
Subscribe to RSS
DOI: 10.1055/s-0042-1744268
Hallux Rigidus: Current Concepts
Article in several languages: español | English
- Abstract
- Introduction
- Presentation
- Imaging
- Classification
- Treatment
- Surgical Treatment
- Cheilectomy
- Proximal Phalanx Osteotomy
- Distal Metatarsal Osteotomy
- Non-joint-sparing Techniques (Fig. 6)
- Conclusions
- Referencias
Abstract
Hallux rigidus is a frequent cause of traumatology consultations, and it is the most frequent osteoarthritis of the foot. It presents clinically with pain and loss of movement of the first metatarsophalangeal joint, with an impact on the quality of life of the patient. The treatment starts conservatively, and is successful in half of the cases, with measures such as modification of footwear, weight management and orthosis designed to limit the movement of the metatarsophalangeal joint. The surgical treatment in patients with mild to moderate hallux rigidus focuses on removing the dorsal osteophytes with a cheilectomy, which can be associated with a proximal phalanx or first metatarsal osteotomy, which improves the range of motion towards a less painful arch. In high-grade hallux rigidus, the most recommended treatment is still arthrodesis, which provides pain relief at the cost of altering gait biomechanics0 given the acquired stiffness. Different arthroplasties (resection, interposition or prosthetic) significantly improve pain without sacrificing mobility, and are a more physiological alternative to preserve the biomechanics of the foot in selected patients.
#
Introduction
Hallux rigidus (HR) is a degenerative and painful condition of the first metatarsophalangeal joint which presents a restricted range of motion with progressive formation of osteophytes.[1] It is the most common osteoarthritis of the foot, affecting 1 in 40 people older than 50 years of age, with a 2:1 female predilection.[2] [3] Up to 45% of adults have radiographic degenerative changes in the first metatarsophalangeal joint, but only 10% have symptomatic HR.[4] [5] Initially described by Davies-Colley[6] in 1887 as hallux flexus, months later Cotterill[1] [3] [7] introduced the term hallux rigidus.
The first metatarsophalangeal joint is a hinge joint with a greater range of dorsiflexion (40°–100°) than of plantar flexion (3°–43°). The range of motion on tiptoes is of 65°, but during walking it is only of 38°. When running, a range of up to 60° may be necessary.[8] It is important to differentiate it from hallux limitus or functional HR, in which the dorsiflexion of the first metatarsophalangeal joint is normal but decreases when weight is loaded, mainly due to alterations in the achilles-calcaneus-plantar system and/or the medial column of the foot.[9] A total of 60% of the cases have a family history, and 80% are bilateral.[6] [10]
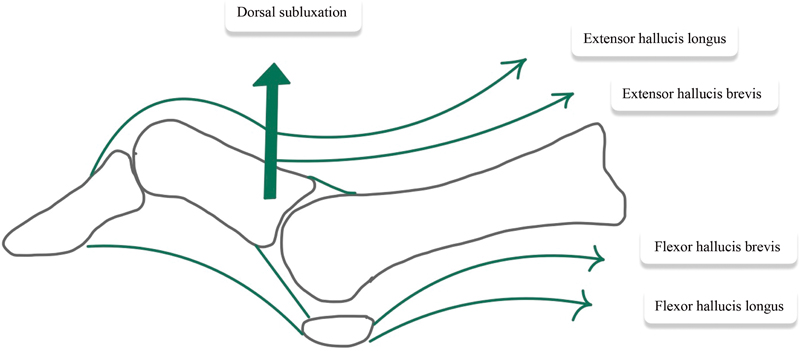
Inflammatory arthropathies, due to crystals and anatomical variations such as a long first metatarsal primus varus, or primus elevatus,[8] could be triggering conditions. Acute trauma or repetitive microtraumas could play a role in unilateral involvement.[1] Scarring of the joint capsule with abnormal centers of rotation results in altered compressive forces on the joint, with decreased range of motion[.11] ([Fig. 1])
