

Subscribe to RSS
DOI: 10.1055/s-0041-1741094
Soft-Tip Stylet and Saline Instillation Technique: Making Difficult Percutaneous CT-Guided Biopsies Possible
Authors


Abstract
Finding a safe needle path during percutaneous computed tomography-guided biopsy is sometimes difficult due to concern for injuring a vital structure. Saline instillation technique has been used to displace the structure out of the way. Another useful tool is a soft-tip stylet. A soft-tip also referred as blunt-tip stylet for the introducer cannula is provided with some coaxial biopsy sets in additional to standard sharp-tip stylet. While the sharp-tip stylet is fitted with introducer cannula for piercing skin, muscle, and fascia, a soft-tip stylet may be used for avoiding injury to structures like vessels and bowel loops especially while advancing introducer cannula through fatty tissue. Additionally, it is also useful for avoiding injury to nerves and giving pleural anesthesia. Although its use has been described in medical literature, many radiologists are still not utilizing this tool to its full potential. In this educational exhibit, various applications of soft-tip stylet and saline instillation technique have been depicted using representative cases.
Background
Percutaneous computed tomography (CT)-guided needle biopsy is an established technique for obtaining tissue sample from deep-seated lesions. However, sometimes it is difficult to find a safe needle path due to concern for injuring a vital structure. Many techniques like saline instillation technique or changing patient's position have been used to displace vital structures out of needle path.[1] [2] [3] [4] A soft-tip also referred to as blunt-tip stylet for the introducer cannula is provided with some coaxial biopsy sets in additional to standard sharp-tip stylet. Although its use has been described in medical literature, many radiologists are still not utilizing this tool to its full potential.[5] The combination of saline instillation and use of soft-tip stylet further increased safety of the procedure.
While using a sharp-tip stylet, it is important to create a wider saline window for safely advancing the needle without injuring adjacent structures. With a soft-tip stylet, usually a small amount of saline instillation is enough to dissect the fascial plane and displace any membranous structures, and this makes enough room for advancing the introducer cannula. Many a times, even saline instillation is not needed if introducer cannula along with soft-tip stylet is sliding smoothly without transgressing the anatomical structures.
Illustrative Cases
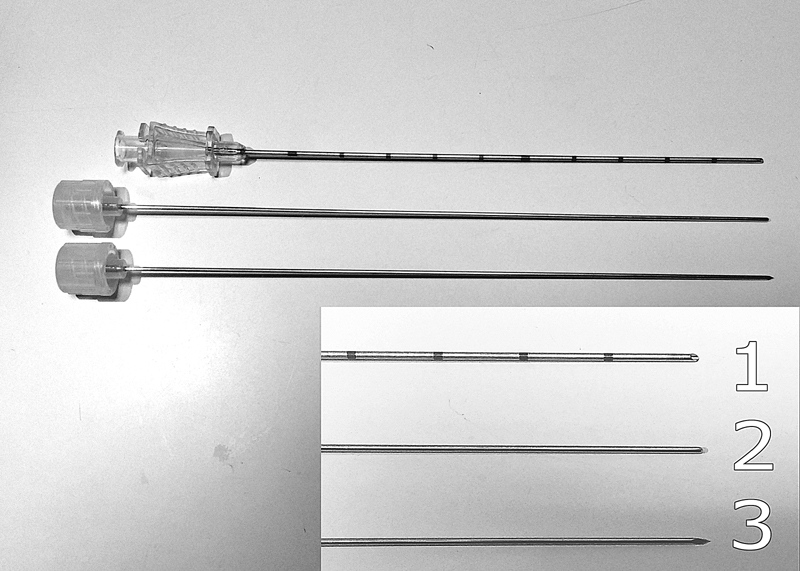
In all representative cases shown in this exhibit, percutaneous CT-guided biopsies were performed using an 18- or 20-gauge coaxial biopsy set (Bard Mission Core Biopsy Instrument, BARD, Arizona, United States) ([Fig. 1]). While a sharp-tip stylet is fitted with introducer cannula for piercing skin, muscle, and fascia, a soft-tip stylet may be used for avoiding injury to structures like lung, vessels, and bowel loops especially while advancing cannula through fatty tissue or between fascial planes ([Fig. 2]). The soft-tip stylet tends to displace the vital structures or slide over them rather than injuring them. Important applications of soft-tip stylet have been described below, and in some cases used in combination with saline instillation.

Neck region: A soft-tip stylet can be used to insert cannula close to the thyroid gland, pharynx, esophagus, and neck vessels ([Fig. 3]).

Mediastinum (anterior parasternal approach): A soft-tip stylet is helpful to slide the introducer cannula close to the ascending aorta, internal mammary arteries, pulmonary artery, and pleura ([Figs. 4] and [5]).


Mediastinum (posterior paravertebral approach): A soft-tip stylet helps to avoid injury to the spinal nerve roots, descending aorta, esophagus, lung, and azygos vein ([Fig. 6]).

