
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1743499
Closure of Transsplenic Access Tracts Using Tract Embolics: Success, Clinical Outcomes, and Complications in a Tertiary Center


Abstract
Purpose The aim of the study was to evaluate the safety and effectiveness of transsplenic venous access closure.
Materials and Methods Twenty patients (mean age: 51.8 years; range: 28–72), underwent 21 transsplenic venous access procedures over 4 years in this retrospective study. Comorbidities, active hemorrhage, anticoagulation, coagulation parameters, platelets, indications for transsplenic access, needle gauge, sheath size, variceal embolization method, tract embolization method, bleeding complications, and transfusion requirements and additional procedures to manage bleeding complications were recorded.
Results Preprocedure comorbidities included portal hypertension (n = 18/20, 90%), portal vein thrombosis (n = 14/20, 70%), hemorrhage (n = 6/20, 30%), splenic vein thrombosis (n = 7/20, 35%), anticoagulation (n = 2/20, 10%), and sinistral portal hypertension (n = 2/20,10%). Mean baseline international normalized ratio was 1.3 (range: 1–1.9), platelets 122 (range: 18–492). Most common transsplenic access indications were gastric varices with nonpatent portosystemic shunt (n = 11/21, 52%) and portal vein targeting for transjugular intrahepatic portosystemic shunt (n = 8, 38%). Most common access sheath sizes were 4-French (n = 5, 24%) and 6-French (n = 6, 29%). Fifteen procedures (71%) involved variceal embolization. Transsplenic tracts were embolized with microfibrillar collagen alone (n = 7), coils and microfibrillar collagen (n = 8), or others (n = 6). Based on the Society of Interventional Radiology adverse event classification system, embolization complications included one major (splenic artery pseudoaneurysm and a splenic vein pseudoaneurysm) and three moderate (19%) adverse bleeding events, which required blood transfusion.
Conclusion Transsplenic venous access tract embolization is a safe and moderately effective method to achieve tract hemostasis, with an overall clinical failure rate of 20%.
#
Introduction
Percutaneous transsplenic venous access (PTSVA) is an effective and safe method to gain entry to the portal venous system when transjugular, transhepatic, and percutaneous transhepatic access routes are not optimal.[1] [2] [3] This approach has been used for diagnostic splenoportography, variceal embolization, portal vein recanalization, and to facilitate portal venous cannulation for transjugular intrahepatic portosystemic shunt (TIPS). Access site hemostasis is an important consideration of PTSVA.[4] However, multiple prior studies have shown no difference between transsplenic and transhepatic access site hemorrhagic complications.[5] [6] Historically, rates of PTSVA tract hemorrhage were significantly higher without the use of embolic materials to plug the splenic tract.[7] [8] To date, splenic parenchymal tract closure has been reported successfully with a low complication rate utilizing a variety of embolics, including plugs, Gelfoam, and a combination of coils and glue.[1] [9] In this retrospective study, we aim to assess the efficacy of splenic parenchymal tract closure with microfibrillar collagen (Avitene microfibrillar collagen hemostat; Warwick, Rhode Island, United States) alone, and in conjunction with a variety of other embolics, for closure of transsplenic access tracts.
#
Materials and Methods
A single-center retrospective review of the electronic medical records was conducted of all patients who underwent PTSVA with tract embolization from August 2014 to August 2018 with the approval of the institutional review board. In all, 23 patients were considered for inclusion. One 18-month-old patient was excluded, one was excluded for insufficient data, and one excluded due to inability to establish secure transsplenic venous access. The analyzed cohort consisted of 21 PTSVA performed in 20 patients (11 male, 9 female; median age: 55), with one patient undergoing two procedures. All but one patient underwent cross-sectional imaging with computed tomographic (CT) or magnetic resonance imaging prior to intervention. All patients were followed for access site complications for a minimum of 45 days unless they died prior to this time (n = 2), except for one patient who was lost to follow-up at 2 weeks.
