Keywords
abscess - antibacterial drug resistance - child - neck
Introduction
Neck abscesses are very common in children and can be severe if deep neck spaces are
involved.[1] They may be potentially life-threatening with significant morbidity and mortality
in children, especially in those with vague presentations and when physical examinations
are difficult.[2]
Anatomically, the deep neck spaces are classified into three groups based on the relationship
with the hyoid bone: spaces localized above the hyoid level (peritonsillar, submental,
submandibular, parapharyngeal, buccal, parotid, masticatory/temporal, buccal, parotid);
spaces that involve the entire circumference of the neck (retropharyngeal, danger
space, prevertebral, and carotid); and the anterior or pretracheal visceral space,
below the hyoid bone.[3]
Early diagnosis, appropriate antibiotic coverage, and drainage of collection play
a key role in management.[4] Antibiotic resistance pattern in pediatric deep neck space infection current evidence
recommends either medical treatment using antibiotics or surgical treatment guided
by patient factors such as age, disease site.[5] Because it is a polymicrobial disease, empirical antibiotics play a critical role
in alleviating the clinical course of neck abscess while awaiting culture report.
However, culture-guided antimicrobial therapy is the best clinical practice.[6]
The present study aimed to review the microbiology, antibiotic sensitivity, and resistance
pattern of deep neck abscess. In addition, the outcome of management, including complication
and recurrence rate, was also assessed.
Materials and Methods
Study Population and Method
A prospective study of pediatric patients admitted for management of neck space infection
at the department of ENT and head and neck surgery was performed for 1 year from August
2017 to August 2018. The age, gender, symptoms and signs, organisms isolated with
their sensitivity and resistance to antibiotics, the duration of abscess resolution,
length of hospital stay, complications, and recurrence were noted. The outcomes, including
complications, abscess resolution, and the length of hospitalization, were observed
in the group managed exclusively with medical treatment as well as in the other group,
managed with combined medical treatment and surgical intervention.
Patients presenting infection of both suprahyoid and infrahyoid spaces, such as submental,
submandibular, peritonsillar, parotid, parapharyngeal, retropharyngeal spaces and
anteroposterior triangle were included. Children with preexisting cyst with secondary
infection, proven case of tubercular abscess, and abscesses secondary to otologic
or orbital complications, were excluded. Any comorbidity predisposing to neck abscess
was noted. All patients had empirical intravenous ampicillin and cloxacillin. Intravenous
metronidazole was added in selected cases, depending on the clinical improvement.
In addition to complete blood count, appropriate imaging of the affected site was
done. The aspiration was done under ultrasonic guidance in the majority of the cases,
except for peritonsillar and retropharyngeal abscess. Due to cost and time constraints,
the abscess was drained without general anesthesia in the ward; however, adequate
analgesia was provided. The abscess was drained under general anesthesia (GA) in cases
of parapharyngeal abscess, necrotizing fasciitis, and cases with negative aspiration
but needing urgent surgical intervention based on the clinical and radiological judgment
in spite of negative aspirate. Cases of pus on aspiration indicating abscess and those
requiring urgent attention underwent surgical drainage (incision and drainage [I&D]).
Pus either aspirated or drained was sent for culture and sensitivity. Patients with
no pus on aspiration on USG guidance and minimal collection on ultrasound were medically
managed. The patients were discharged with oral medications after improvement in the
clinical symptoms, like fever, dysphagia, pain, and the laboratory parameters. Patients
were discharged with oral antibiotics provided they showed improvement clinically
and no further collection on either repeat ultrasound or computed tomography (CT)
scan.
Role of Imaging
Ultrasonography was performed in all cases as the first-line investigation, except
in cases of peritonsillar abscess and retropharyngeal space. A contrast-enhanced CT
scan was performed in selected cases of parapharyngeal and retropharyngeal abscess
as well as in cases with life-threatening complications and those in which ultrasonography
(USG) did not yield enough information.
Statistical Analysis
Statistical analysis was performed using the IBM SPSS Statistics for Windows, Version
25.0 (IBM Corp., Armonk, NY, USA) software. The mean, frequencies, and range were
calculated. The differences between groups were analyzed using the chi-squared test
or the Fisher exact test for categorical data, and the t-test for continuous data, as appropriate, and significance was set at a p-value of 0.05.
Results
Population Characteristics
There were 108 cases included in the study, out of which 51 were male (47.2%) and
57 were female (52.8%) patients. The age ranged from 5 months to 15 years, with the
mean age being 5.39 ± 4.35 years. The majority of the children were younger than 5
years of age (60.16%) ([Table 1]). In our study, fever and painful neck swelling were the most common presentations.
