
RSS-Feed abonnieren
DOI: 10.1055/s-0041-1724044
Anastomosis Patterns between the Median and Ulnar Nerves in the Upper Limbs
Padrões de anastomose entre os nervos mediano e ulnar nos membros superiores

- Abstract
- Resumo
- Introduction
- Martin-Gruber Anastomosis
- Marinacci Anastomosis
- Berrettini Anastomosis
- Riche-Cannue Anastomosis
- Conclusion
- References
Abstract
There are four types of anastomoses between the median and ulnar nerves in the upper limbs. It consists of crossings of axons that produce changes in the innervation of the upper limbs, mainly in the intrinsic muscles of the hand. The forearm has two anatomical changes – Martin-Gruber: branch originating close to the median nerve joining distally to the ulnar nerve; and Marinacci: branch originating close to the ulnar nerve and distally joining the median nerve. The hand also has two types of anastomoses, which are more common, and sometimes considered a normal anatomical pattern – Berrettini: Connection between the common digital nerves of the ulnar and median nerves; and Riche-Cannieu: anastomosis between the recurrent branch of the median nerve and the deep branch of the ulnar nerve. Due to these connection patterns, musculoskeletal disorders and neuropathies can be misinterpreted, and nerve injuries during surgery may occur, without the knowledge of these anastomoses. Therefore, knowledge of them is essential for the clinical practice. The purpose of the present review is to provide important information about each type of anastomosis of the median and ulnar nerves in the forearm and hand.
#
Resumo
Existem quatro tipos de anastomoses entre os nervos mediano e ulnar nos membros superiores. Elas consistem em cruzamentos de axônios que produzem mudanças na inervação dos membros superiores, principalmente na musculatura intrínseca da mão. O antebraço apresenta duas variações anatômicas – Martin-Gruber: ramo que se origina proximalmente ao nervo mediano e se une distalmente ao nervo ulnar; e Marinacci: ramo que se origina proximalmente ao nervo ulnar e se une distalmente ao nervo mediano. A mão apresenta também dois tipos de anastomoses, mais comuns, por vezes considerados padrão anatômico normal – Berrettini: conexão entre os nervos digitais comuns dos nervos ulnar e mediano; e Riche-Cannieu: anastomose entre o ramo recorrente do nervo mediano e o ramo profundo do nervo ulnar. Devido a esses padrões de conexões, distúrbios musculoesqueléticos e neuropatias podem ser mal interpretadas, e lesões nervosas durante as cirurgias podem ocorrer, sem o conhecimento dessas anastomoses. Portanto, o conhecimento delas é fundamental para a prática clínica. O objetivo desta revisão é fornecer informações importantes acerca de cada tipo de anastomose dos nervos mediano e ulnar no antebraço e na mão.
#
Keywords
Martin Gruber - Marinacci - Berrettini - Riche-Cannieu - median nerve - ulnar nerve - anastomosisPalavras-chave
Martin-Gruber - Marinacci - Berrettini - Riche-Cannieu - nervo mediano - nervo ulnar - anastomosesIntroduction
Anastomoses between the median and ulnar nerves can be found in the upper limbs. They consist of crossings of axons that can produce variations in the innervation of the muscles in the upper limbs, mainly the motor part of the intrinsic muscles of the hand.[1] [2] Basically, four types of anastomoses can be found between the median and ulnar nerves in the upper limbs: two connections in the forearm (Martin-Gruber and Marinacci) and two connections in the hand (Berrettini and Riche-Cannieu).
The median nerve originates from the roots of C5 to T1 of the brachial plexus. It does not innervate any muscle in the arm. In the forearm, it is responsible for the innervation of the flexor and pronator muscles, except for the flexor carpi ulnaris muscle and half of the flexor digitorum profundus III and IV, which are innervated by the ulnar nerve. In the hand, the median nerve innervates lumbrical muscles I and II, the opponens pollicis muscle, the abductor pollicis brevis muscle, and the flexor pollicis brevis muscle. In the elbow, the median nerve branches into the anterior interosseous nerve, which is a purely motor nerve that innervates the flexor digitorum I and II, the flexor pollicis longus, and the pronator quadratus muscle.[3]
The ulnar nerve originates from the roots of C8 and T1. It also does not innervate any muscle in the arm. As previously reported,[3] in the forearm region, it innervates the flexor ulnaris carpi muscles and half of the flexor digitorum profundus III and IV. In the hand, it innervates the adductor pollicis, interosseous muscles, lumbrical muscles III and IV, the hypotenary musculature, the palmaris brevis muscle and the deep part of the flexor pollicis brevis muscle.
