
Subscribe to RSS
DOI: 10.1055/s-0042-1742602
Sagittal Alignment Concepts and Spinopelvic Parameters
Article in several languages: português | English
- Abstract
- Introduction
- Sagittal Misalignment Cascade
- Clinical presentations
- Main sagittal alignment measurements
- Lordosis distribution
- Pelvic Incidence and Lumbar Lordosis Mismatch
- Treatment
- Referências
Abstract
Spinal surgery continues to expand its horizons to care for disabled patients presenting pain and deformities. Over the past decade, our knowledge of spinal alignment, from the skull to the pelvis, has increased considerably. Such knowledge must expand to reach general orthopedists and improve the care required for so many people.
Global spinal alignment is a critical concept in understanding the impact of pathological conditions (degenerative diseases, traumas, deformities) and their treatment, including spinal instrumentation and arthrodesis. Therefore, the treatment of any spinal disease must include the knowledge of the complexity of the spinopelvic alignment.
At first, all parameters seem like pure mathematics, hardly applicable to the everyday life of the inattentive reader. However, it gradually becomes clear that, like everything else in orthopedics, biomechanics is an essential part of the knowledge of the musculoskeletal system, revealing the logic behind the physiology of movements.
The knowledge of the sagittal alignment concepts and spinopelvic parameteres provide a better comprehension of the axial and appendicular skeletons, increasing the understanding of the physiological and adaptive spinal processes in the face of the degenerative process that increases throughout life.
#
Introduction
The distinction between alignment and balance, which is virtually obvious to engineers, physiologists, and choreographers, is not so clear to orthopedic surgeons. Sagittal balance describes something dynamic, appreciating a person in motion. Optimal spinal alignment in the sagittal and coronal planes is mistakenly described as balance, for example, when we are interpreting panoramic radiographs of the spine. In the present article, we want to clarify the concept of stability with movement, a continuous process that defines balance.
These concepts have gained importance since the study by Schwab et al.[1] Before that, there were few works on the subject in the literature, but the number of publications has grown exponentially throughout the last decade.
In the sagittal plane, the normal spine has four curvatures (thoracic and sacral kyphoses, and cervical and lumbar lordoses) that correlate; this enables the correct body alignment to stand up and walk, with equal force distribution across the spine towards the lower limbs.
These curvatures present normal variations, but pathological processes and aging can change this sagittal alignment, modifying the distribution of these curves. This imbalance leads to a cascade of adaptation mechanisms, but with a high energy cost for the human body. These changes occur in the lower extremities and the pelvis, altering spinal alignment.[1]
Regarding alignment in the sagittal plane, Hardacker et al.[2] propose the following parameters:
-
Cervical lordosis: 30° to 50°. It is equally distributed over the cervical spine, with its apex at C4-C5.
-
Thoracic kyphosis: 20° to 50°. It increases with age, especially after 40 years; the greatest increase occurs in women.
-
Lumbar lordosis (LL): 30° to 80°. Two thirds of LL occur between L4 and S1.
Changes in any of these sagittal alignment components result in compensatory changes in adjacent segments.
#
Sagittal Misalignment Cascade
A subject with a correctly-aligned spine needs a virtually-imperceptible basal energy expenditure to maintain an upright position. On the other hand, a subject with an misaligned spine requires great effort to remain up, and may need crutches for better body weight distribution. Therefore, sustaining an upright position depends on three components: an aligned spine, good distribution of body weight, and adequate support provided by stabilizing muscles.
The defense mechanisms activated by sagittal malalignment include the use of stabilizing muscles (increasing energy expenditure), changes in sacral position (pelvic tilt, PT), and hip and knee flexion ([Figs. 1a] and [1b]).

Young patients and subjects with good muscle tone can deal with this situation better, but not older people or those with worse tonus. Aging worsens spine alignment because the deformity depletes the muscular system and contributes to the acceleration of disc degenerative processes; in addition, older patients may develop knee and hip osteoarthritis, which significantly increases energy consumption and pain.[3]
#
Clinical presentations
In younger patients, sagittal spinal malalignment occurs in cases of deformities such as scoliosis (coronal and sagittal deviations), Scheuermann disease, and spondylolisthesis, especially of the dysplastic or traumatic types.
In adults, these presentations are a natural progression of the lack of treatment or incorrect management (iatrogenic lesions) of the aforementioned diseases, or the result of osteoporotic fractures.
