of eosinophilic, epithelial or spindle-shaped cells within a myxoid stroma, resembling
chordoma. Variable numbers of lymphocytes and plasma cells characterize these tumors.
Chordoid meningiomas occur very rarely, corresponding to up to 1% of surgically removed
meningiomas, even in large cohorts. Chordoid meningiomas are located supratentorially
in 81.5% of the cases.[13] Unusual sites, such as the ventricular system, the foramen jugulare and the orbital
area have been described in several case reports.[14]
[15] Histologically, CM consists of cords or trabeculae of eosinophilic and vacuolated
cells embedded in an abundant mucoid matrix.[16]
However, sometimes the histological diagnosis is difficult because it is comparable
morphology in other intracranial tumors, such as chordoid glioma, chordoma, extraskeletal
chondrosarcoma, myxopapillary ependymoma and metastatic tumors.[8]
Immunohistopathological studies have shown that this tumor shows positivity for vimentin,
EMA and D2–40, and occasional positivity for S-100 protein, on the other hand demonstrating
negativity for GFAP and cytokeratin.[9]
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
The first choice of treatment for CM is surgical excision. The goal of surgery is
a complete resection. The complete resection of a tumor is sometimes difficult because
of its location.[8]
[9]
[10]
[11] The surgical strategy is to perform total resection of the tumor, dura and bone,
while protecting the surrounding structures. In contrast, when an incomplete removal
is realized, due to the risk of injury to the surrounding vital neurovascular structures,
postoperative adjuvant RT is an acceptable option.[16]
[19]
[20] Despite this recommendation, there is controversy surrounding the value of postoperative
RT in atypical meningiomas. This treatment is commonly recommended for patients with
atypical meningiomas following subtotal removal, but some investigators, acknowledging
the greater recurrence risk of atypical meningiomas, recommend early irradiation,
irrespective of the resection extent, to optimize local control and improve survival.[5] Once recurrent, grade II meningiomas carry a mortality risk and postoperative RT,
after total removal, may prolong or prevent recurrence.[9] Perhaps, more comprehensive series are required to evaluate the role of brain invasion
and postoperative RT in the prognosis of CM.[1]
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
[20]
[21] In our case, we reconvened the patient to continue the treatment and improve the
prognosis.
Conclusion
Chordoid meningiomas are rare and different tumors of the meningiomas that present
a high degree of recurrence, even when the satisfactory resection of the lesion is
achieved. Recurrence is particularly worrisome after a subtotal surgical resection.
Their histological similarity to chordoid neoplasms, especially chordoma, can make
the diagnosis challenging. These two neoplasms have different biological behaviors,
so it is important to be able to distinguish them. The goal of treatment is surgery,
with total resection of the tumor. In cases of relapse or in cases of residual tumor,
it is necessary to perform RT.






