
Subscribe to RSS
DOI: 10.1055/s-0041-1729998
Pyrocarbon Implant for Trapeziometacarpal Arthritis: Mid-term Clinical and Radiological Results
Article in several languages: English | español
Abstract
Pyrolytic carbon implants for trapeziometacarpal (TMC) arthritis have been extensively studied, but there is still discrepancy in the literature concerning the mid-term functional results. Our group describes the clinical and radiological results after five years of surgical management of TMC arthritis with Pyrodisk (Integra Life Sciences, Plainsboro, NJ, US). A total of 19 patients (2 males and 17 females) aged 56.45 ± 5.95 (range: 44 to 67) years were reviewed with a mean follow-up of 74.05 ± 14.43 (range: 60.00 to 105.83) months. At the final follow-up, the score on the Visual Analogue Scale (VAS) for pain was of 1.76 ± 2.05, the average score on the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire was of 22.73 ± 22.33, and all functional parameters were above the 90% barrier of the contralateral side. The progression of radiolucency was 89% at 1 year and 11% at 5 years of follow-up respectively, but it was not related to the clinical outcomes. The prevalence of subluxation (around one-fourth of the center of the implant) was of 24% in asymptomatic patients, and dislocation was not observed. The overall survival of the implant was of 89%. Revision took place in 11% of the cases due to persistent pain and implant breakage after direct impact. More than 75% of the patients were very or highly satisfied with the treatment. In conclusion, Pyrodisk enabled us to obtain good functional mid-term results, with an acceptable survival of the implant and low risk of dislocation. Radiological findings do not necessarily translate into clinical symptoms.
#
Introduction
The trapeziometacarpal (TMC) joint is commonly affected by arthritis, with a prevalence of 8% to 11% in the general population.[1] Although the conservative treatment plays a role in the improvement of symptoms and delay of progression,[2] surgery is frequently required. Numerous operative strategies have been shown to be effective in most cases, but no single method so far has emerged as superior to the others.[2] [3] [4] [5] [6]
The use of pyrolytic carbon prostheses has increased during the last decade,[7] [8] due to their biocompatibility, low coefficient of friction, and particular module of elasticity,[9] [10] which creates a high-strength and wear-resistant implant.[10] [11] [12] Studies published to date are discrepant on what concerns mid-term functional results: many describe favorable outcomes, namely excellent pain relief and patient satisfaction,[4] [8] [10] [13] [14] but some report high failure rates, secondary to breakage, instability, dislocation, loosening, and stiffness.[9] [15]
The pyrolytic carbon nonanatomic interposition implant (PyroDisk, Integra Life Sciences, Plainsboro, NJ, US) preserves thumb length and provides an anatomical basis for better thumb function and pinch strength.[16] It also avoids the problems with metallosis, bone cement and polyethylene wear observed with other implants.[13] The present work aims to address the clinical and radiological results in a series of patients submitted to surgery for isolated TMC primary osteoarthritis with Pyrodisk after 5 years of follow-up.
#
Materials and Methods
Study design. We conducted a retrospective observational study with patients diagnosed with isolated primary TMC degenerative osteoarthritis who were submitted to surgery at our center between February 2011 and March 2014. Revision and approval by the Ethical and Health Committee of Hospital de Braga, Braga, Portugal were obtained. The inclusion criteria were: age > 18 years at the time of the surgery, minimum follow-up of 60 months, primary TMC degenerative osteoarthritis, radiographic stages II and III according to Eaton classification,[17] [18] no prior TMC joint operations, and failure of the nonsurgical treatment. The exclusion criteria were: patients younger than 18 years of age, and radiographic evidence of scaphotrapeziotrapezoidal arthritis. The patients were identified in a database, and their medical records were reviewed. In total, 28 patients were selected (3 males and 25 females). From these, one patient was deceased, four were excluded due to loss of follow-up, and another four were excluded due to the unavailability of postoperative radiographs at the latest follow-up. A total of 19 patients (2 males and 17 females) were reviewed.
Surgical technique. All of the patients were operated under general or brachial plexus anesthesia. A pneumatic tourniquet was used (with 250 mmHg of pressure). The patients were in supine position, with the affected limb on a lateral table. A dorsolateral approach was used between Abdutor Pollicis Longus and Extensor Pollicis Brevis. The superficial branches of the radial nerve were identified and spread apart. A longitudinal capsulotomy of the TMC joint was performed from the mid-portion of the metacarpal to the base of the trapezium. An oscillating saw was used to remove 2 mm to 3mm from the base of the first metacarpal bone perpendicularly to the bone's long axis. A minimal resection of the trapezium was performed using an oscillating saw for parallel alignment to the metacarpal bone. A reamer was used to create a concavity between the base of the metacarpal bone of the thumb and the distal surface of the trapezium. A 3.2-mm drill was used to create a hole in the trapezium (from the proximal and dorsoradial aspects of the trapezium toward the center of the TMC joint) and in the first metacarpal bone (at 1.5 cm distal to the surface of the joint and from the dorsoradial aspect of the base of the metacarpal bone toward the center of the TMC joint as well). The proper implant was determined by selecting the trial implant that best fitted the base of the metacarpal bone and confirmed by intraoperative fluoroscopy. A hemiplasty of the Flexor Carpi Radiallis was performed. The tendon was first passed deep in relation to the tendons of the first dorsal compartment, and then, through the trapezium, the implant hole, and it was finally recovered through the metacarpal tunnel. The plasty was sutured dorsally back onto itself, considering the correct tension to ensure the stability of the TMC joint. The capsule and skin were closed with absorbable and non-absorbable sutures, respectively. A thumb spica plaster immobilization was used in every case.