Technical success of PTSVA tract closure was defined by stability of the tract embolic between immediate and 1-minute delayed fluoroscopic imaging relative to PTSVA tract embolization. Clinical success was defined as the absence of high-density ascites (on CT), or perisplenic hematoma on post-procedural ultrasound or CT performed for the evaluation of postprocedural abdominal pain, hypotension or hemoglobin drop. Clinical failures were graded on the basis of the most recent Society of Interventional Radiology (SIR) adverse event classification system.[10]
Procedural Technique
An attending interventional radiologist saw each patient in the clinic or during inpatient consultation before the procedure. Procedures were performed with moderate sedation with intravenous midazolam and fentanyl or general anesthesia administered by a certified registered nurse anesthetist or anesthesiologist. Patients were resuscitated for ongoing hemorrhage and coagulopathy by anesthesia staff throughout the procedure when necessary. Paracentesis was performed in cases with large volume ascites prior to performing PTSVA.
Available preprocedural cross-sectional imaging was reviewed to determine the optimal site for PTSVA. Access was preferentially targeted to inferior splenic vasculature when feasible to minimize the risk of pleural transgression. All patients were administered local analgesia percutaneously to the level of the splenic capsule with 1% lidocaine. Percutaneous access was performed with a 21 or 22-gauge Chiba needle (Cook Medical; Bloomington, Indiana, United States) under sonographic guidance. Angiography was then performed to confirm appropriate access. This was followed by splenic vein cannulation with a 0.018” wire except for one case (Patient #1) that was performed through the 22G access, which was sufficient for Gelfoam embolization of gastric varices. Transitional dilatation was performed in all other cases to sheath sizes ranging from 4 to 8 French. The most common procedures subsequently performed were TIPS with portal venous recanalization (n = 8), antegrade gastric variceal embolization (n = 7), and antegrade gastroesophageal embolization (n = 5), as previously described.[11] [12]
For access closure, transsplenic angiography was performed during retraction of the PTSVA sheath to identify the point of splenic venous entry. Tract embolization was then performed under continuous fluoroscopic imaging to the level of the splenic capsule. PTSVA tracts were embolized through the largest placed access sheath with one or a combination of embolics, including Gelfoam, microfibrillar collagen, coils, and n-butyl cyanoacrylate (NBCA). Gelfoam and microfibrillar collagen embolic suspensions were prepared as a slurry with iodinated contrast material. NBCA was mixed with lipiodol when utilized. Mixture ratios were determined by operator preference.
#
Statistical Analyses
Patient characteristics assessed for statistical significance with respect to PTSVA tract hemorrhage included age, international normalized ratio (INR), platelets, PTSVA sheath size (data not available for one patient, and one case was performed with PTSVA through a 22G Chiba needle), preprocedural active hemorrhage, and preprocedural or intraprocedural active anticoagulation (referred to as active anticoagulation). PTSVA tract embolic selection was also assessed for statistical significance with respect to hemorrhage in the following categories: microfibrillar collagen, microfibrillar collagen combined with other embolics, and single or multiple embolics other than microfibrillar collagen. Significance of hemorrhage could not be ascertained on the basis of pre- and postprocedural hemoglobin changes due to a lack of standardization of hemoglobin measurements related to procedural timing and transfusion requirements.
IBM SPSS Statistics for Windows, Version 24.0. (IBM Corporation, Armonk, New York, United States) was used to perform the statistical analysis. Means, standard deviations, Welch's t-tests, Fisher's exact test, and chi-squared analysis were performed for PTSVA tract bleed complications ([Tables 1] and [2]). A 5% level of significance was used.
Abbreviations: INR, international normalized ratio; PTSVA, percutaneous transsplenic venous access.
Abbreviation: PTSVA, percutaneous transsplenic venous access.