The knowledge of the different patterns of anastomoses between the median and ulnar nerves in the forearm and hand is important to recognize the clinical manifestations in peripheral nerves and musculoskeletal disorders, as well as to plan surgical approaches and understand their prognosis.[4] [5] [6] [7]
#
Martin-Gruber Anastomosis
The anastomosis in the forearm, in which the anastomotic branch originates proximally to the median nerve and joins distally to the ulnar nerve, is known as the median-ulnar anastomosis, or Martin-Gruber anastomosis ([Figs. 1] [2] [3]).


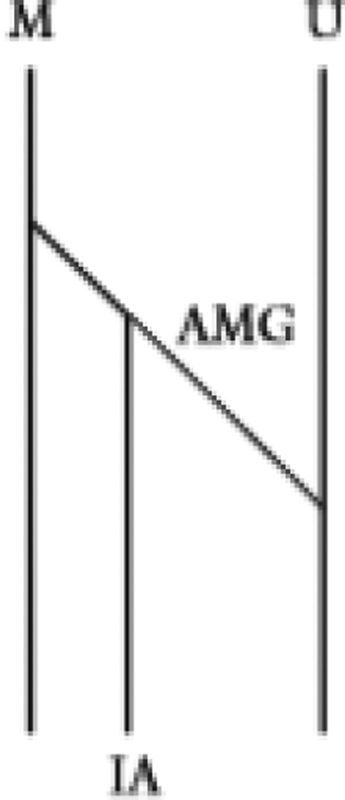
In 1763, Martin,[8] a Swedish anatomist, was the first to consider the possibility of a connection between the fascicles of the median and ulnar nerves in the forearm. In the following century, in 1870, Gruber[9] dissected 250 forearms and found 38 connections (15.2%); since then, the median-ulnar anastomosis became known as the Martin-Gruber anastomosis.
This anastomosis can occur between the branches intended for the flexor digitorum profundus, directly from the median nerve to the ulnar nerve, between the anterior interosseous nerve and the ulnar nerve, or by combinations between these types of anastomoses.[10]
The reported incidence of the Martin-Gruber anastomosis in the literature ranges from 10.5% to 23%.[1] [9] [11] [12] [13] In a meta-analysis of 41 studies conducted by Roy et al.,[14] the prevalence found was of 19.5%.
The Martin-Gruber anastomosis can be divided into six subtypes – type I: oblique anastomotic branch between the anterior interosseous nerve and the ulnar nerve; type II: double anastomosis between the anterior interosseous nerve and the ulnar nerve; type III: anastomosis between the median nerve and the ulnar nerve; type IV: anastomosis between the branches of the median and ulnar nerves that follow to the flexor digitorum profundus muscle; type V: intramuscular anastomosis; and type VI: anastomosis between the median nerve branch that leads to the flexor digitorum superficialis muscle and the ulnar nerve.[15]
In about 56.5% of the Martin-Gruber anastomoses discovered, the proximal anastomotic branch originates from the anterior interosseous nerve.[9] Taams[13] suggested that the Martin-Gruber anastomosis occurs more frequently in the right forearm than in the left forearm, and is only bilateral in 10% to 40% of the cases. Gruber[9] further suggested that it would be more common to find only one anastomotic branch than two.
The Martin-Gruber anastomosis is observed mainly in the upper portion of the forearm, in the plane between the epitrochlear muscles and the flexor digitorum profundus muscle.[16] [17] Srinivasan and Rhodes[18] congenitally examined abnormal fetuses (fetuses with trisomy 21) and found the Martin-Gruber anastomosis on both forearms of every fetus. Crutchfield and Gutmann[19] and Piza-Katzer[20] found a communication between the median nerve and the ulnar nerve in family members of people who showed this anomalous connection, and suggested that it is a hereditary trait, probably autosomal dominant.
The recognition of the Martin-Gruber anastomosis is important for the correct diagnosis of neuropathies, and traumatic and compressive injuries of the peripheral nerves. For example, a patient may have compression of the median nerve in the wrist through the flexor retinaculum of the hand (carpal tunnel syndrome) with preservation of the clinical symptoms and atypical electromyographic findings in the tenar musculature, or, inversely, they may have symptoms of carpal tunnel syndrome without compression of the median nerve observed by the negative Tinel and Phalen tests, due to compression of the ulnar nerve in the elbow.[21]
Brandsma et al.[22] described the cases of five patients with complete lesion to the ulnar nerve in the elbow and injury to the median nerve in the wrist, due to leprosy neuropathy, who mainteined good function of the first dorsal interosseous muscle and flexor pollicis brevis muscle. He attributed these findings to the presence of the Martin-Gruber anastomosis, which was later confirmed by studies of nerve conduction, reinforcing its clinical importance.
#
Marinacci Anastomosis
Another type of anastomosis can occur between the median nerve and the ulnar nerve in the forearm. The anastomotic branch originates proximally to the ulnar nerve and joins distally to the median nerve, and it is called an ulnar-median anastomosis, reverse Martin-Gruber anastomosis, or Marinacci anastomosis. It is composed mainly of motor fibers.[23] ([Figs. 4] [5] [6]).