Postoperative treatment. The sutures were removed at 15 days. The splint was removed at three weeks. Active range of motion (ROM) and physical rehabilitation started afterwards. The total time of the therapy was defined on an individual basis. Unrestrained activities were allowed at 12 weeks after surgery.
Outcome measures. At the final follow-up, the clinical and radiological data were reviewed. The Visual Analogue Scale (VAS) for pain, which ranges from 0 (no pain) to 10 (maximum pain imaginable), was applied. A 10-point scale from 0 (no satisfaction) to 10 (complete satisfaction) was used to record patient satisfaction with the outcome of the surgery and with the appearance of the digit after surgery. Global hand function was evaluated using the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire validated for the Portuguese population, which ranges from 0 (normal upper limb function) to 100 (no upper limb function). The motion of the thumb in opposition and adduction were assessed using the Kapandji classification.[19] Palmar abduction and radial abduction were evaluated with a classic goniometer. Grip strength (kg) and pinch strength (kg) were obtained by the mean of three repeated measures with a hand-held dynamometer (Lafayette Instrument, model 01165, Lafayette, IN, US). The preoperative radiographs were analyzed according to Eaton classification.[17] [18] The frontal and lateral views of the postoperative radiographs were reviewed using the software on the radiology imaging system (Sectra IDS7, version 21.1.3.2033, Sectra AB, Linköping, Sweden) at the immediate posteoperative time and at 1-year and 5-year of follow-up. The coronal and sagittal alignments of the implant in relation to the long axis of the TMC joint were measured as described by Barrera-Ochoa et al.:[13] the base of the TMC joint was divided into quarters on the front and lateral views, and the position of the implant was defined as centered, one-fourth displaced, one-half displaced, and more than one-half displaced. The periprosthetic lucency was measured using a modification of the system described by Herren et al.[20] for pyrocarbon proximal interphalangeal joint arthroplasty: 0–radiolucent line (0.5 mm) around the implant on a plain radiograph from the pyrolitic carbon coating; 1–radiolucent line present measuring ≤ 1 mm in width at any point around the implant; 2–radiolucent line > 1 mm in width at any point around the implant; 3–macroscopic displacement of the implant (more than one-fourth of the base of the first metacarpal bone).
Statistical analysis. The quantitative variables were described as means and standard deviations using the GraphPad Prism (GraphPad Software, Inc., San Diego, CA, US) software, version 8 for Windows 10. The results of ROM and strength were expressed as percentages of the contralateral limb function. Implant survival was presented as percentages. The correlation between the clinical results (ROM and strength) and the radiological features (position of implant and radiolucency) was tested using the Spearman rank correlation test with a 95% confidence interval (95%CI) and p < 0.05.
#
Results
A total of 19 patients (2 males and 17 females) were reviewed. The patients had a mean age of 56.45 ± 5.95 (range: 44 to 67) years, and the mean follow-up was of 74.05 ± 14.43 (range: 60.00 to 105.83) months. In total, 32% and 68% were identified as Eaton stages II and III, respectively. The dominant side was affected in 63% of the sample. A total of 3 out of 19 patients had already undergone surgery in the opposite hand: one patient (patient 7) had been submited to a total TMC arthroplasty with a ball-and-socket implant, another patient (patient 13) had undergone the placement of a pyrocarbon implant with the same technique, and another one (patient 14) had been submitted to a primary repair for an acute injury of the ulnar collateral ligament of the metacarpophalangeal joint of the thumb. Two patients underwent revision before the end of the follow-up. The authors chose to include them in the implant survival analysis, but their final clinical results are not displayed, neither are their radiological findings after revision.