Descriptive statistics were performed for the following variables: procedural indications, procedures performed, indications for PTSVA, portal venous hypertension, variceal embolization methods, PTSVA tract embolics, postprocedural transfusion requirements, procedures required to treat PTSVA tract hemorrhage, and adverse bleeding event severity defined by SIR criteria.[10]
#
#
Results
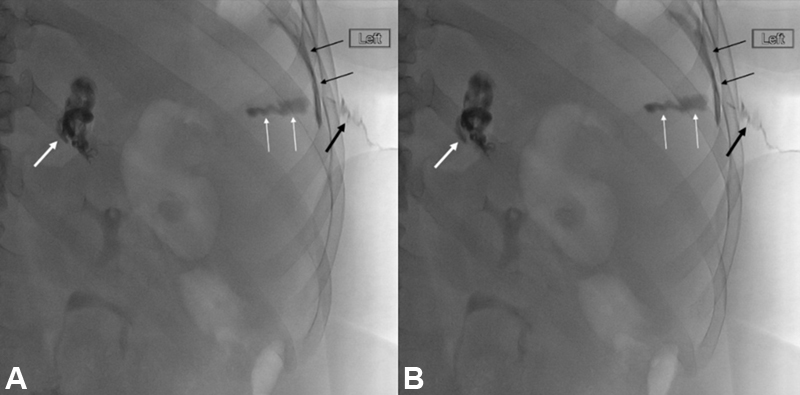
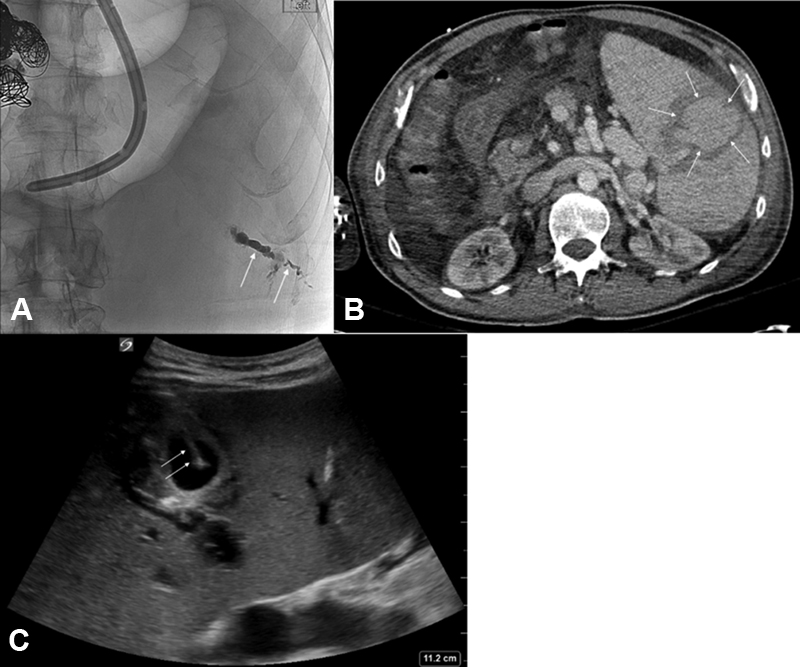
Technical success of PTSVA tract embolization was achieved in 9 of 10 cases that were able to be assessed due to absent or insufficient imaging in the remaining 11 cases, rendering this component of the study as descriptive. [Fig. 1] demonstrates an example of a technically successful case. One technical failure—characterized by partial migration of tract embolic following PTSVA tract embolization—was not associated with clinical failure. Clinical success was achieved in 17/21 cases (81%). Four cases were complicated by PTSVA access site hemorrhage in which three cases were moderate and one was severe as per SIR classification. Mean follow-up time was 9.3 months,(median being 5 months; range: 0.25–25.5 months). There were no postprocedural access site bleeds that developed beyond 30 days. Three of four perisplenic hemorrhages presented on the same day of the procedure or postprocedure day (PPD) 1 and were stabilized by PPD 1 or 2. One PTSVA tract hemorrhagic complication was found incidentally on PPD 2 and stabilized by PPD 31 ([Fig. 2]).