In 1964, Marinacci[24] reported the case of a patient who suffered trauma to the median nerve in the forearm, but preserved the muscles of the hand innervated by the median nerve, despite denervation of the flexors muscles of the forearm. The reported frequency of Marinacci anastomosis is very low. In many studies[29], this type of anastomosis was not found, and it is considered by many authors an anatomical anomaly.
The occurrence of Martin-Gruber or Marinacci anastomoses can be understood by the fact that the median and ulnar nerves develop from a similar embryonic region.[25] There are reports of a high incidence of peripheral-nerve connections in monkeys, which indicates a phylogenetic basis.[1] [26]
Regarding the Marinacci anastomosis, there are no studies on the incidence in cadavers, but its incidence in electroneuromyography studies was of 5% according to Rosen[27] and of 16.7% according to Golovchinsky[28]. Felippe et. al[29] demontrated a dissection cadaver that presented a rare case of Marinacci anastomosis: the anastomotic branch originated proximally to the ulnar nerve, and was inserted into the anterior interosseous nerve, located on the right side; it was a single anastomotic branch measuring 7.4 cm in length.[27] [28] [29]
Sraj et al.[30] published a case report of a patient who, despite presenting typical symptoms of carpal tunnel syndrome, did not manifest any of the clinical signs of median nerve compression. The patient presented evidence of compression of the ulnar nerve in the elbow, and by testing the ulnar nerve, the authors found that the patient had the symptoms of carpal tunnel syndrome. Another case reported by Sraj et al have also reported a patient with a median nerve injury to the elbow[30], without clinical repercussion in the thenar muscles, such as the abdutor pollicis brevis muscle, innervated by the median nerve. No changes were observed in the hand muscles, despite the denervation of the flexor muscles of the forearm.[29]
#
Berrettini Anastomosis
Communications between the median nerve and the ulnar nerve can occur with great frequency in the wrist and hand, and the anastomosis between the deep branch of the ulnar nerve and the recurrent branch of the median nerve in the tenar eminence is known as the Riche-Cannieu anastomosis. Communication between common digital nerves that emerge from the median nerve and the ulnar nerve on the surface of the palm is known as Berrettini anastomosis or ramus communicans cum nervi ulnari in anatomical terminology[4] [31] ([Figs. 7] and [8]).


Variations of the Berrettini anastomosis exist, and communications between the fourth common digital ulnar nerve and the third common digital median nerve may explain the variations in digital sensory innervation. The anastomotic branch originates most commonly from the fourth common digital nerve of the ulnar nerve, communicating distally to the third common digital nerve of the median nerve.[32] Its incidence varies drastically, between 4% and 94%, which is why some anatomists consider the Berrettini anastomosis a normal anatomical structure, and not an anatomical variation; however, this discussion is quite controversial.[5] [32] [33] [34]
In 1991, Meals and Calkins[35] gave notoriety to the term Berrettini anastomosis in honor of Pietro Berrettini Cortonensi, a famous artist known for his painting of Santa Cecilia, who illustrated the occurrence of superficial communication between the ulnar and median nerves, in the engravings ofthe book Tabulae Anatomicae,[37] published in 1741.[35] [36] [37]
Berrettini's anastomosis is believed to be purely sensitive, and an injury to it results in reduced sensitivity in the region between the third and fourth fingers.[38]
Rollins and Meals[39] described the loss of sensory innervation caused by traumatic injury to the Berrettini anastomosi:, their patient reported symptoms of paresthesia in the area between the middle and ring fingers.
Loukas et al.[5] reported that there were no differences observed in the morphometric or topographic parameters according to the thnicity, age or gender of the individual.
Some anatomy books do not mention the presence of this anastomotic branch, but some atlases illustrate it as a communicating branch or anastomotic branch.[18] [36] [39] [40] [41] [42] Rollins and Meals[39] paid attention to the fact that the presence of the Berrettini anastomosis can cause changes in the pattern of innervation of the fingers, according to the lesion and its topography, such as the persistence of sensitivity in the ulnar edge of the middle finger or in the radial edge of the ring finger in lesions to the median and ulnar nerves in the region of the wrist. The anastomosis is located in the middle palmar region, at a point of intersection between an axial line of the fourth finger and the Kaplan cardinal line.[43]
The Berrettini anastomosis is important because injuries can occur in the volar surface on the hand. This is due to the fact that surgeons who deal with carpal tunnel syndrome are working superficially in the area of the Berrettini anastomosis, which is why knowledge of it is extremely important.[5]
#
Riche-Cannue Anastomosis
The Riche-Cannieu anastomosis is located between the ulnar and median nerves in the hand. It consists of a communication between the recurrent branch of the median nerve and the deep branch of the ulnar nerve in the tenar region, and it can alter the motor innervation of the hand[44] ([Figs. 9] and [10]). Both motor and sensitive fibers may be involved, with the possibility of three types of clinical presentation: the hand totally innervated by the ulnar nerve; motor fibers only from the ulnar nerve; or the hand with normal innervation by the median nerve, partially supplied by the ulnar nerve.[45] It was first described by Cannieu in 1894, who reported an anastomosis between the recurrent branch of the median nerve and the ulnar nerve in 03 out of 20 anatomical pieces that he dissected.[38] Later, in 1897, Riche[46] found anastomoses in 3 out of 12 anatomical specimens.