At the latest follow-up, the mean score on the VAS for pain was of 1.76 ± 2.05, and the average score on the QuickDASH was of 22.73 ± 22.33. The mean time to return to work was of 4.07 ± 2.92 months, but 12 out of 19 patients were retired at the time of the surgery. In total, 26% and 82% of the patients were very or highly satisfied (score ≥ 8 out of 10) with the general treatment and cosmetic appearance, respectively. These results are detailed in [Table 1].
|
VAS (0-10) |
QuickDASH (0-100) |
Time to return to work (months) |
Global satisfaction score (0-10) |
Cosmetic appearance satisfaction score (0-10) |
Radiolucency* |
Implant position** |
Revision (Yes/No) |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Postoperative period |
1 year |
5 years |
Postop. |
1 year |
5 years |
|||||||
|
Patient 1 |
0 |
0.00 |
NA |
10 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 2 |
0 |
9.09 |
4.00 |
10 |
10 |
0 |
1 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 3 |
0 |
0.00 |
NA |
10 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 4 |
4 |
4.55 |
NA |
9 |
9 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 5 |
4 |
22.73 |
7.00 |
7 |
7 |
0 |
2 |
3 |
Centered |
Centered |
¼ displaced |
No |
|
Patient 6 |
5 |
61.36 |
3.00 |
8 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 7 |
5 |
56.82 |
1.50 |
10 |
10 |
0 |
1 |
1 |
Centered |
Centered |
Centered |
No |
|
Patient 8 |
2 |
36.36 |
NA |
10 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 9 |
0 |
2.27 |
NA |
10 |
8 |
0 |
1 |
1 |
Centered |
Centered |
¼ displaced |
No |
|
Patient 10 |
0 |
9.09 |
NA |
10 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 11 |
5 |
50.00 |
NA |
10 |
10 |
0 |
0 |
0 |
Centered |
Centered |
Centered |
No |
|
Patient 12 |
2 |
38.64 |
1.00 |
7 |
10 |
0 |
1 |
1 |
Centered |
Centered |
Centered |
No |
|
Patient 13 |
0 |
11.36 |
3.00 |
10 |
10 |
3 |
3 |
3 |
¼ displaced |
¼ displaced |
¼ displaced |
No |
|
Patient 14 |
2 |
52.27 |
NA |
8 |
8 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 15 |
0 |
29.55 |
NA |
9 |
10 |
0 |
2 |
2 |
Centered |
Centered |
Centered |
No |
|
Patient 16 |
1 |
0.00 |
NA |
10 |
10 |
0 |
1 |
1 |
Centered |
Centered |
Centered |
No |
|
Patient 17 |
0 |
2.27 |
9.00 |
10 |
9 |
0 |
3 |
3 |
Centered |
¼ displaced |
¼ displaced |
No |
|
Patient 18 |
NA |
NA |
NA |
NA |
NA |
0 |
NA |
NA |
Centered |
NA |
NA |
Yes |
|
Patient 19 |
NA |
NA |
NA |
NA |
NA |
0 |
2 |
NA |
Centered |
Centered |
NA |
Yes |
|
Mean |
1.76 |
22.73 |
4.07 |
9.29 |
9.47 |
– |
– |
– |
– |
– |
– |
– |
|
Standard deviation |
2.05 |
22.33 |
2.92 |
1.10 |
0.94 |
– |
– |
– |
– |
– |
– |
– |
The mean values of the functional parameters of grip and pinch strength were of 89 ± 26% and 93 ± 23% of the contralateral side, respectively. The mean values for palmar and radial abductions were of 33.06° ± 9.59° and 42.49° ± 17.14°, respectively. The mean values for opposition (Kapandji[19]) and retropulsion (Kapandji[19]) were of 8.47 ± 1.55 and 2.65 ± 0.61, respectively. The functional and ROM results are detailed in [Table 2].
|
Grip strenght (kg) |
Pinch strenght (kg) |
Palmar abduction (degrees) |
Radial abduction (degrees) |
Oppostion (Kapandji[19]) |
Retropulsion (Kapandji[19]) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Op. |
Ct. |
% op. side |
Op. |
Ct. |
% Op. side |
Op. |
Ct. side |
% Op. side |
Op. side |
Ct. side |
% Op. side |
Op. side |
Ct. side |
% Op. side |
Op. side |
Ct. side |
% Op. side |
|
|
side |
side |
side |
side |
side |
||||||||||||||
|
Patient 1 |
8.17 |
8.13 |
101% |
5.35 |
4.65 |
115% |
26 |
28 |
93% |
32 |
40 |
80% |
8 |
8 |
100% |
2 |
2 |
100% |
|
Patient 2 |
9.82 |
10.57 |
93% |
3.36 |
3.96 |
85% |
40 |
40 |
100% |
78 |
70 |
111% |
9 |
10 |
90% |
4 |
4 |
100% |
|
Patient 3 |
11.22 |
10.45 |
107% |
4.7 |
4.45 |
105% |
40 |
42 |
95% |
60 |
40 |
150% |
10 |
10 |
100% |
3 |
3 |
100% |
|
Patient 4 |
21.32 |
21.4 |
100% |
6.59 |
6.53 |
101% |
34 |
30 |
113% |
40 |
50 |
80% |
8 |
10 |
80% |
3 |
4 |
75% |
|
Patient 5 |
5.09 |
8.58 |
59% |
2.01 |
3.13 |
64% |
24 |
20 |
120% |
50 |
42 |