Procedural indications, procedures performed, and indications for PTSVA are shown in [Table 3]. Patient age, INR, platelets, PTSVA sheath size, preprocedural active hemorrhage, presence or absence of active anticoagulation, and PTSVA tract embolics are also shown in [Table 3]. Portal venous hypertension was present in all patients. Portal venous thrombosis was present in 14 cases. Splenic vein thrombosis was present in 7 cases. Variceal embolization was performed in 15 cases with one, or a combination of Gelfoam, coils, NBCA, and/or vascular plug. Number of postprocedural packed red blood cell transfusion requirements, interventions required for management of PTSVA tract hemorrhage, and adverse event category by SIR criteria are listed for all cases complicated by PTSVA tract hemorrhages in [Table 4].
Abbreviations: EV, esophageal varices/variceal; GOV, gastroesophageal varices/variceal; GV, gastric varices/variceal; HE, hepatic encephalopathy; MV, mesenteric varices; NBCA, n-butyl cyanoacrylate; PSS, portosystemic shunt; PsV, peristomal varices/variceal; PTSVA, percutaneous transsplenic venous access; PVR, portal venous recanalization; PVT, portal vein thrombosis; PV, portal venography; RV, rectal varices/variceal; Spl VT, splenic venous thrombosis; SPM, spleno-porto-mesenteric; TIPS, transjugular intrahepatic portosystemic shunt; Ts LB, transsplenic liver biopsy.
|
Patient number |
Postprocedural PRBC transfusion requirement |
Additional interventions |
AE category by SIR criteria |
|---|---|---|---|
|
5 |
2 |
None |
Moderate AE |
|
7 |
2 |
None |
Moderate AE |
|
13 |
2 |
None |
Moderate AE |
|
20 |
2 |
Splenic venous pseudoaneurysm thrombin injection on PPD 12. Splenic arterial pseudoaneurysm embolization on PPD 21. Laparotomy and washout on PPD 31 |
Severe AE |
Abbreviations: AE, adverse event; PRBC, packed red blood cell; PPD, postprocedure day; SIR, Society of Interventional Radiology.
Means, standard deviations, and p-values with respect to the distribution of patient age and INR, platelets, and PTSVA sheath size with respect to presence or absence of PTSVA tract bleeding complications are shown in [Table 1]. Distribution of cases involving active hemorrhage, active anticoagulation, and PTSVA tract embolics with respect to the presence or absence of PTSVA tract bleeding complications and associated p-values is shown in [Table 2]. Mean platelet values for patients who did and did not suffer PTSVA tract hemorrhage were 58.5 and 135 (1000/mm^3), respectively, which were statistically significant (p = 0.032). Mean ages for patients who did and did not suffer PTSVA tract hemorrhage were 59.8 and 49.8 (years), respectively, which were also significantly different (p = 0.044). There was no statistically significant difference between risk of PTSVA tract hemorrhage corresponding to INR (p = 0.730), active anticoagulation (p = 1), active hemorrhage (p = 0.694), PTSVA sheath size (p = 0.814), or PTSVA tract embolics (p = 0.921).
#
Discussion
PTSVA is a valuable technique to gain antegrade access to the portal venous system in a minority of portal venous interventions. The technique has been shown to be useful in the setting of portal venous thrombosis requiring main portal venous recanalization, variceal embolization, accurate measurements of extrahepatic portal hypertension, and antegrade portography to visualize portal venous collateral pathways.[9] [13] [14] PTSVA is also useful to access bleeding gastric varices that are not associated with a patent gastrorenal shunt.[12] [15] This study also finds PTSVA to be useful in circumstances similar to those reported in the literature ([Table 3]).
Haddad et al validated the safety of transsplenic access in 2018 by comparison of patient cohorts undergoing transsplenic and transhepatic accesses from 2000 to 2017 at their institution. They report 3 bleeding complications out of 24 transsplenic accesses (12.5%), and 10 bleeding complications out of 124 transhepatic accesses (8.1%), which were not significantly different when stratified to overall and major bleeding complications.[5] Multiple authors have demonstrated a similar rate of bleeding complications. Liang et al reported 2 bleeding complications out of 17 cases of transsplenic access (12.5%).[3] Zhu et al reported 3 major and 6 minor bleeding complications out of 44 transsplenic accesses (6.5 and 13%, respectively).[13] Monroe et al reported 2 bleeding complications out of 26 cases (7.7%).[9] As such, the bleeding complication rate in this study is comparable to the reported literature for transsplenic access. We report a 19% complication rate with respect to bleeding following PTSVA tract embolization (4 bleeding events). Three patients adequately responded to transfusions of two units of packed red blood cells qualifying the severity of their complications as moderate adverse events by SIR criteria (14.3%). One patient experienced a major adverse event related to bleeding (4.8%). He required two procedures to treat splenic venous and arterial pseudoaneurysms, respectively, and an operation to evacuate a painful intraperitoneal hematoma ([Fig. 2]).