#
Main sagittal alignment measurements
Panoramic spinal radiography is the “gold standard” study to correctly assess sagittal alignment. It enables complete observation of the spine and its position regarding the sacrum, the femoral heads, and the femoral orientation.[4] [5] [6]
The main virtue of this test is its objectivity in assessing spinal alignment; as such, it reveals the magnitude of the deformity and enables an accurate preoperative planning to restore alignment.[7]
A new technology introduced about 15 years ago for body imaging, called EOS (EOS imaging, Paris, France), enables a more comprehensive study, including the lower limbs, with a low dose of radiation.[8]
In addition, new software such as Surgimap (Nemaris, Inc., New York, NY, United States) and SagittalMeter enable the quick and efficient acquisition of the measurements presented below.
The main measurements evaluated on panoramic spinal radiography for the study of sagittal alignment include the following:
-
Sagittal vertical axis (SVA): it is used to locate the position of the head concerning the normal center of gravity. It is a straight line that runs from the center of the vertebral body of C7 to the tip of the superior platform of the sacrum ([Fig. 2]). The SVA can be positive (normal), negative or neutral, depending on where the line runs in relation to S1. A normal SVA measures < 5 cm, and it is associated to the health-related quality of life (HRQOL) index.[1] [7]
-
Sacral slope (SS): it is the angle between the upper platform of S1 and a horizontal line that reaches the highest portion of the sacrum. The average SS is of 40°, ranging from 20° to 65°.[5]
-
Pelvic incidence (PI): it is the angle between a line perpendicular to the center of the sacral platform and a line running from the same point to the center of the femoral head ([Fig. 3]). It measures the inclination at which the sacrum articulates with the pelvis. The average PI is of 51°, ranging from 34° to 84°. The PI usually is fixed in adults, and it does not vary with changes in the patient's position.[1]
-
Pelvic tilt (PT): it is the angle between a vertical line starting at the center of the femoral head and a line from the same point to the center of the platform of S1. This angle describes the rotation of the pelvis regarding the femoral heads ([Fig. 4]). The average PT is of 12°, ranging from 5° to 30°. It displays compensatory changes since it is a postural angle.[5]



The PT is directly related to the PI ([Fig. 5]). A PI increase results in a PT increase, although not proportionally. There is a geometric relationship among all of these angles, and PI is equal to the sum of PT and SS, that is, PI = PT + SS.[1]

To minimize energy consumption, the pelvis tends to align itself with the sacrum that is, its angulation changes to achieve a vertical femoral-sacral line ([Fig. 5]). However, when this line becomes horizontal, pelvic retroversion increases. At this point, the defense mechanisms become insufficient, leading to sagittal malalingment.
A PT increase results in increased pelvic torque, which is the torque of bodyweight mainly at the pelvis and sacrum, and the ground reaction force, applied mainly at the pelvis and acetabulum ([Fig. 6]). Therefore, a higher PT increases compensatory muscle effort to stabilize the pelvis and keep the subject standing straight. Spines with better alignment present smaller PT values (a more vertical femoral line and lower pelvic torque).[3]

-
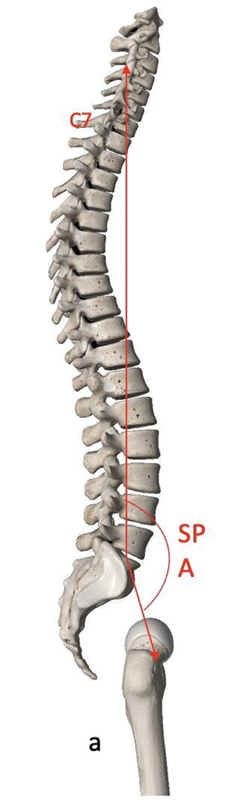
Spinopelvic angle (SPA): it is the angle between a line from the center of the vertebral body of C7 to the center of the superior sacral plate, and a line from that point to the center of the femoral head ([Fig. 7]). The SPA defines the subject's position. Patients with hip flexion present increased SPA, for instance.
-
Spinosacral angle (SSA): it is an angle between a line from the center of the vertebral body of C7 to the center of the superior sacral plateau, and a line running along the surface of the superior sacral plate ([Fig. 8]). The SSA is directly related to the angle of inclination of the sacrum, and it does not vary (it is a fixed angle).[1]

#
Lordosis distribution
Approximately two-thirds of LL occur between L4 and S1. When total lordosis is lost at the expense of the lower lumbar spine, the remaining levels try to compensate by increasing segmental lordosis, which leads to normal LL values. The compensatory defense mechanism leads to a significant pain response.