119% |
7 |
9 |
78% |
3 |
3 |
100% |
|
Patient 6 |
4.38 |
9.33 |
47% |
1.47 |
3.02 |
49% |
20 |
20 |
100% |
40 |
30 |
133% |
9 |
10 |
90% |
2 |
4 |
50% |
|
Patient 7 |
5.3 |
5.49 |
96% |
1.63 |
1.96 |
84% |
32 |
28 |
114% |
38 |
50 |
76% |
9 |
9 |
100% |
3 |
3 |
100% |
|
Patient 8 |
1.68 |
2.34 |
72% |
1.39 |
11.83 |
115% |
18 |
20 |
90% |
40 |
40 |
100% |
9 |
10 |
90% |
3 |
3 |
100% |
|
Patient 9 |
6.23 |
7.65 |
82% |
2.85 |
1.21 |
113% |
30 |
38 |
79% |
52 |
62 |
84% |
9 |
10 |
90% |
3 |
2 |
150% |
|
Patient 10 |
7.36 |
6.88 |
107% |
3.17 |
3.23 |
98% |
50 |
40 |
125% |
34 |
44 |
77% |
9 |
9 |
100% |
2 |
3 |
67% |
|
Patient 11 |
10.63 |
7.19 |
148% |
4.18 |
4.79 |
87% |
42 |
38 |
111% |
78 |
50 |
156% |
9 |
9 |
100% |
3 |
3 |
100% |
|
Patient 12 |
2.08 |
6.01 |
35% |
1.16 |
2.17 |
53% |
26 |
44 |
59% |
24 |
50 |
48% |
9 |
9 |
100% |
2 |
3 |
67% |
|
Patient 13 |
11.32 |
13.28 |
85% |
4.13 |
5.78 |
72% |
40 |
70 |
57% |
52 |
50 |
104% |
9 |
9 |
100% |
2 |
3 |
67% |
|
Patient 14 |
1.7 |
2.06 |
82% |
1.2 |
1.17 |
103% |
22 |
30 |
73% |
30 |
30 |
100% |
3 |
6 |
50% |
2 |
2 |
100% |
|
Patient 15 |
8.17 |
7.84 |
104% |
4.04 |
4.46 |
88% |
48 |
52 |
92% |
22 |
24 |
92% |
9 |
9 |
100% |
3 |
3 |
100% |
|
Patient 16 |
8.34 |
8.22 |
98% |
4.41 |
3.24 |
136% |
38 |
40 |
95% |
24 |
30 |
80% |
9 |
10 |
90% |
2 |
2 |
100% |
|
Patient 17 |
8.37 |
8.91 |
94% |
2.79 |
2.63 |
106% |
32 |
38 |
84% |
30 |
26 |
115% |
9 |
9 |
100% |
3 |
3 |
100% |
|
Patient 18 |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
|
Patient 19 |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
|
Mean |
7.70 |
8.49 |
89% |
3.20 |
3.46 |
93% |
33.06 |
36.35 |
94% |
42.59 |
42.82 |
100% |
8.47 |
9.18 |
92% |
2.65 |
2.94 |
93% |
|
Standard deviation |
4.71 |
4.32 |
26% |
1.60 |
1.51 |
23% |
9.59 |
12.59 |
20% |
17.14 |
12.55 |
28% |
1.55 |
1.01 |
13% |
0.61 |
0.66 |
22% |
At the immediate postoperative period, all implants except one were graded as Herren 0. In one case, the implant was macroscopically displaced (Herren grade 3). One year after surgery, 89% of progression of lucency was observed as follows: progression from grade 0 to grade 1 and from grade 1 to grade 2 were observed in 5 and 10 cases, respectively; progression from grade 2 to grade 3 was observed in 1 case. Between 1 and 5 years of follow-up, the progression of lucency observed was of 11%, as follows: progression from grade 1 to grade 2 in 1 case and from grade 2 to grade 3 in another case. No differences were observed in the rest of the implants. These radiological results are detailed in [Table 2].
At the immediate postoperative period, all implants except one were perfectly centered. In this case (patient 13), a displacement of one-fourth was observed. One year after surgery, another implant (patient 17) was displaced by one-fourth. Five years after surgery, 2 implants (patients 5 and 9) were displaced by one-fourth. All the other implants were perfectly centered. No major dislocations were noted. The percentage of displacements of one-fourth 1 and 5 years after surgery was, respectively, 11% and 24%. Progression of the previously observed displacement for each implant was not observed during follow-up. These data are also detailed in [Table 2].
There was no correlation between the radiological results and the clinical parameters, namely pain, score on the QuickDASH, ROM, or strength. During the follow-up, 2 implants were reviewed: the first patient (patient 18) suffered a fall while walking, with direct impact on the hand, 4.03 months after surgery. Due to the posttraumatic implant displacement (of one-fourth) and persistent pain, the patient underwent trapeziectomy, ligament reconstruction and tendon interposition according to the Burton-Pellegrini technique.[21] The second patient (patient 19) had persistent pain and TMC subluxation. In this case, trapeziectomy and suspension using a suture button was performed[22] at 60 months of follow-up. The overall implant survival with revision of the implant as the outcome measure was of 89% 5 years after surgery.