Transsplenic access tract embolization is a commonly reported technique to lower the risk of tract hemorrhage.[3] [5] [9] [13] Commonly reported embolics, including Gelfoam, coils, coils and glue, and vascular plugs, have demonstrated acceptable performance in this regard.[1] [2] [12] [15] [16] This study demonstrates that low-cost microfibrillar collagen confers no greater risk of PTSVA tract hemorrhage compared to Gelfoam, NBCA or coils when used alone or in combination with one of these agents (p = 0.977). Pimpalwar et al demonstrated a relatively higher rate of transsplenic access tract hemorrhage of 27% in a pediatric cohort embolized with Gelfoam pledgets or microfibrillar collagen, but this study did not make a comparison of different embolic agents with respect to tract hemorrhage. Interestingly, the authors of that study report limited success with microfibrillar collagen, which they discontinued early in the course of their work due to clogging of microfibrillar collagen-contrast slurry in the 4 French dilators they used to deploy the embolic.[14] In this study, PTSVA tract embolization was performed in 17 cases without experiencing delivery system occlusion. At the authors' institution, microfibrillar collagen is routinely used for closure of both transhepatic and transsplenic access tracts. Benefits of this agent include the low cost, ease of use, and lack of permanent artifact on future CT imaging associated with coils and NBCA tract closure.
We detected a significant difference in preprocedural mean platelet levels between patients who did and did not experience a PTSVA tract hemorrhage following tract embolization ([Table 4]). The cohort of patients who experienced PTSVA tract hemorrhage demonstrated a mean platelet level of 58,000 plt/mm^3, which is higher than the cutoff of 50,000 plt/ mm^3 recommended by the SIR anticoagulation guidelines for procedures with significant bleeding risk.[17] The increased rate of bleeding may have been due to concomitant bleeding risk factors that were not independently associated with higher PTSVA tract bleeding in our study, likely due to our small patient population. Zhu et al reported a higher prevalence of transsplenic access hemorrhage in a 46-patient series among patients with moderately elevated INR in the range of 1.51 to 1.64.[13] However, we did not detect INR to be a significant risk factor for PTSVA tract bleeding, possibly also due to the small size of our population.
Additionally, we found age to be a significant risk factor for prediction of PTSVA tract hemorrhage in our cohort, which has not been previously reported in the literature. The loss of physiologic reserve associated with advancing age may correlate with multiple risk factors for tract bleeding.
This study is limited by its retrospective uncontrolled design. No differences were detected in clinical outcomes on the basis of chosen PTSVA tract embolic; however, a lack of post-procedural imaging in many cases may have resulted in underreporting of clinically insignificant mild adverse events with respect to PTSVA tract bleeding. Furthermore, a lack of standardized ratios of Gelfoam and microfibrillar mixture with iodinated contrast material, and NBCA mixture with ethiodized oil limited our development of a given protocol by which liquid embolics may be used with equal efficacy for PTSVA tract embolization. Furthermore, our small population size imposed several limits to our statistical analysis. The technical success of PTSVA tract embolization was observed in 9/10 cases that could be assessed, with the other 11 having absent/insufficient imaging, making that part of the study descriptive. This, in addition to a lack of a controlled design, accounts for the confinement of our studied tract embolics to broad categories apart from microfibrillar collagen. Our small patient sample size may also explain why we were unable to identify expected risk factors as significantly predictive of PTSVA tract hemorrhages.