Table 1
Age distribution of the children with neck space infection
|
Age
|
Frequency
|
Percentage
|
|
Up to 1 year
|
24
|
22.22
|
|
1–5 years
|
41
|
37.94
|
|
5–10 years
|
26
|
24.07
|
|
10–15 years
|
17
|
15.74
|
Self-medication Prior to Hospitalization
Sixty-four (59.25%) patients had taken medication prior to hospital admission ([Fig. 1]). The most commonly prescribed drug was a combination of ampicillin and cloxacillin
followed by azithromycin and a third-generation cephalosporin.
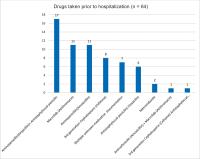 Fig. 1 Self-medication from the local medical shop before hospitalization.
Fig. 1 Self-medication from the local medical shop before hospitalization.
Disease Pattern
The majority of the cases were the submandibular and submental abscess secondary to
the dental origin, sialadenitis, lymph node suppuration after upper respiratory tract
infection ([Table 2]).
Table 2
Site and pattern of the children with neck abscess
|
Spaces localized above the hyoid level
|
Number
|
Percentage
|
|
1. Submandibular & submental abscess
|
55
|
50.9%
|
|
2. Parapharyngeal abscess
|
23
|
21.29%
|
|
3. Peritonsillar abscess
|
11
|
10.18%
|
|
4. Parotid abscess
|
5
|
4.67%
|
|
5. Masticator/Temporal abscess
|
3
|
2.78%
|
|
6. Ludwig's angina
|
3
|
2.78%
|
|
Spaces localized below the hyoid level
|
|
|
|
7. Anterior visceral
|
1
|
0.92%
|
|
Spaces localized in the entire circumference of the neck
|
|
|
|
8. Retropharyngeal abscess
|
3
|
2.78%
|
|
Miscellaneous
|
|
|
|
9. Necrotizing fasciitis of neck
|
4
|
3.7%
|
Bacterial Growth in the Pus Cultures
Positive Bacterial Growth in the Pus Culture
Out of 108 cases, pus culture was sent in 85 cases, 41 of which showed positive culture
(48.3%). Staphylococcus aureus was the most common organism isolated, which was followed by coagulase-negative staphylococci.
There were three cases of methicillin-resistant staphylococci isolated ([Fig. 2]).
 Fig. 2 Bacterial growth in the pus culture in children with neck abscess.
Fig. 2 Bacterial growth in the pus culture in children with neck abscess.
Drug Sensitivity and Resistance Pattern with Various Drugs among Positive Growth with
Staphylococcus Aureus
Only the sensitivity pattern of the most commonly used drugs was taken. In S. aureus, sensitivity was the highest to clindamycin (82.35%) followed by vancomycin (73.53%)
and cloxacillin (73.53%). The most commonly used drug, amoxicillin/ampicillin, had
the lowest sensitivity (20.58) ([Table 3]). Coagulase-negative staphylococci also had a similar sensitivity pattern ([Table 4]).
Table 3
Antibiotic sensitivity pattern for Staphylococcus aureus in the pus culture
|
Sensitivity pattern of Staphylococcus aureus (n = 34)
|
|
Drug
|
Sensitivity pattern
|
|
Sensitivity
|
Resistance
|
|
Clindamycin
|
28
|
(82.35%)
|
6
|
(17.64%)
|
|
Vancomycin
|
25
|
(73.53%)
|
9
|
(26.47%)
|
|
Cloxacillin
|
24
|
(70.59%)
|
10
|
(29.41%)
|
|
Gentamycin
|
23
|
(67.64%)
|
11
|
(32.36%)
|
|
Amikacin
|
23
|
(67.64%)
|
11
|
(32.36%)
|
|
Chloramphenicol
|
15
|
(44.11%)
|
19
|
(55.89%)
|
|
Erythromycin
|
10
|
(29.41%)
|
24
|
(70.58%)
|
|
Ciprofloxacin
|
9
|
(26.47%)
|
25
|
(73.53%)
|
|
Doxycycline
|
9
|
(26.47%)
|
25
|
(73.53%)
|
|
Levofloxacin
|
7
|
(20.58%)
|
27
|
(79.42%)
|
|
Ampicillin/Amoxicillin
|
7
|
(20.58%)
|
27
|
(79.42%)
|
Table 4
Antibiotic sensitivity pattern for coagulase-negative staphylococci in the pus culture
|
Sensitivity pattern of Coagulase-negative staphylococci (n = 4)
|
|
Drug
|
Sensitivity pattern
|
|
Sensitivity
|
Resistance
|
|
Clindamycin
|
4
|
(100%)
|
0
|
|
|
Vancomycin
|
4
|
(100%)
|
0
|
|
|
Cloxacillin
|
3
|
(75%)
|
1
|
(25%)
|
|
Amikacin
|
2
|
(50%)
|
2
|
(50%)
|
|
Gentamycin
|
2
|
(50%)
|
2
|
(50%)
|
|
Chloramphenicol
|
2
|
(50%)
|
2
|
(50%)
|
|
Ciprofloxacin
|
2
|
(50%)
|
2
|
(50%)
|
|
Doxycycline
|
2
|
(50%)
|
2
|
(50%)
|
|
Levofloxacin
|
2
|
(50%)
|
2
|
(50%)
|
|
Erythromycin
|
1
|
(50%)
|
3
|
(75%)
|
|
Ampicillin/Amoxicillin
|
0
|
|
4
|
(100%)
|
Abscess Resolution
Overall, 90.74% of cases improved after the initial treatment whether medically or
combined with surgical drainage.