#
Discussion
The present work describes the clinical and radiological results after 5 years of surgical management of TMC arthritis with a pyrocarbon implant. Previous papers report that the mean postoperative VAS score for pain ranged from 0.5[16] to 4.9[7] points. Based on our data, the mean postoperative pain was of 1.76 ± 2.05, one of the lowest values reported in the current literature for this kind of technique. It is important to note, however, that 2 patients referred high values: one of them (patient 19) was reoperated at 60 months of follow-up due to persistent pain and subluxation; the other one (patient 7) was very satisfied, as he could perfectly perform his daily activities, and refused surgery. The average postoperative score on the QuickDASH was of 22.73 ± 22.33. These values are in line with those of the current literature, which presents mean values ranging from 17 to 31 points.[7] [13] [14] [16] [23] Although some of our patients scored as high as 50 and 60 points on the QuickDASH, they all referred satisfaction scores between 8 and 10, and stated no need for an additional surgery. In fact, 76% and 82% of the patients were very or highly satisfied (score ≥ 8 out of 10) with the general treatment and cosmetic appearance, respectively.
All the functional parameters (strength and ROM) were above the 90% barrier of the contralateral side. These are extremely positive results, and the values for grip and pinch strength are in fact slightly higher than the scores obtained in some of the papers that refer to similar techniques.[11] Opposition (Kapandji[19]), one of the most important features, had a mean value of 8.47 ± 1.55, which is in line with the values of previously-published studies.[7] [13] [16] [23]
The relationship between the functional results and the time to resume activities should be an interesting thing to examine, but it is hardly referred in the current literature. In our series, only 7 out of 19 patients were not retired at the time of the surgery, with an average time to return to work of 4.07 ± 2.92 months. It is a quite long period though, especially when involving young and active patients.
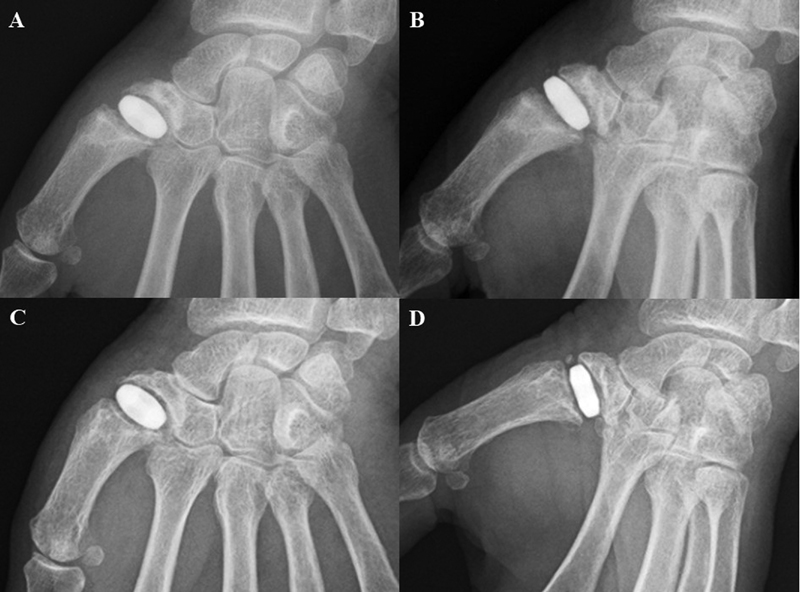
According to the literature, a normal radiolucent line is thought to correspond to the mantle of radiolucent pyrocarbon.[20] [24] [25] This lucency should not be interpreted as a complication, unless it increases above 1 mm or shows a significant progressive increase on serial studies.[25] In our results, all implants except one showed progressive radiolucency 1 year after surgery (89% of progression). However, between 1 and 5 years of follow-up, the progression of radiolucency was of only 11%. Similar results were found by Barrera-Ochoa et al.[13] Differences in progression according to time frames point out that the period in which most important radiological changes occur is within the first postoperative year ([Fig. 1, A,B,C,D]). Interestingly, Smeraglia et al.[23] have also found that evidence of instability in the first two postoperative years could be a predictor of the long-term durability of the implant.