The incidence is quite controversial in the literature, with studies showing different prevalence rates. Studies on anatomical dissection describe the following incidences: Cannieu[47]–7%; Bölükbaşi[48]–0%; Riche[46]–13%; Yang[49]–50%; Souza[50]–50%; Harness[51]–77%; and Caetano[52]–100%. In an electrophysiological study,[38] the incidence found was of 83.3%. According to Boland et al.,[53] there is a family tendency for autosomal dominant inheritance.
The location of the Riche-Cannieu anastomosis would be at the intersection of a line perpendicular to the midpoint of the proximal flexor crease of the first finger and the axial line of the second finger.[43]
There are three types of connections described: type I: between the deep branch of the ulnar nerve and the recurrent branch of the median nerve for the two heads of the flexor pollicis brevis muscle; type II: between the deep branch of the ulnar nerve and the branch of the median nerve, within the muscular body of the transverse head of the adductor pollicis; type III: communication between these two nerves within the lumbrical muscle body.[46]
Regarding the clinical repercussion, the presence of this anastomosis can cause a risk of injury during surgical procedures, and also hinder the interpretation of electrophysiological studies in the diagnosis of neuropathies. Carpal tunnel syndrome, in particular, has been associated with exacerbated or decreased symptoms in the presence of these anastomoses.[52] [54] It can generate an “ulnar-hand” phenomenon in some cases, in which the muscles in the tenar eminence only present innervation from the ulnar nerve, with no contribution from the median nerve.[55]
In an electroneuromyographic study,[56] it caused difficulty in interpreting the results, especially in the evaluation of the lesions to the median nerve, the opponens pollicis muscle, amd the abductor pollicis brevis muscle.
These anastomoses can cause confusion in the diagnosis of lesions: complete lesion to the median nerve, in a situation in which the Riche-Cannieu anastomosis exists, can be interpreted as a partial nerve injury, for example. In cases of injury to the ulnar nerve, the presence of signs of denervation of the muscles innervated by the median nerve (the opponens pollicis muscle and the abductor pollicis brevis muscle) may lead to the suspicion of of brachial plexus injury (C8-T1).[56] [57]
#
Conclusion
Anastomoses between the median and ulnar nerves in the forearm and hand can cause confusion in the diagnosis of conditions affecting the nerve that supplies the intrinsic muscles of the hand. Crossing axons can innervate the intrinsic muscles supplied by the ulnar nerve, the median nerve, or both. This explains the cases in which nerve damage in the forearm does not cause changes in the muscles of the hand. The symptoms of carpal tunnel syndrome may be incomplete or exacerbated due to the existence of these anastomoses, which alter the innervation of the upper limb. Or a traumatic nerve injury at the level of the forearm may be mistakenly interpreted as a partial injury in the median nerve or ulnar nerve, and importance should also be given to its topography to prevent injuries to the anastomotic branches in upper-limb surgical procedures. Therefore, knowledge of these anastomoses is important, given their impact on the surgical treatment in the forearm and hand, to avoid iatrogenic injuries and prevent complications in surgeries, as well as in the clinical and electromyographic diagnosis of partial and total injuries to the median and ulnar nerves.
#
#
Conflict of Interests
The authors have no conflict of interests to declare.