Abdomen: A soft-tip stylet is used to slide introducer cannula over the kidney, liver, splenic capsule, and displacing the ureters or bowel loops ([Figs. 7], [8], [9]). It is also used for avoiding injury to mesenteric, splenic, epigastric, and iliac arteries ([Fig. 10]). The soft-tip stylet has also been used as a lever to displace a structure manually especially the bowel loops.[1]




Retroperitoneum (posterior approach): A soft-tip stylet is used to slip close to the kidney capsule, ureter, colon, vertebra, or spinal nerves. Similarly, it can be used to avoid injury to the inferior vena cava ([Figs. 11] and [12]).


Pelvis: A soft-tip stylet is used to avoid injury to the iliopsoas muscle, iliac vessels, ureter, colon, and urinary bladder ([Fig. 13]).

Other Uses
During vertebral or paravertebral biopsies, often the needle path runs close to exiting nerve, again a soft-tip stylet may help push the nerve aside while advancing the introducer cannula ([Fig. 14]). It is also useful for slipping introducer cannula close to bones without injuring periosteum which is a pain-sensitive structure.

During lung biopsies, giving local anesthesia to the pleura is important as it is a pain-sensitive structure. Pleural anesthesia is even more important during targeting small lung nodules, as these patients need to hold the breath at the time of advancing the needle into the lung; however, if the pleura is not anesthetized, the sharp pain of pleural puncture may cause movement or improper breath holding. Anesthetizing the pleura makes insertion of needle pain-free from chest wall into the lung. While manipulating the introducer cannula close to the pleura, soft-tip stylet is safer than sharp-tip stylet which may inadvertently cause pneumothorax ([Fig. 15]). A flat-tip bevel of the introducer cannula ([Fig. 1]) can also be manipulated close to the pleura safely and intercostal muscles may be pierced by making rotatory motions.

Limitations
Soft-tip stylet cannot be used to pierce tough structures like the skin, fascia, or muscles. It can distort the anatomy by pushing the anatomical structures rather than sliding over them; however, when used in between the fascial planes in conjunction with saline instillation, usually the introducer cannula slips easily over the anatomical structures. Similarly, the soft-tip stylet can be advanced through the fatty tissue while making gentle rotatory movements with little resistance.
Conclusion
During insertion of introducer cannula for coaxial CT-guided percutaneous biopsy, a soft-tip or blunt-tip stylet can be used for avoiding injury to structures like vessels and bowel loops especially while advancing the cannula through fatty tissue. Additionally, it is also useful for avoiding injury to nerves, muscles, and giving pleural anesthesia. A combination of saline instillation technique with soft-tip stylet further reduces the complications.
Conflicts of Interest
There are no conflicts of interest.
Acknowledgement
None.
Financial Support and Sponsorship
None.
-
References
- 1 Goodacre BW, Savage C, Zwischenberger JB, Wittich GR, vanSonnenberg E. Salinoma window technique for mediastinal lymph node biopsy. Ann Thorac Surg 2002; 74 (01) 276-277
- 2 Karampekios S, Hatjidakis AA, Drositis J, Gourtsoyiannis N. Artificial paravertebral widening for percutaneous CT-guided adrenal biopsy. J Comput Assist Tomogr 1998; 22 (02) 308-310
- 3 Zwischenberger JB, Savage C, Alpard SK, Anderson CM, Marroquin S, Goodacre BW. Mediastinal transthoracic needle and core lymph node biopsy: should it replace mediastinoscopy?. Chest 2002; 121 (04) 1165-1170
- 4 Gupta S, Seaberg K, Wallace MJ. et al. Imaging-guided percutaneous biopsy of mediastinal lesions: different approaches and anatomic considerations. Radiographics 2005; 25 (03) 763-786 , discussion 786–788
- 5 de Bazelaire C, Farges C, Mathieu O. et al. Blunt-tip coaxial introducer: a revisited tool for difficult CT-guided biopsy in the chest and abdomen. AJR Am J Roentgenol 2009; 193 (02) W144-8
Address for correspondence
Publication History
Article published online:
10 January 2022
© 2022. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Goodacre BW, Savage C, Zwischenberger JB, Wittich GR, vanSonnenberg E. Salinoma window technique for mediastinal lymph node biopsy. Ann Thorac Surg 2002; 74 (01) 276-277
- 2 Karampekios S, Hatjidakis AA, Drositis J, Gourtsoyiannis N. Artificial paravertebral widening for percutaneous CT-guided adrenal biopsy. J Comput Assist Tomogr 1998; 22 (02) 308-310
- 3 Zwischenberger JB, Savage C, Alpard SK, Anderson CM, Marroquin S, Goodacre BW. Mediastinal transthoracic needle and core lymph node biopsy: should it replace mediastinoscopy?. Chest 2002; 121 (04) 1165-1170
- 4 Gupta S, Seaberg K, Wallace MJ. et al. Imaging-guided percutaneous biopsy of mediastinal lesions: different approaches and anatomic considerations. Radiographics 2005; 25 (03) 763-786 , discussion 786–788
- 5 de Bazelaire C, Farges C, Mathieu O. et al. Blunt-tip coaxial introducer: a revisited tool for difficult CT-guided biopsy in the chest and abdomen. AJR Am J Roentgenol 2009; 193 (02) W144-8