However, it is important to emphasize that our radiological findings were not correlated to the clinical results. In a study of 31 patients aged 58 years with 13 months of follow-up, Stillwater et al.[25] have demonstrated similar results with adverse clinical outcomes for only 11 of the 31 implants showing evidence of loosening. Our work concurs, thus, with the idea that radiographic loosening per se should not be used as a predictor of implant failure or adverse clinical outcomes.[13] [25]
Dislocation is one of the most important complications of pyrocarbon implants,[8] [26] [27] occurring in up to 33% of the cases.[9] Pyrodisk is well known to be quite stable, since a ligamentous plasty is used for its stabilization, in contrast with other implants, such as Pi2 (Bioprofile, Grenoble, France), Pyrocardan (Tornier, Montbonnot Saint Martin, France) and NuGrip (Integra Life Sciences, Plainsboro, NJ, US).[9] [16] In the current study, no cases of dislocation were noted, but displacement of the implant occurred in 11% and 24% of the cases after 1 and 5 years of follow-up, respectively. These patients were asymptomatic, and were not reoperated ([Fig. 2, A] and [B]). Similar results were obtained by Barrera-Ochoa et al.[13]

In the present study, the overall implant survival with revision of the implant as the outcome measure was of 89% at 5 years after surgery. This data is in line with that of the current literature for Pyrodisk,[13] and it is higher than the survival expected for other pyrocarbon implants.[15] Revision was needed in two cases due to specific reasons. One patient (patient 18) presented with persistent pain, with subluxation of the implant during daily activities. We think this case was related to technical errors during the first surgical procedure. Another patient (patient 19) had a fall with direct impact on the hand, resulting in posttraumatic subluxation of the implant and persistent pain. The stability of the implant was assumed to be compromised ([Fig. 3, A] and [B]) and revision was carried out.

The present study has some important limitations. First of all, as a retrospective study, preoperative data for clinical parameters were not available. This is an important drawback, as it precludes the analysis of the potential changes after the surgery. Secondly, our sample is small and with a significant number of excluded patients, as explained earlier (only 19 patients out of an initial group of 27 patients), which limits the extrapolation of our conclusions to the general population. Prospective studies regarding preoperative features and larger samples should be performed.
#
Conclusion
The treatment of TMC osteoarthritis is currently demanding, as there is no gold-standard surgery. In the universe of pyrocarbon implants, Pyrodisk enabled us to obtain good functional results in the mid-term, with low risk of dislocation. Radiolucency lines do not relate to clinical outcomes, and should not be considered in the decision to perform revision.
#
#
-
References
- 1 Haara MM, Heliövaara M, Kröger H. et al. Osteoarthritis in the carpometacarpal joint of the thumb. Prevalence and associations with disability and mortality. J Bone Joint Surg Am 2004; 86 (07) 1452-1457
- 2 Bakri K, Moran SL. Thumb carpometacarpal arthritis. Plast Reconstr Surg 2015; 135 (02) 508-520
- 3 Wajon A, Vinycomb T, Carr E, Edmunds I, Ada L. Surgery for thumb (trapeziometacarpal joint) osteoarthritis. Cochrane Database Syst Rev 2015; (02) CD004631
- 4 Vitale MA, Taylor F, Ross M, Moran SL. Trapezium prosthetic arthroplasty (silicone, Artelon, metal, and pyrocarbon). Hand Clin 2013; 29 (01) 37-55
- 5 Gay AM, Cerlier A, Iniesta A, Legré R. Surgery for trapeziometacarpal osteoarthritis. Hand Surg Rehabil 2016; 35 (04) 238-249
- 6 Vermeulen GM, Slijper H, Feitz R, Hovius SE, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg Am 2011; 36 (01) 157-169
- 7 Cuenca-Llavall M, Lizano-Díez X, Cruz-Sánchez M, Cebamanos-Celma J, Pidemunt-Moli G. Comparative functional analysis between pyrolytic carbon prostheses and ligamentous suspension/reconstruction in the treatment of rhizarthrosis. Rev Esp Cir Ortop Traumatol 2018; 62 (05) 373-379
- 8 Russo S, Bernasconi A, Busco G, Sadile F. Treatment of the trapeziometacarpal osteoarthritis by arthroplasty with a pyrocarbon implant. Int Orthop 2016; 40 (07) 1465-1471