On the other hand, it is difficult to establish whether the degenerative changes observed after corrective hallux valgus osteotomies (OTTs) are caused by the surgery itself or are the consequence of a preoperative deformity. In theory, correction of the incongruity improves the biomechanical conditions of the joint and the degenerative changes should not progress, but if an aggressive dissection is performed around the neck of the metatarsal bone, or a very distal OTT, the arterial supply can be damaged, evolving towards avascular necrosis of the head of the first metatarsal bone, with chondrolysis and progressive joint incongruity. Something similar occurs when contact forces increase at the joint level after malunion.[12]
#
Presentation
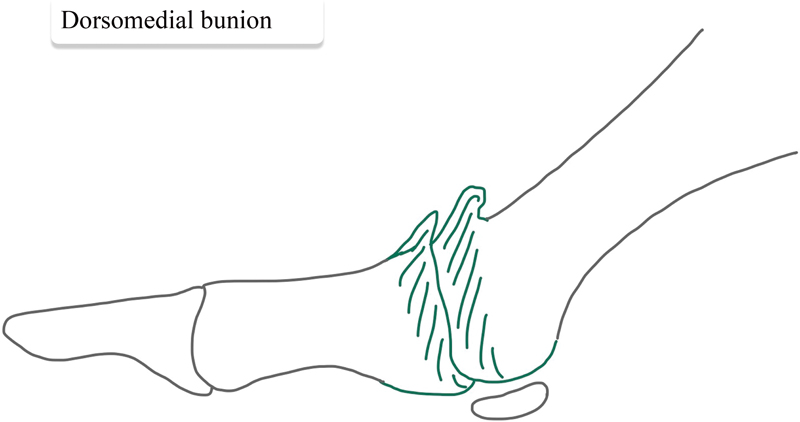
The patients present with pain in the extremes of movement, particularly at maximal dorsiflexion, such as it occurs when climbing stairs, running, or wearing high heels.[6] As the disease progresses, the pain is aggravated by daily activities, wearing flat shoes, and at rest. Transfer metatarsalgia and neuritis pain are due to impingement of the medial branch of the superficial peroneal nerve by dorsal osteophytes.[3] [13] [14] These, in turn, generate a dorsal prominence over the metatarsophalangeal joint called the dorsomedial bunion.[3] [13] [14] ([Fig. 2])
The axial compression test of the metatarsophalangeal joint or axial grind test is positive if it causes pain. Pain in the middle range of motion indicates the presence of advanced osteoarthritis.[13]
There are subtle gait disturbances to prevent full metatarsophalangeal dorsiflexion, showing early toe-out or increased foot progression angle. The foot supinates, which increases the load through the minor rays that lead to lateral metatarsalgia with compensatory hyperextension of the interphalangeal joint, generating hyperkeratosis under it.
In patients with functional HR, there is increased dorsiflexion of the hallux when the foot is examined in plantar flexion, as this relaxes the gastrocnemius and removes the restraining factor.[13] It is important to evaluate the presence of gastrocnemius shortening with the Silfverskiold test, since there is a correlation between its presence and forefoot overload.
#
Imaging
Although the diagnosis is clinical, evaluation with anteroposterior (AP), lateral, oblique foot and axial X-rays of the sesamoid bones enables the establishment of the most appropriate treatment.
The AP radiograph ([Fig. 3]) shows irregular narrowing of the joint space by osteophytes, with the metatarsal head larger and flattened.[13] Dorsal osteophytes can obstruct the AP view of the joint, leading to overestimation of the disease, with inaccurate assessment of the remaining cartilage and joint damage.[15] [16] On the oblique view, the true joint space is observed. Moreover, subchondral bone cysts and joint sclerosis may be observed.