Roussouly et al.[3] defined four types of sagittal alignment and consequent lordosis distribution. This classification shows the variability and distribution of spinal curves in a subject. These categories help identify some morphological characteristics involved in the pathogenesis of back pain, deformities, and some surgical outcomes. In addition, they improve the understanding of the relationship between sagittal alignment and degenerative changes.[3]
• Sagittal profile variations
There is no single sagittal profile considered normal. In a study with 160 asymptomatic subjects using a three-dimensional model, Roussouly et al.[3] defined four different types ([Fig. 9]):

-
Type-1 lordosis: the transition point in which lordosis changes to kyphosis is at L3-L4, while the apex is at L5. The SS is lower than 35°, and the PI is small. Thoracic kyphosis is long, and lumbar lordosis is short. The ratio between thoracic and lumbar segments is of 80:20.
-
Type-2 lordosis: the transition point is at L1-L2, and the apex is at the base of L4. The SS is lower than 35°, and the PI is small. Thoracic kyphosis is smaller, while lumbar lordosis is greater, with a 60:40 ratio.
-
Type-3 lordosis: the transition is at T12-L1, the SS is between 35° and 45°, and the apex is at the center of L4. The PI is high. The transition point is on the thoracolumbar segment. The kyphosis-to-lordosis ratio is of 50:50, which assumes that the spine is well aligned. It is the most frequent type.
-
Type-4 lordosis: the transition point is at T9-T10. The SS is higher than 45°, the PI is high, and the apex is at the base of L3. Lordosis is greater than dorsal kyphosis, with a 20:80 ratio.
#
#
Pelvic Incidence and Lumbar Lordosis Mismatch
The difference between PI and LL is known as a mismatch. The PI and LL are directly related, and the normal difference between them (PI-LL) is ≤ 10° ([Fig. 10]). There is also a correlation between PI-LL imbalance and the SVA. Its correction is the main goal in the surgical treatment of sagittal malalignment for a harmonious, painless spinopelvic alignment, applicable in both long and short fusions.[9]

#
Treatment
• Conservative treatment
Patients with symptomatic sagittal imbalance respond poorly to the conservative treatment, showing temporary improvement with braces, muscle strengthening due to physical therapy, and/or selective blocks. Although surgery may not be an initial indication, it is the therapeutic goal for these subjects.[5] [10]
#
• Surgical treatment
The indications include failure of the conservative treatment, curvature progression, back pain, progressive neurological deficit, loss of quality of life, and correction of the underlying disease (scoliosis, spondylolisthesis, Scheuermann disease).[11] [12] [13] The goals of surgery are to achieve solid fusion with an aligned spine in the sagittal and coronal planes, relieve pain, and achieve PI-LL < 10°, PT < 25°, and SVA < 5 cm.[7] Several studies have shown that proper restoration of sagittal alignment significantly improves clinical outcomes and prevents adjacent disc disease and further pseudarthrosis.[14] Glassman et al.[15] demonstrated that restoring sagittal alignment as much as possible is the critical goal for any spinal reconstructive surgery.
Since surgeries to correct sagittal imbalance are major procedures, the patient must be carefully assessed preoperatively by a multidisciplinary team to reduce risks, such as those of pseudarthrosis, implant loosening, infection, neurological damage, and excessive bleeding.[15] [16] [17] [18] [19] [20] Studies show a 24% prevalence of pseudarthrosis after long instrumentation with fusion up to S1.[20]
The measurement of spinopelvic parameters is essential in preoperative planning. Bridwell et al.[19] classified the deformities into three categories based on curve flexibility: fully flexible, partially flexible with movable segments, and fixed deformity with no correction in recumbency.
Spine flexibility must be evaluated radiologically due to the presence of mobile segments. Anteroposterior and lateral panoramic radiographs and lateral flexion and extension radiographs may demonstrate the flexibility of the deformity.[18]
It is suggested that flexible deformities can be corrected both anteriorly and posteriorly with no need for three-column osteotomies, such as pedicle subtraction osteotomy (PSO) or vertebral column resection (VCR).[19] The improvement in sagittal alignment is due to correction and elongation of the anterior column, through a structural allograft, a structural autograft, or interbody cages.