#
Conclusion
PTSVA is an important adjunctive technique for common portal venous interventions, particularly those complicated by portal venous occlusion. Within the limitations of our study, we have demonstrated that embolization of transsplenic venous access tract is safe and effective.
#
#
Conflict of Interest
None declared.
Ethical approval
The article was exempted from an ethical committee approval.
-
References
- 1 Chu HH, Kim HC, Jae HJ. et al. Percutaneous transsplenic access to the portal vein for management of vascular complication in patients with chronic liver disease. Cardiovasc Intervent Radiol 2012; 35 (06) 1388-1395
- 2 Habib A, Desai K, Hickey R. et al. Portal vein recanalization-transjugular intrahepatic portosystemic shunt using the transsplenic approach to achieve transplant candidacy in patients with chronic portal vein thrombosis. J Vasc Interv Radiol 2015; 26 (04) 499-506
- 3 Liang HL, Yang CF, Pan HB, Chen CK, Chang JM. Percutaneous transsplenic catheterization of the portal venous system. Acta Radiol 1997; 38 (02) 292-295
- 4 Quinn SF, vanSonnenberg E, Casola G, Wittich GR, Neff CC. Interventional radiology in the spleen. Radiology 1986; 161 (02) 289-291
- 5 Haddad MM, Fleming CJ, Thompson SM. et al. Comparison of bleeding complications between transsplenic versus transhepatic access of the portal venous system. J Vasc Interv Radiol 2018; 29 (10) 1383-1391
- 6 Ohm J-Y, Ko G-Y, Sung K-B, Gwon D-I, Ko HK. Safety and efficacy of transhepatic and transsplenic access for endovascular management of portal vein complications after liver transplantation. Liver Transpl 2017; 23 (09) 1133-1142
- 7 Brazzini A, Hunter DW, Darcy MD. et al. Safe splenoportography. Radiology 1987; 162 (03) 607-609
- 8 Probst P, Rysavy JA, Amplatz K. Improved safety of splenoportography by plugging of the needle tract. AJR Am J Roentgenol 1978; 131 (03) 445-449
- 9 Monroe EJ, Speir EJ, Hawkins CM, Shivaram G, Koo KSH, Gill AE. Transsplenic splenoportography and portal venous interventions in pediatric patients. Pediatr Radiol 2018; 48 (10) 1441-1450
- 10 Khalilzadeh O, Baerlocher MO, Shyn PB. et al. Proposal of a new adverse event classification by the Society of Interventional Radiology Standards of Practice Committee. J Vasc Interv Radiol 2017; 28 (10) 1432-1437.e3
- 11 Thornburg B, Desai K, Hickey R. et al. Portal vein recanalization and transjugular intrahepatic portosystemic shunt creation for chronic portal vein thrombosis: technical considerations. Tech Vasc Interv Radiol 2016; 19 (01) 52-60
- 12 Gong GQ, Wang XL, Wang JH. et al. Percutaneous transsplenic embolization of esophageal and gastrio-fundal varices in 18 patients. World J Gastroenterol 2001; 7 (06) 880-883
- 13 Zhu K, Meng X, Zhou B. et al. Percutaneous transsplenic portal vein catheterization: technical procedures, safety, and clinical applications. J Vasc Interv Radiol 2013; 24 (04) 518-527
- 14 Pimpalwar S, Chinnadurai P, Hernandez A, Kukreja K, Siddiqui S, Justino H. Trans-splenic access for portal venous interventions in children: do benefits outweigh risks?. Cardiovasc Intervent Radiol 2018; 41 (01) 87-95
- 15 Grosse U, Brechtel K, Ketelsen D. et al. Portal vein recanalization and embolization of the transsplenic puncture tract using an Amplatzer® vascular plug: a case report. BMC Res Notes 2015; 8: 193
- 16 Uller W, Müller-Wille R, Grothues D. et al. Gelfoam for closure of large percutaneous transhepatic and transsplenic puncture tracts in pediatric patients. Röfo Fortschr Geb Röntgenstr Nuklearmed 2014; 186 (07) 693-697