The lateral radiograph ([Fig. 4]) shows dorsal osteophytes projecting proximally as “dripping candle wax”. The base of the proximal phalanx may appear larger and with a dorsal osteophyte parallel to the metatarsal head. There may be elevation of first metatarsal bone in relation to smaller metatarsal bones, which is called metatarsus primus elevatus, the sesamoids appear longer, and the distance to the base of the proximal phalanx decreases as the osteoarthritis progresses.[15]

Magnetic resonance imaging (MRI) and computed tomography (CT) are not routinely necessary, except in cases of normal radiographs with suspected osteochondral injury.[17]
#
Classification
The Hattrup and Johnson[18] and Coughlin and Shurnas[10] classifications ([table 1]) are among those used to evaluate HR, and they incorporate clinical findings (percentage of passive dorsiflexion) and radiographic criteria, providing guidelines about management.
|
Grade |
Examination findings |
Dorsiflexion (degrees)/% of loss compared to the contralateral side |
Radiographic findings |
|---|---|---|---|
|
0 |
Stiffness without pain |
40°–60°/10–20% |
Normal |
|
1 |
Occasional mild pain at extremes of motion |
30°–40°/ 20–50% |
Mild dorsal osteophyte, normal joint space |
|
2 |
Moderate and more constant pain, pain prior to the maximum range of motion |
10°–30° / 50–75% |
Moderate dorsal osteophyte, < 50% of joint space narrowing, flattened metatarsal head, > 25% of the dorsal joint compromised on lateral X-ray |
|
3 |
Significant stiffness, pain at extreme range of motion, no pain at midrange of motion |
≤ 10°/ 75–100% loss of plantar flexion in the metatarsophalangeal joint (normal: ≤ 10°) |
Severe dorsal osteophyte, > 50% of joint space narrowing, enlarged sesamoid +- cysts |
|
4 |
Significant stiffness, pain at extreme range of motion, pain at midrange of motion |
Same as grade 3 |
Same as grade 3 |
#
Treatment
Treatment begins with conservative management, which aims to relieve pain and achieve adequate function, with up to 55% of success.[3] [6] [8] [19] This includes weight management, if necessary.
Nonsteroidal anti-inflammatory drugs reduce inflammation and joint pain, but do not improve the long-term results, in addition to having gastric, renal and cardiac side effects. Intra-articular corticosteroid injection reduces pain to a limited extent and may adversely affect the joint cartilage; therefore, its use is not recommended.[20] Intra-articular injection of hyaluronic acid has shown promising results but requires more studies to establish its long-term effect.[21]
Shoe modifications, such as a Morton extension insole made of rigid material, may be helpful in reducing dorsiflexion and stress on the first metatarsophalangeal joint. In cases in which there is a symptomatic dorsal osteophyte,[22] wide and tall shoes can relieve pressure. Shoes with heels should be avoided.
The changes in daily activities decrease pain, avoiding excessive load in dorsiflexion when climbing stairs or running.
When all else fails, the surgical treatment is indicated.
#
Surgical Treatment
The goal of surgery is to relieve pain, restore function, maintain stability of the first metatarsophalangeal joint, and improve quality of life. The surgical techniques can be divided into joint-sparing and non-joint-sparing. It is also possible to consider the release of the gastrocnemius as an adjuvant procedure.[9]
Joint-sparing techniques ([Fig. 5]).