-
References
- 1 Mannerfelt L. Studies on the hand in ulnar nerve paralysis. A clinical-experimental investigation in normal and anomalous innervation. Acta Orthop Scand 1966; (Suppl. 87) 1
- 2 Kimura J, Murphy MJ, Varda DJ. Electrophysiological study of anomalous innervation of intrinsic hand muscles. Arch Neurol 1976; 33 (12) 842-844
- 3 Greenberg MS. Manual de Neurocirurgia.7.ed – Porto Alegre. Art Med 2013
- 4 Dogan NU, Uysal II, Seker M. The communications between the ulnar and median nerves in upper limb. Neuroanat 2009; 8: 15-19
- 5 Loukas M, Louis Jr RG, Stewart L. et al. The surgical anatomy of ulnar and median nerve communications in the palmar surface of the hand. J Neurosurg 2007; 106 (05) 887-893
- 6 Meenakshi-Sundaram S, Sundar B, Arunkumar MJ. Marinacci communication: an electrophysiological study. Clin Neurophysiol 2003; 114 (12) 2334-2337
- 7 Riechers II RG, Landau ME, Farber G, Campbell WW. Damage to sensory fibers in a martin-gruber anomaly after biceps tendon repair. J Clin Neuromuscul Dis 2005; 6 (04) 162-166
- 8 Martin R. Tal om Nervus alimanna Egenskaper I Maniskans Kropp. 1763
- 9 Gruber W. Ueber die Verbindung des Nervus medianus mit dem Nervus ulnaris am Unterame des Menschen um der Saugethiere. 1870
- 10 Nakashima T. An anatomic study on the Martin-Gruber anastomosis. Surg Radiol Anat 1993; 15 (03) 193-195
- 11 Thomson A, Hollinshead W. Anatomy for surgeons. The back and the limbs. 1958
- 12 Hirasawa K. Untersuchungen uber das periphere nervensystem, plexus brachialis and die nerven der oberen extremitat. 1931
- 13 Taams KO. Martin–Gruber connections in South Africa. An anatomical study. J Hand Surg Br 1997; 22 (03) 328-330
- 14 Roy J, Henry BM, PĘkala PA. et al. Median and ulnar nerve anastomoses in the upper limb: A meta-analysis. Muscle Nerve 2016; 54 (01) 36-47
- 15 Cavalheiro CS, Filho MR, Pedro G, Caetano MF, Vieira LA, Caetano EB. Clinical repercussions of Martin-Gruber anastomosis: anatomical study. Rev Bras Ortop 2016; 51 (02) 214-223
- 16 Villar F. Quelques recherché sur les anastomoses des nerfs der member superier. 1905
- 17 Goss CM. Gray anatomia. 29 ed.. Rio de Janeiro: Guanabara Koogan; 1988
- 18 Sirinivasan R, Rhodes J. The median-ulnar anastomosis (Martin-Gruber) in normal and congenenitally abnormal fetuses. Arch Neurol 1981; 38 (07) 418-419
- 19 Crutchfield Ca. Gutmann L. Hereditary aspects of median-ulnar nerve communications. J Neurol Neurosurg Psychiatry 1980; 43 (01) 53-55
- 20 Piza-Katzer H. [Familial occurrence of Martin-Gruber anastomosis.]. Handchirurgie 1976; 8 (04) 215-218
- 21 Caetano EB, Vieira LÂ, Caetano MF, Cavalheiro CS, Razuk M, Sabongi JJ. Intramuscular Martin-Gruber anastomosis. Acta Ortop Bras 2016; 24 (02) 94-97
- 22 Brandsma J. Intrinsic minus hand. 1993
- 23 Hopf HC. Forearm ulnar-to-median nerve anastomosis of sensory axons. Muscle Nerve 1990; 13 (07) 654-656
- 24 Marinacci AA. The problem of unusual anomalous innervations of hand muscles:the value of electrodiagnosis in its evaluation. Bull Los Angel Neuro Soc 1964; 29: 133-142
- 25 Almeida A, Vitti M, Garbino J. Estudo anatômico da anastomose de Martin-Gruber. Hansen Int 1999; 24 (01) 15-20
- 26 Sperino G. Anatomia Del cimpanzé. 1888
- 27 Rosen AD. Innervation of the hand: an electromyographic study. Electromyogr Clin Neurophysiol 1973; 13 (02) 175-178
- 28 Golovchinsky V. Ulnar-to-median anastomosis and its role in the diagnosis of lesions of the median nerve at the elbow and the wrist. Electromyogr Clin Neurophysiol 1990; 30 (01) 31-34
- 29 Felippe MM, Telles FL, Soares ACL, Felippe FM. Anastomosis Between the median nerve and ulnar nerve in the forearm. J Morphol Sci 2012; 29 (01) 23-26
- 30 Sraj SA, Moussallem CD, Stafford JB. Cubital tunnel syndrome presenting with carpal tunnel symptoms: clinical evidence for sensory ulnar-to-median nerve communication. Am J Orthop 2009; 38 (06) E104-E106
- 31 Federative Committee on Anatomy Technology. Terminologia anatomica. Stuttgart thieme; 1998