- 17 Patel IJ, Rahim S, Davidson JC. et al. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions-Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J Vasc Interv Radiol 2019; 30 (08) 1168-1184.e1
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
08. März 2022
© 2022. Indian Society of Vascular and Interventional Radiology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Chu HH, Kim HC, Jae HJ. et al. Percutaneous transsplenic access to the portal vein for management of vascular complication in patients with chronic liver disease. Cardiovasc Intervent Radiol 2012; 35 (06) 1388-1395
- 2 Habib A, Desai K, Hickey R. et al. Portal vein recanalization-transjugular intrahepatic portosystemic shunt using the transsplenic approach to achieve transplant candidacy in patients with chronic portal vein thrombosis. J Vasc Interv Radiol 2015; 26 (04) 499-506
- 3 Liang HL, Yang CF, Pan HB, Chen CK, Chang JM. Percutaneous transsplenic catheterization of the portal venous system. Acta Radiol 1997; 38 (02) 292-295
- 4 Quinn SF, vanSonnenberg E, Casola G, Wittich GR, Neff CC. Interventional radiology in the spleen. Radiology 1986; 161 (02) 289-291
- 5 Haddad MM, Fleming CJ, Thompson SM. et al. Comparison of bleeding complications between transsplenic versus transhepatic access of the portal venous system. J Vasc Interv Radiol 2018; 29 (10) 1383-1391
- 6 Ohm J-Y, Ko G-Y, Sung K-B, Gwon D-I, Ko HK. Safety and efficacy of transhepatic and transsplenic access for endovascular management of portal vein complications after liver transplantation. Liver Transpl 2017; 23 (09) 1133-1142
- 7 Brazzini A, Hunter DW, Darcy MD. et al. Safe splenoportography. Radiology 1987; 162 (03) 607-609
- 8 Probst P, Rysavy JA, Amplatz K. Improved safety of splenoportography by plugging of the needle tract. AJR Am J Roentgenol 1978; 131 (03) 445-449
- 9 Monroe EJ, Speir EJ, Hawkins CM, Shivaram G, Koo KSH, Gill AE. Transsplenic splenoportography and portal venous interventions in pediatric patients. Pediatr Radiol 2018; 48 (10) 1441-1450
- 10 Khalilzadeh O, Baerlocher MO, Shyn PB. et al. Proposal of a new adverse event classification by the Society of Interventional Radiology Standards of Practice Committee. J Vasc Interv Radiol 2017; 28 (10) 1432-1437.e3
- 11 Thornburg B, Desai K, Hickey R. et al. Portal vein recanalization and transjugular intrahepatic portosystemic shunt creation for chronic portal vein thrombosis: technical considerations. Tech Vasc Interv Radiol 2016; 19 (01) 52-60
- 12 Gong GQ, Wang XL, Wang JH. et al. Percutaneous transsplenic embolization of esophageal and gastrio-fundal varices in 18 patients. World J Gastroenterol 2001; 7 (06) 880-883
- 13 Zhu K, Meng X, Zhou B. et al. Percutaneous transsplenic portal vein catheterization: technical procedures, safety, and clinical applications. J Vasc Interv Radiol 2013; 24 (04) 518-527
- 14 Pimpalwar S, Chinnadurai P, Hernandez A, Kukreja K, Siddiqui S, Justino H. Trans-splenic access for portal venous interventions in children: do benefits outweigh risks?. Cardiovasc Intervent Radiol 2018; 41 (01) 87-95
- 15 Grosse U, Brechtel K, Ketelsen D. et al. Portal vein recanalization and embolization of the transsplenic puncture tract using an Amplatzer® vascular plug: a case report. BMC Res Notes 2015; 8: 193
- 16 Uller W, Müller-Wille R, Grothues D. et al. Gelfoam for closure of large percutaneous transhepatic and transsplenic puncture tracts in pediatric patients. Röfo Fortschr Geb Röntgenstr Nuklearmed 2014; 186 (07) 693-697
- 17 Patel IJ, Rahim S, Davidson JC. et al. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions-Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J Vasc Interv Radiol 2019; 30 (08) 1168-1184.e1