Rigid deformities are corrected by anterior, a combination of anterior and posterior, or posterior surgery. Techniques to perform three-column osteotomies (PSO, VCR) are also used, aiming at posterior shortening as a basis for correction.
Currently, the levels of complication from the correction of vertebral deformities in adults have been progressively decreasing due to the knowledge acquired over the last decades. All techniques have excellent short- and long-term outcomes thanks to the continuous development and advent of minimally-invasive surgical techniques.[19]
#
Final Considerations
Body imbalance in the sagittal plane is a spinal misalignment with several etiologies, including congenital, degenerative, iatrogenic, and traumatic disorders. Initially, it can be tolerated by the patient, but the exhaustion of defense mechanisms results in pain, functional loss, and worsening of quality of life. Panoramic radiography is the study of choice to perform all pertinent measurements (SVA, PT, PI, SS, SSA, SPA). Currently, there are several techniques for the surgical treatment, and the choice of the most appropriate approach depends on the degree of deformity and the affected levels. An anterior, a combination of anterior and posterior, or a combined approach can be used, with or without osteotomies.
Understanding the concepts involved in vertebral alignment and its implications are critical to assess a patient with deformity both in the coronal and sagittal planes. General orthopedists must know how to recognize a patient with deformity and sagittal imbalance for an appropriate referral to specialists. Spine surgeons must have this knowledge consolidated for correct preoperative planning to avoid unsatisfactory outcomes resulting in pain and loss of quality of life.
#
#
#
Financial Support
There was no financial support from public, commercial, or non-profit sources.
-
Referências
- 1 Schwab F, Lafage V, Patel A, Farcy JP. Considerações sobre o plano sagital e a pelve no paciente adulto. Spine (Phila Pa 1976) 2009; 34 (17) 1828-1833
- 2 Hardacker JW, Shuford RF, Capicotto PN, Pryor PW. Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine (Phila Pa 1976) 1997; 22 (13) 1472-1480
- 3 Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 2005; 30 (03) 346-353
- 4 Aoki Y, Nakajima A, Takahashi H. et al. Influence of pelvic incidence-lumbar lordosis mismatch on surgical outcomes of short-segment transforaminal lumbar interbody fusion. BMC Musculoskelet Disord 2015; 16: 213
- 5 Bradford DS, Tay BK, Hu SS. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine (Phila Pa 1976) 1999; 24 (24) 2617-2629
- 6 Savarese LG, Menezes-Reis R, Bonugli GP, Herrero CFPDS, Defino HLA, Nogueira-Barbosa MH. Spinopelvic sagittal balance: what does the radiologist need to know?. Radiol Bras 2020; 53 (03) 175-184
- 7 Le Huec JC, Roussouly P. Sagittal spino-pelvic balance is a crucial analysis for normal and degenerative spine. Eur Spine J 2011; 20 Suppl 5(Suppl 5): 556-557
- 8 Van Royen BJ, Toussaint HM, Kingma I. et al. Accuracy of the sagittal vertical axis in a standing lateral radiograph as a measurement of balance in spinal deformities. Eur Spine J 1998; 7 (05) 408-412
- 9 Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine (Phila Pa 1976) 1999; 24 (16) 1712-1720
- 10 Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am 2003; 85 (03) 454-463
- 11 Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: prevalence and risk factor analysis of 144 cases. Spine (Phila Pa 1976) 2006; 31 (20) 2329-2336
- 12 Dorward IG, Lenke LG. Osteotomies in the posterior-only treatment of complex adult spinal deformity: a comparative review. Neurosurg Focus 2010; 28 (03) E4
- 13 Tebet MA. Current concepts on the sagittal balance and classification ofspondylolysis and spondylolisthesis. Rev Bras Ortop 2014; 49 (01) 3-12
- 14 Hu SS, Berven SH. Preparing the adult deformity patient for spinal surgery. Spine (Phila Pa 1976) 2006; 31 (19) , Suppl) S126-S131
- 15 Glassman SD, Berven S, Bridwell K, Horton W, Dimar JR. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976) 2005; 30 (06) 682-688