- 32 Ferrari GP, Gilbert A. The superficial anastomosis on the palm of the hand between the ulnar and median nerves. J Hand Surg [Br] 1991; 16 (05) 511-514
- 33 Don Griot JPWD, Zuidam JM, van Kooten EO, Prosé LP, Hage JJ. Anatomic study of the ramus communicans between the ulnar and median nerves. J Hand Surg Am 2000; 25 (05) 948-954
- 34 Tagil SM, Bozkurt MC, Ozçakar L, Ersoy M, Tekdemir I, Elhan A. Superficial palmar communications between the ulnar and median nerves in Turkish cadavers. Clin Anat 2007; 20 (07) 795-798
- 35 Meals RA, Calkins ER. Anomalous innervation of the upper extremity in Gelberman RH: Operative nerve repair and reconstruction. Philadelphia, JB: Lippincott; 1991: 197-204
- 36 Anson BJ. Human anatomy. New York: McGraw-Hill; 1966
- 37 Berrettini P. Tabulae anatomicae. Roma: F. Amidei; 1741
- 38 Kimura I, Ayyar DR, Lippmann SM. Electrophysiological verification of the ulnar to median nerve communications in the hand and forearm. Tohoku J Exp Med 1983; 141 (03) 269-274
- 39 Rollins J, Meals RA. Recognition of acutely lacerated ulnar nerve-median nerve palmar communicating branch. A case report. Clin Orthop Relat Res 1985; (201) 91-93
- 40 Grant JCB. Atlas de anatomia. Rio de Janeiro: Editora Guanabara koogan; 1946
- 41 Wolf-Heidegger G. Atlas of sistematic human anatomy. New York: S.Karger; 1962
- 42 Ferner H, Staubesand J. Sobotta, atlas de anatomia humana. Rio de janeiro: editora Koogan; 1984
- 43 Rojas RL, Nieto RLE, Sepúlveda C. Proyección topográfica de las anastomosis entre nervios mediano y cubital en antebrazo y mano. Cirurgía Plástica 2014; 24 (02) 82-87
- 44 Russomano S, Herbison GJ, Baliga A, Jacobs SR, Moore J. Riche-Cannieu anastomosis with partial transection of the median nerve. Muscle Nerve 1995; 18 (01) 120-122
- 45 Gutmann L. AAEM minimonograph #2: important anomalous innervations of the extremities. Muscle Nerve 1993; 16 (04) 339-347
- 46 Riche D. Le nerf cubital et les muscles de l'eminence thenar. Bull Mem Soc Anat Paris 1897; •••: 251-252
- 47 Cannieu A. Recherche sur l'innervation de l'eminence thenar par le cubital. J Med Bordeaux 377-379 1896;
- 48 Bölükbaşi O, Turgut M, Akyol A. Ulnar to median nerve anastomosis in the palm (Riches-Cannieu anastomosis). Neurosurg Rev 1999; 22 (2-3): 138-139
- 49 Yang H, Gil Y, Kim S, Bang J, Choi H, Lee HY. From the brachial plexus to the hand, multiple connections between the median and ulnar nerves may serve as bypass routes for nerve fibres. J Hand Surg Eur Vol 2016; 41 (06) 648-656
- 50 Souza OM. Contribuição ao estudo da inervação dos Musculi Hypotenaris et tenaris no homem. São Paulo: 1975. . Tese: Escola Paulista de Medicina
- 51 Harness D, Sekeles E. The double anastomotic innervation of thenar muscles. J Anat 1971; 109 (Pt 3): 461-466
- 52 Caetano EB, Vieira LA, Sabongi Neto JJ, Caetano MF, Sabongi RG. Anastomose de Riche-Cannieu: estrutura, função e significância clínica. Rev Bras Ortop 2019; 54: 564-571
- 53 Boland RA, Krishnan AV, Kiernan MC. Riche-Cannieu anastomosis as an inherited trait. Clin Neurophysiol 2007; 118 (04) 770-775
- 54 Caetano EB, Morad JFM. Estudo anatômico da anastomose entre o nervo mediano e o ramo profundo do nervo ulnar (anastomose de Cannieu e Riché). Rev. bras. ciênc. Morfol 247 1987;
- 55 Brown JV, Landau ME. Sparing of the second lumbrical in a Riche-Cannieu anastomosis: the nearly all-ulnar hand. J Clin Neuromuscul Dis 2013; 14 (04) 184-187
- 56 Saperstein DS, King RB. Motor neuron presentation of an ulnar neuropathy and Riche-Cannieu anastomosis. Electromyogr Clin Neurophysiol 2000; 40 (02) 119-122
- 57 Kazakos KJ, Smyrnis A, Xarchas KC, Dimitrakopoulou A, Verettas DA. Anastomosis between the median and ulnar nerve in the forearm. An anatomic study and literature review. Acta Orthop Belg 2005; 71 (01) 9-35
- 58 Duran JTC, Arquez HF. Anastomosis between median and ulnar nerve in forearm and hand. Journal of Chemical and Pharmaceutical Research 2016; 8 (08) 675-680
Address for correspondence
Publikationsverlauf
Eingereicht: 13. Juli 2020
Angenommen: 16. November 2020