Abscess Recurrence
There was recurrence in 10 cases, out of which 2 had multiple episodes of recurrence
([Table 5] and [6]).
Table 5
Recurrence rate among the children
|
Frequency
|
Percentage
|
|
None
|
98
|
90.74
|
|
Single recurrence
|
8
|
7.41
|
|
Multiple recurrence
|
2
|
1.85
|
|
Total
|
108
|
100.0
|
Table 6
Details of the children with recurrence
|
Recurrence
|
Age in years
|
Episode
|
Previous management
|
Space involved
|
Collection size noted in previous episode (in ml)
|
Possible reason for recurrence
|
Days of previous stay
|
|
Recurrence 1
|
5
|
Multiple
|
Surgical
|
Parotid /Parapharyngeal
|
15
|
Inadequate drainage
|
10
|
|
Recurrence 2
|
5
|
Single
|
Surgical
|
Submandibular
|
5
|
Inadequate drainage short duration of treatment
|
5
|
|
Recurrence 3
|
3
|
Single
|
Surgical
|
Parapharyngeal
|
20
|
−
|
8
|
|
Recurrence 4
|
5
|
Single
|
Surgical
|
Parotid
|
5
|
−
|
15
|
|
Recurrence 5
|
15
|
Single
|
Surgical
|
Parapharyngeal
|
18
|
−
|
12
|
|
Recurrence 6
|
6
|
Single
|
Surgical
|
Parotid
|
30
|
Inadequate drainage
|
8
|
|
Recurrence 7
|
10
|
Single
|
Surgical
|
Submandibular
|
15
|
−
|
9
|
|
Recurrence 8
|
7
|
Single
|
Surgical
|
Submandibular
|
5
|
−
|
8
|
|
Recurrence 9
|
2
|
Multiple
|
Surgical
|
Necrotizing fasciitis of neck
|
8
|
Immunocompromised
|
108
|
|
Recurrence 10
|
1
|
Single
|
Surgical
|
Submandibular
|
8
|
−
|
10
|
Complications
There was no complication including mortality noted in the study.
Length of Hospitalization
The mean hospital stay was 6.94 days. The mean duration of stay in the group with
medical management was 10.62 days, compared with 6.11 days, with a p-value of 0.07 ([Table 7]).
Table 7
Difference in the medical management group alone versus medical and surgical management
group
|
Overall
|
Medical and surgical management
|
Medical management only
|
p-value
|
|
Gender
|
Male (51)
|
|
38
|
13
|
0.133
|
|
Female(57)
|
|
49
|
8
|
|
Age
|
5.39
|
5.058
|
6.774
|
0.105
|
|
Total count prior to admission
|
15389
|
16040
|
12693
|
0.009
|
|
Days of stay
|
6.98
|
6.11
|
10.62
|
0.07
|
|
Recurrence rate
|
|
(8/78) 10.2%
|
(2/20) 10%
|
1
|
Discussion
Infections and abscesses around the neck are common in young children mostly due to
lymph node suppuration secondary to upper respiratory tract infection (URTI) or pharyngeal
infection. The other sources of infection in the neck leading to abscess formation
are of dental origin, infections of salivary glands, and cystic lesions of the neck.[7]
Fever is an invariable symptom in most neck abscesses. Other symptoms, like odynophagia,
drooling, and painful neck swelling, may not be very specific for parapharyngeal,
retropharyngeal, or peritonsillar abscesses; thus, this may lead to difficulty in
diagnosis in children. In our study, fever and painful neck swelling were the most
common presentations for all pediatric patients. The most common age range was 1 to
5 years, with the mean age being 5.32 years, which tallied with other studies.[8]
[9] The younger spectrum of patients being more affected could be related to an immature
immune system.[9] There was no observed difference in gender distribution.