- 9 Maru M, Jettoo P, Tourret L, Jones M, Irwin L. Thumb carpometacarpal osteoarthritis: trapeziectomy versus pyrocarbon interposition implant (Pi2) arthroplasty. J Hand Surg Eur Vol 2012; 37 (07) 617-620
- 10 Haubold AD. On the durability of pyrolytic carbon in vivo. Med Prog Technol 1994; 20 (3-4): 201-208
- 11 Colegate-Stone TJ, Garg S, Subramanian A, Mani GV. Outcome analysis of trapezectomy with and without pyrocarbon interposition to treat primary arthrosis of the trapeziometacarpal joint. Hand Surg 2011; 16 (01) 49-54
- 12 Cook SD, Beckenbaugh RD, Redondo J, Popich LS, Klawitter JJ, Linscheid RL. Long-term follow-up of pyrolytic carbon metacarpophalangeal implants. J Bone Joint Surg Am 1999; 81 (05) 635-648
- 13 Barrera-Ochoa S, Vidal-Tarrason N, Correa-Vázquez E, Reverte-Vinaixa MM, Font-Segura J, Mir-Bullo X. Pyrocarbon interposition (PyroDisk) implant for trapeziometacarpal osteoarthritis: minimum 5-year follow-up. J Hand Surg Am 2014; 39 (11) 2150-2160
- 14 Odella S, Querenghi AM, Sartore R, DE Felice A, Dacatra U. Trapeziometacarpal osteoarthritis: pyrocarbon interposition implants. Joints 2015; 2 (04) 154-158
- 15 Martinez de Aragon JS, Moran SL, Rizzo M, Reggin KB, Beckenbaugh RD. Early outcomes of pyrolytic carbon hemiarthroplasty for the treatment of trapezial-metacarpal arthritis. J Hand Surg Am 2009; 34 (02) 205-212
- 16 Mariconda M, Russo S, Smeraglia F, Busco G. Partial trapeziectomy and pyrocarbon interpositional arthroplasty for trapeziometacarpal joint osteoarthritis: results after minimum 2 years of follow-up. J Hand Surg Eur Vol 2014; 39 (06) 604-610
- 17 Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am 1973; 55 (08) 1655-1666
- 18 Eaton RG, Glickel SZ. Trapeziometacarpal osteoarthritis. Staging as a rationale for treatment. Hand Clin 1987; 3 (04) 455-471
- 19 Kapandji A. Clinical evaluation of the thumb's opposition. J Hand Ther 1992; 5 (02) 102-106
- 20 Herren DB, Schindele S, Goldhahn J, Simmen BR. Problematic bone fixation with pyrocarbon implants in proximal interphalangeal joint replacement: short-term results. J Hand Surg (Edinburgh, Scotland) 2006; 31 (06) 643-651
- 21 Burton RI, Pellegrini Jr VD. Surgical management of basal joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplasty. J Hand Surg Am 1986; 11 (03) 324-332
- 22 Cox CA, Zlotolow DA, Yao J. Suture button suspensionplasty after arthroscopic hemitrapeziectomy for treatment of thumb carpometacarpal arthritis. Arthroscopy 2010; 26 (10) 1395-1403
- 23 Smeraglia F, Barrera-Ochoa S, Mendez-Sanchez G, Basso MA, Balato G, Mir-Bullo X. Partial trapeziectomy and pyrocarbon interpositional arthroplasty for trapeziometacarpal osteoarthritis: minimum 8-year follow-up. J Hand Surg Eur Vol 2020; 45 (05) 472-476
- 24 Vitale MA, Hsu CC, Rizzo M, Moran SL. Pyrolytic Carbon Arthroplasty versus Suspensionplasty for Trapezial-Metacarpal Arthritis. J Wrist Surg 2017; 6 (02) 134-143
- 25 Stillwater L, Memauri B, Ratanshi I, Islur A, Amaratunga T. Radiographic interpretation of carpometacarpal arthroplasty: correlation between radiographic loosening and clinical outcome. Skeletal Radiol 2017; 46 (08) 1057-1062
- 26 Vinycomb T, Crock J. Trapeziectomy with ligament reconstruction and tendon interposition: a minimum 10-year follow-up. Hand Surg 2013; 18 (03) 365-368
- 27 Szalay G, Meyer C, Kraus R, Heiss C, Schnettler R. [The operative treatment of rhizarthrosis with pyrocarbon spacer as replacement of the trapezium]. Handchir Mikrochir Plast Chir 2009; 41 (05) 300-305
Address for correspondence
Publication History
Received: 05 September 2020
Accepted: 21 January 2021
Article published online:
02 July 2021
© 2021. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Haara MM, Heliövaara M, Kröger H. et al. Osteoarthritis in the carpometacarpal joint of the thumb. Prevalence and associations with disability and mortality. J Bone Joint Surg Am 2004; 86 (07) 1452-1457
- 2 Bakri K, Moran SL. Thumb carpometacarpal arthritis. Plast Reconstr Surg 2015; 135 (02) 508-520
- 3 Wajon A, Vinycomb T, Carr E, Edmunds I, Ada L. Surgery for thumb (trapeziometacarpal joint) osteoarthritis. Cochrane Database Syst Rev 2015; (02) CD004631
- 4 Vitale MA, Taylor F, Ross M, Moran SL. Trapezium prosthetic arthroplasty (silicone, Artelon, metal, and pyrocarbon). Hand Clin 2013; 29 (01) 37-55