Artikel online veröffentlicht:
29. März 2021
© 2021. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Mannerfelt L. Studies on the hand in ulnar nerve paralysis. A clinical-experimental investigation in normal and anomalous innervation. Acta Orthop Scand 1966; (Suppl. 87) 1
- 2 Kimura J, Murphy MJ, Varda DJ. Electrophysiological study of anomalous innervation of intrinsic hand muscles. Arch Neurol 1976; 33 (12) 842-844
- 3 Greenberg MS. Manual de Neurocirurgia.7.ed – Porto Alegre. Art Med 2013
- 4 Dogan NU, Uysal II, Seker M. The communications between the ulnar and median nerves in upper limb. Neuroanat 2009; 8: 15-19
- 5 Loukas M, Louis Jr RG, Stewart L. et al. The surgical anatomy of ulnar and median nerve communications in the palmar surface of the hand. J Neurosurg 2007; 106 (05) 887-893
- 6 Meenakshi-Sundaram S, Sundar B, Arunkumar MJ. Marinacci communication: an electrophysiological study. Clin Neurophysiol 2003; 114 (12) 2334-2337
- 7 Riechers II RG, Landau ME, Farber G, Campbell WW. Damage to sensory fibers in a martin-gruber anomaly after biceps tendon repair. J Clin Neuromuscul Dis 2005; 6 (04) 162-166
- 8 Martin R. Tal om Nervus alimanna Egenskaper I Maniskans Kropp. 1763
- 9 Gruber W. Ueber die Verbindung des Nervus medianus mit dem Nervus ulnaris am Unterame des Menschen um der Saugethiere. 1870
- 10 Nakashima T. An anatomic study on the Martin-Gruber anastomosis. Surg Radiol Anat 1993; 15 (03) 193-195
- 11 Thomson A, Hollinshead W. Anatomy for surgeons. The back and the limbs. 1958
- 12 Hirasawa K. Untersuchungen uber das periphere nervensystem, plexus brachialis and die nerven der oberen extremitat. 1931
- 13 Taams KO. Martin–Gruber connections in South Africa. An anatomical study. J Hand Surg Br 1997; 22 (03) 328-330
- 14 Roy J, Henry BM, PĘkala PA. et al. Median and ulnar nerve anastomoses in the upper limb: A meta-analysis. Muscle Nerve 2016; 54 (01) 36-47
- 15 Cavalheiro CS, Filho MR, Pedro G, Caetano MF, Vieira LA, Caetano EB. Clinical repercussions of Martin-Gruber anastomosis: anatomical study. Rev Bras Ortop 2016; 51 (02) 214-223
- 16 Villar F. Quelques recherché sur les anastomoses des nerfs der member superier. 1905
- 17 Goss CM. Gray anatomia. 29 ed.. Rio de Janeiro: Guanabara Koogan; 1988
- 18 Sirinivasan R, Rhodes J. The median-ulnar anastomosis (Martin-Gruber) in normal and congenenitally abnormal fetuses. Arch Neurol 1981; 38 (07) 418-419
- 19 Crutchfield Ca. Gutmann L. Hereditary aspects of median-ulnar nerve communications. J Neurol Neurosurg Psychiatry 1980; 43 (01) 53-55
- 20 Piza-Katzer H. [Familial occurrence of Martin-Gruber anastomosis.]. Handchirurgie 1976; 8 (04) 215-218
- 21 Caetano EB, Vieira LÂ, Caetano MF, Cavalheiro CS, Razuk M, Sabongi JJ. Intramuscular Martin-Gruber anastomosis. Acta Ortop Bras 2016; 24 (02) 94-97
- 22 Brandsma J. Intrinsic minus hand. 1993
- 23 Hopf HC. Forearm ulnar-to-median nerve anastomosis of sensory axons. Muscle Nerve 1990; 13 (07) 654-656
- 24 Marinacci AA. The problem of unusual anomalous innervations of hand muscles:the value of electrodiagnosis in its evaluation. Bull Los Angel Neuro Soc 1964; 29: 133-142
- 25 Almeida A, Vitti M, Garbino J. Estudo anatômico da anastomose de Martin-Gruber. Hansen Int 1999; 24 (01) 15-20
- 26 Sperino G. Anatomia Del cimpanzé. 1888
- 27 Rosen AD. Innervation of the hand: an electromyographic study. Electromyogr Clin Neurophysiol 1973; 13 (02) 175-178
- 28 Golovchinsky V. Ulnar-to-median anastomosis and its role in the diagnosis of lesions of the median nerve at the elbow and the wrist. Electromyogr Clin Neurophysiol 1990; 30 (01) 31-34
- 29 Felippe MM, Telles FL, Soares ACL, Felippe FM. Anastomosis Between the median nerve and ulnar nerve in the forearm. J Morphol Sci 2012; 29 (01) 23-26
- 30 Sraj SA, Moussallem CD, Stafford JB. Cubital tunnel syndrome presenting with carpal tunnel symptoms: clinical evidence for sensory ulnar-to-median nerve communication. Am J Orthop 2009; 38 (06) E104-E106