In the present study, 44 cases (51.76%) did not show any growth in culture. Such a
large number of negative culture growth could be due to self-medication with antibiotics
prior to hospital admission. Sixty-four (59.25%) patients had taken medication prior
to hospital admission, 37 patients had been prescribed over-the-counter penicillin
group of drug, either alone as a combination, and referred to a specialist after the
non-resolution of the symptom. Azithromycin was prescribed in 12% (13/108) of cases,
with a single dose daily for 5 days. According to the systematic review done by Nepal
et al.,[10] the prevalence of self-medication with antibiotics (SMA) in Southeast Asia ranged
from 7.3 to 85.59%, with an overall prevalence of 42.64%. The other possibility could
be an atypical mycobacterial infection, which is not included in the routine culture
sensitivity tests.
Among the positive culture growth, the most common organism isolated was staphylococcus,
which was similar to the findings of various published studies.[4]
[7] The most sensitive antibiotic was clindamycin in 28 cases (82.25%), followed by
vancomycin and cloxacillin. This is similar to the findings in the published literature.[7] The reason for this may be clindamycin is active against staphylococci, penicillin-resistant
strains of Streptococcus pneumoniae, Streptococcus pyogenes, and viridans streptococci as well as most anaerobes. Clindamycin also reduces some
virulence factors of microbes, such as toxin production by S. aureus, Clostridium, and capsule formation by S. pyogenes, and S. pneumoniae, and it enhances phagocytosis of susceptible organisms.[11]
Staphylococcus aureus with resistance to multiple antibiotics, like methicillin-resistant
Staphylococcus aureus (MRSA), is highest in Asia.[12] Similarly, a higher resistance pattern is seen in low developing countries, such
as those in sub-Saharan Africa.[13] This is a matter of concern, especially in the context of pediatric deep neck space
infection, in which life-threatening complications can occur despite early treatment
with commonly used drugs, such as those in penicillin group (amoxicillin/ampicillin).
Ampicillin and amoxicillin are not penicillinase-resistant and, therefore, had a low
sensitivity of 17.03% and a high resistance pattern. Considering the safety profile,
among the oral penicillin group of drugs, cloxacillin had the highest sensitivity.
The recurrence rate was 9.26% (10/108), of which 8 cases had a single recurrence and
2 cases had more than 1. There were three cases with a single recurrence due to inadequate
drainage during the first treatment. All cases with multiple recurrences had multiple
neck space involvement. One case with necrotizing fasciitis secondary to immune suppression
had a prolonged stay and repeated recurrence with a chest infection. The recurrence
rate was high in young children (mostly below 7 years of age). The small size of young
babies with difficult anatomic location was likely the cause for the difficult drainage
and often inadequate drainage which might be the possible reason for the high recurrence
rate in our study. The repeat CT scan was not feasible in every case because of the
financial constraints, so, clinical judgment and ultrasonography were used as discharge
criteria as a parameter for subsidence of the abscess. Parapharyngeal and parotid
abscess with deep collection which are often missed, could be the possible reason
for high recurrence. Recurrence was common in both the small size and large size collections,
and inadequate drainage was the main reason for recurrence.
The mean duration of stay was longer in the group with medical management as compared
with those with medical treatment and surgical drainage ([Table 7]). Higher leukocyte count was found in surgically managed cases when compared with
those who needed only medical management. Higher leukocyte count might predict the
long duration of infection with pus formation and hence the need for incision and
drainage. Slightly raised leukocyte count indicates an early inflammation period (cellulitis
stage) with no abscess formation.
Potential life-threatening complications can arise despite using multiple medications.
The complications rate in pediatrics neck space abscesses is variable with the complication
rate in literature ranging from 9 to 12%.[2]
[14]
[15] However, there was no complication noted in our study.
Patigaroo et al. and Ossowski et al. emphasize surgical drainage to minimize the time
in the hospital and accelerates resolution.[2]
[16] However, the published study in parapharyngeal and retropharyngeal space infection
show the comparable outcome of conservative management to surgical intervention in
deep neck space.[17]
[18]
The treatment of neck space abscess consists of medical treatment, surgical intervention,
and management of complications. Due to the lack of universal consensus regarding
the approach to indications of surgical intervention, empirical choice, and duration
of antibiotic, the treatment should be individualized depending on the clinical response.[7]
The limitation of this study is that the culture and sensitivity pattern was not tested
with anaerobic organisms in all cases because of the problem in transport and culture
media. Similarly, the sensitivity testing of a commonly used drug, amoxicillin combined
with clavulanic acid, is lacking in this study as this is not always included in the
routine test. The small sample size is another potential limitation of the study.
Conclusion
The majority of neck abscess was due to staphylococcus. The empirical drug of choice
for deep neck space infection in pediatric patients is clindamycin or cloxacillin,
which should be followed by culture-guided appropriate antibiotics. Antistaphylococcal
drug (cloxacillin) alone should be used instead of a combination of ampicillin and
cloxacillin as the resistance to ampicillin is high. In an early presentation with
only slightly raised leukocyte count, the conservative management with appropriate
intravenous antibiotic alone is a good option.