- 16 Bridwell KH. Decision making regarding Smith-Petersen vs. pedicle subtraction osteotomy vs. vertebral column resection for spinal deformity. Spine (Phila Pa 1976) 2006; 31 (19) , Suppl) S171-S178
- 17 Pateder DB, Kebaish KM, Cascio BM, Neubaeur P, Matusz DM, Kostuik JP. Posterior only versus combined anterior and posterior approaches to lumbar scoliosis in adults: a radiographic analysis. Spine (Phila Pa 1976) 2007; 32 (14) 1551-1554
- 18 Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine (Phila Pa 1976) 2009; 34 (17) E599-E606
- 19 Bridwell KH, Lenke LG, Lewis SJ. Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop Relat Res 2001; (384) 35-44
- 20 Haid RW, Shaffrey CI, Youssef JA, Schwab FJ. Global Spine Alignment: Principles, pathologies and Procedures. St. Louis, Missouri: Quality Medical Publishing; 2015
Endereço para correspondência
Publication History
Received: 20 December 2020
Accepted: 22 November 2021
Article published online:
11 March 2022
© 2022. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Schwab F, Lafage V, Patel A, Farcy JP. Considerações sobre o plano sagital e a pelve no paciente adulto. Spine (Phila Pa 1976) 2009; 34 (17) 1828-1833
- 2 Hardacker JW, Shuford RF, Capicotto PN, Pryor PW. Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine (Phila Pa 1976) 1997; 22 (13) 1472-1480
- 3 Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 2005; 30 (03) 346-353
- 4 Aoki Y, Nakajima A, Takahashi H. et al. Influence of pelvic incidence-lumbar lordosis mismatch on surgical outcomes of short-segment transforaminal lumbar interbody fusion. BMC Musculoskelet Disord 2015; 16: 213
- 5 Bradford DS, Tay BK, Hu SS. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine (Phila Pa 1976) 1999; 24 (24) 2617-2629
- 6 Savarese LG, Menezes-Reis R, Bonugli GP, Herrero CFPDS, Defino HLA, Nogueira-Barbosa MH. Spinopelvic sagittal balance: what does the radiologist need to know?. Radiol Bras 2020; 53 (03) 175-184
- 7 Le Huec JC, Roussouly P. Sagittal spino-pelvic balance is a crucial analysis for normal and degenerative spine. Eur Spine J 2011; 20 Suppl 5(Suppl 5): 556-557
- 8 Van Royen BJ, Toussaint HM, Kingma I. et al. Accuracy of the sagittal vertical axis in a standing lateral radiograph as a measurement of balance in spinal deformities. Eur Spine J 1998; 7 (05) 408-412
- 9 Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine (Phila Pa 1976) 1999; 24 (16) 1712-1720
- 10 Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am 2003; 85 (03) 454-463
- 11 Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: prevalence and risk factor analysis of 144 cases. Spine (Phila Pa 1976) 2006; 31 (20) 2329-2336
- 12 Dorward IG, Lenke LG. Osteotomies in the posterior-only treatment of complex adult spinal deformity: a comparative review. Neurosurg Focus 2010; 28 (03) E4
- 13 Tebet MA. Current concepts on the sagittal balance and classification ofspondylolysis and spondylolisthesis. Rev Bras Ortop 2014; 49 (01) 3-12
- 14 Hu SS, Berven SH. Preparing the adult deformity patient for spinal surgery. Spine (Phila Pa 1976) 2006; 31 (19) , Suppl) S126-S131
- 15 Glassman SD, Berven S, Bridwell K, Horton W, Dimar JR. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976) 2005; 30 (06) 682-688
- 16 Bridwell KH. Decision making regarding Smith-Petersen vs. pedicle subtraction osteotomy vs. vertebral column resection for spinal deformity. Spine (Phila Pa 1976) 2006; 31 (19) , Suppl) S171-S178
- 17 Pateder DB, Kebaish KM, Cascio BM, Neubaeur P, Matusz DM, Kostuik JP. Posterior only versus combined anterior and posterior approaches to lumbar scoliosis in adults: a radiographic analysis. Spine (Phila Pa 1976) 2007; 32 (14) 1551-1554
- 18 Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine (Phila Pa 1976) 2009; 34 (17) E599-E606
- 19 Bridwell KH, Lenke LG, Lewis SJ. Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop Relat Res 2001; (384) 35-44
- 20 Haid RW, Shaffrey CI, Youssef JA, Schwab FJ. Global Spine Alignment: Principles, pathologies and Procedures. St. Louis, Missouri: Quality Medical Publishing; 2015