- 31 Federative Committee on Anatomy Technology. Terminologia anatomica. Stuttgart thieme; 1998
- 32 Ferrari GP, Gilbert A. The superficial anastomosis on the palm of the hand between the ulnar and median nerves. J Hand Surg [Br] 1991; 16 (05) 511-514
- 33 Don Griot JPWD, Zuidam JM, van Kooten EO, Prosé LP, Hage JJ. Anatomic study of the ramus communicans between the ulnar and median nerves. J Hand Surg Am 2000; 25 (05) 948-954
- 34 Tagil SM, Bozkurt MC, Ozçakar L, Ersoy M, Tekdemir I, Elhan A. Superficial palmar communications between the ulnar and median nerves in Turkish cadavers. Clin Anat 2007; 20 (07) 795-798
- 35 Meals RA, Calkins ER. Anomalous innervation of the upper extremity in Gelberman RH: Operative nerve repair and reconstruction. Philadelphia, JB: Lippincott; 1991: 197-204
- 36 Anson BJ. Human anatomy. New York: McGraw-Hill; 1966
- 37 Berrettini P. Tabulae anatomicae. Roma: F. Amidei; 1741
- 38 Kimura I, Ayyar DR, Lippmann SM. Electrophysiological verification of the ulnar to median nerve communications in the hand and forearm. Tohoku J Exp Med 1983; 141 (03) 269-274
- 39 Rollins J, Meals RA. Recognition of acutely lacerated ulnar nerve-median nerve palmar communicating branch. A case report. Clin Orthop Relat Res 1985; (201) 91-93
- 40 Grant JCB. Atlas de anatomia. Rio de Janeiro: Editora Guanabara koogan; 1946
- 41 Wolf-Heidegger G. Atlas of sistematic human anatomy. New York: S.Karger; 1962
- 42 Ferner H, Staubesand J. Sobotta, atlas de anatomia humana. Rio de janeiro: editora Koogan; 1984
- 43 Rojas RL, Nieto RLE, Sepúlveda C. Proyección topográfica de las anastomosis entre nervios mediano y cubital en antebrazo y mano. Cirurgía Plástica 2014; 24 (02) 82-87
- 44 Russomano S, Herbison GJ, Baliga A, Jacobs SR, Moore J. Riche-Cannieu anastomosis with partial transection of the median nerve. Muscle Nerve 1995; 18 (01) 120-122
- 45 Gutmann L. AAEM minimonograph #2: important anomalous innervations of the extremities. Muscle Nerve 1993; 16 (04) 339-347
- 46 Riche D. Le nerf cubital et les muscles de l'eminence thenar. Bull Mem Soc Anat Paris 1897; •••: 251-252
- 47 Cannieu A. Recherche sur l'innervation de l'eminence thenar par le cubital. J Med Bordeaux 377-379 1896;
- 48 Bölükbaşi O, Turgut M, Akyol A. Ulnar to median nerve anastomosis in the palm (Riches-Cannieu anastomosis). Neurosurg Rev 1999; 22 (2-3): 138-139
- 49 Yang H, Gil Y, Kim S, Bang J, Choi H, Lee HY. From the brachial plexus to the hand, multiple connections between the median and ulnar nerves may serve as bypass routes for nerve fibres. J Hand Surg Eur Vol 2016; 41 (06) 648-656
- 50 Souza OM. Contribuição ao estudo da inervação dos Musculi Hypotenaris et tenaris no homem. São Paulo: 1975. . Tese: Escola Paulista de Medicina
- 51 Harness D, Sekeles E. The double anastomotic innervation of thenar muscles. J Anat 1971; 109 (Pt 3): 461-466
- 52 Caetano EB, Vieira LA, Sabongi Neto JJ, Caetano MF, Sabongi RG. Anastomose de Riche-Cannieu: estrutura, função e significância clínica. Rev Bras Ortop 2019; 54: 564-571
- 53 Boland RA, Krishnan AV, Kiernan MC. Riche-Cannieu anastomosis as an inherited trait. Clin Neurophysiol 2007; 118 (04) 770-775
- 54 Caetano EB, Morad JFM. Estudo anatômico da anastomose entre o nervo mediano e o ramo profundo do nervo ulnar (anastomose de Cannieu e Riché). Rev. bras. ciênc. Morfol 247 1987;
- 55 Brown JV, Landau ME. Sparing of the second lumbrical in a Riche-Cannieu anastomosis: the nearly all-ulnar hand. J Clin Neuromuscul Dis 2013; 14 (04) 184-187
- 56 Saperstein DS, King RB. Motor neuron presentation of an ulnar neuropathy and Riche-Cannieu anastomosis. Electromyogr Clin Neurophysiol 2000; 40 (02) 119-122
- 57 Kazakos KJ, Smyrnis A, Xarchas KC, Dimitrakopoulou A, Verettas DA. Anastomosis between the median and ulnar nerve in the forearm. An anatomic study and literature review. Acta Orthop Belg 2005; 71 (01) 9-35
- 58 Duran JTC, Arquez HF. Anastomosis between median and ulnar nerve in forearm and hand. Journal of Chemical and Pharmaceutical Research 2016; 8 (08) 675-680