- 5 Gay AM, Cerlier A, Iniesta A, Legré R. Surgery for trapeziometacarpal osteoarthritis. Hand Surg Rehabil 2016; 35 (04) 238-249
- 6 Vermeulen GM, Slijper H, Feitz R, Hovius SE, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg Am 2011; 36 (01) 157-169
- 7 Cuenca-Llavall M, Lizano-Díez X, Cruz-Sánchez M, Cebamanos-Celma J, Pidemunt-Moli G. Comparative functional analysis between pyrolytic carbon prostheses and ligamentous suspension/reconstruction in the treatment of rhizarthrosis. Rev Esp Cir Ortop Traumatol 2018; 62 (05) 373-379
- 8 Russo S, Bernasconi A, Busco G, Sadile F. Treatment of the trapeziometacarpal osteoarthritis by arthroplasty with a pyrocarbon implant. Int Orthop 2016; 40 (07) 1465-1471
- 9 Maru M, Jettoo P, Tourret L, Jones M, Irwin L. Thumb carpometacarpal osteoarthritis: trapeziectomy versus pyrocarbon interposition implant (Pi2) arthroplasty. J Hand Surg Eur Vol 2012; 37 (07) 617-620
- 10 Haubold AD. On the durability of pyrolytic carbon in vivo. Med Prog Technol 1994; 20 (3-4): 201-208
- 11 Colegate-Stone TJ, Garg S, Subramanian A, Mani GV. Outcome analysis of trapezectomy with and without pyrocarbon interposition to treat primary arthrosis of the trapeziometacarpal joint. Hand Surg 2011; 16 (01) 49-54
- 12 Cook SD, Beckenbaugh RD, Redondo J, Popich LS, Klawitter JJ, Linscheid RL. Long-term follow-up of pyrolytic carbon metacarpophalangeal implants. J Bone Joint Surg Am 1999; 81 (05) 635-648
- 13 Barrera-Ochoa S, Vidal-Tarrason N, Correa-Vázquez E, Reverte-Vinaixa MM, Font-Segura J, Mir-Bullo X. Pyrocarbon interposition (PyroDisk) implant for trapeziometacarpal osteoarthritis: minimum 5-year follow-up. J Hand Surg Am 2014; 39 (11) 2150-2160
- 14 Odella S, Querenghi AM, Sartore R, DE Felice A, Dacatra U. Trapeziometacarpal osteoarthritis: pyrocarbon interposition implants. Joints 2015; 2 (04) 154-158
- 15 Martinez de Aragon JS, Moran SL, Rizzo M, Reggin KB, Beckenbaugh RD. Early outcomes of pyrolytic carbon hemiarthroplasty for the treatment of trapezial-metacarpal arthritis. J Hand Surg Am 2009; 34 (02) 205-212
- 16 Mariconda M, Russo S, Smeraglia F, Busco G. Partial trapeziectomy and pyrocarbon interpositional arthroplasty for trapeziometacarpal joint osteoarthritis: results after minimum 2 years of follow-up. J Hand Surg Eur Vol 2014; 39 (06) 604-610
- 17 Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am 1973; 55 (08) 1655-1666
- 18 Eaton RG, Glickel SZ. Trapeziometacarpal osteoarthritis. Staging as a rationale for treatment. Hand Clin 1987; 3 (04) 455-471
- 19 Kapandji A. Clinical evaluation of the thumb's opposition. J Hand Ther 1992; 5 (02) 102-106
- 20 Herren DB, Schindele S, Goldhahn J, Simmen BR. Problematic bone fixation with pyrocarbon implants in proximal interphalangeal joint replacement: short-term results. J Hand Surg (Edinburgh, Scotland) 2006; 31 (06) 643-651
- 21 Burton RI, Pellegrini Jr VD. Surgical management of basal joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplasty. J Hand Surg Am 1986; 11 (03) 324-332
- 22 Cox CA, Zlotolow DA, Yao J. Suture button suspensionplasty after arthroscopic hemitrapeziectomy for treatment of thumb carpometacarpal arthritis. Arthroscopy 2010; 26 (10) 1395-1403
- 23 Smeraglia F, Barrera-Ochoa S, Mendez-Sanchez G, Basso MA, Balato G, Mir-Bullo X. Partial trapeziectomy and pyrocarbon interpositional arthroplasty for trapeziometacarpal osteoarthritis: minimum 8-year follow-up. J Hand Surg Eur Vol 2020; 45 (05) 472-476
- 24 Vitale MA, Hsu CC, Rizzo M, Moran SL. Pyrolytic Carbon Arthroplasty versus Suspensionplasty for Trapezial-Metacarpal Arthritis. J Wrist Surg 2017; 6 (02) 134-143
- 25 Stillwater L, Memauri B, Ratanshi I, Islur A, Amaratunga T. Radiographic interpretation of carpometacarpal arthroplasty: correlation between radiographic loosening and clinical outcome. Skeletal Radiol 2017; 46 (08) 1057-1062
- 26 Vinycomb T, Crock J. Trapeziectomy with ligament reconstruction and tendon interposition: a minimum 10-year follow-up. Hand Surg 2013; 18 (03) 365-368
- 27 Szalay G, Meyer C, Kraus R, Heiss C, Schnettler R. [The operative treatment of rhizarthrosis with pyrocarbon spacer as replacement of the trapezium]. Handchir Mikrochir Plast Chir 2009; 41 (05) 300-305