#
Cheilectomy
Described by DuVries[3] [6] in 1959, it consists of the removal of dorsal osteophytes and up to 30% of the metatarsal head so that it does not generate instability due to dorsal subluxation of the proximal phalanx. It is indicated in patients with HR of grades 1, 2 and some selected patients with grade 3. It provides an improvement of up to 60° of dorsiflexion of the first metatarsophalangeal,[23] with benefits regarding gait function. There may be recurrence of dorsal exostosis in up to 31% of the cases.[24] With less than 50% of the joint viable, cheilectomy is contraindicated.[2] [6] [8] The long-term results are good to excellent in 72% to 100% of the patients,[25] with 70% of patients free of pain after 6 years of follow-up[26] and low rates of conversion to arthrodesis. It can also be performed arthroscopically.[27]
#
Proximal Phalanx Osteotomy
Moberg OTT:[2] [13] it is a dorsal closing wedge osteotomy of the proximal phalanx. First described by Bonney y Macnab[6] in 1952, it simulates an increase in dorsiflexion that facilitates the take-off phase or third rocker, and shifts the center of pressure on the first metatarsal head in a plantar direction, reducing the force acting on the joint surface. A cheilectomy may be added. It is a good option for young patients with mild to moderate HR, and it has low rates of complications and revision, with high patient satisfaction.[28]
#
Distal Metatarsal Osteotomy
Youngswick OTT: it is a modified chevron OTT. After performing the 60° V-shaped OTT, a second OTT is performed parallel to the dorsal one, which results in shortening and plantar translation of the first metatarsal head, decompressing the joint, reducing pain, and eliminating dorsal impingement.[6] [19] It is indicated in cases of functional HR with an elongated first metatarsal bone, requiring shortening and plantar flexion of the head.[16] [29]
Reverdin Green OTT: it is a modification of the previous procedure. After performing the V-shaped OTT, a second OTT is performed in parallel at the dorsal end of the first OTT and the removed bone block is installed at the plantar end of the OTT to translate the metatarsal head to the plantar aspect. It is combined with cheilectomy.[29] [30]
Distal oblique sliding OTT: it is characterized by a single dorsodistal to proximal plantar oriented OTT line, beginning just proximal to the articular surface. The OTT angle is of approximately 35° to 45°. The capital fragment is displaced to the plantar aspect. It shortens the first ray and decompresses the metatarsophalangeal joint. Dorsiflexion improves from 22° to 45°, but it leads to excessive pressure under the lesser metatarsal heads, decreased forefoot supination, and sesamoid pain, as well as transfer metatarsalgia.[6] [29] [30]
#
Non-joint-sparing Techniques ([Fig. 6])

Arthrodesis: the standard in the treatment of severe HR,[6] it improves pain because it eliminates the residual layer of cartilage, sacrificing joint movement. It is indicated in grade-3 and -4 HR in patients with a high level of physical activity, in cases of concomitant hallux valgus, hallux varus, and rheumatoid arthritis, and as a rescue procedure in recurrence after joint-preservation procedures. The optimal position of the fusion is neutral rotation, 5° to 15° of valgus, and 10° to 15° of dorsiflexion. Excessive valgus increases the risk of interphalangeal joint degeneration. Increased dorsiflexion causes pain at the tip of the toe, over the interphalangeal joint, and below the metatarsal bone. Excessive plantar flexion increases distal hallux pressure.[6] Fixation can be performed with solid, cannulated, Herbert-type double compressive screws, dorsal plates, or Kirshner wires. Biomechanical studies[31] [32] have shown that the dorsal plate and the double compressive screw are superior to a 4-mm cancellous oblique screw both in strength at failure and in initial stiffness. If the shortening of the first metatarsal bone is greater than 5 mm, as seen in revisions, a graft is added.
Better results have been shown in terms of satisfaction, functional scores and lower pain scores on the Visual Analog Scale (VAS) for arthrodesis, with a lower revision rate compared to that of arthroplasty groups.[33]
Keller arthroplasty: it is the resection of the base of the proximal phalanx that decompresses the joint and increases its dorsiflexion while sacrificing stability. Its complications include weakness when walking off, transfer metatarsalgia to the second and third rays, and cock-up deformity in up to half of the patients. It is a simple procedure with short rehabilitation that provides pain relief and normal mobility in four to six weeks. It is indicated in elderly patients with little demand and contraindicated in patients with pre-existing rigid hyperextension deformity of the metatarsophalangeal joint.[3] [6] [8] [34] [35] [36]
Interposition arthroplasty: this procedure combines the Keller resection arthroplasty with the implantation of a biological spacer in the joint, which can be a capsular autograft, meniscal allograft, regenerative tissue matrix, or tendon autograft. It maintains length, and improves joint stability and movement compared to the Keller arthroplasty. It has complications similar to those of the Keller arthroplasty.[3] [34] Joint capsule interposition, described more than 20 years ago, has shown excellent results.[37] [38]
Prosthetic arthroplasty of the first metatarsophalangeal joint: prosthetic implants are classified according to the material (silicone or metal) and anchoring system used. The contraindications for their use are active infection, insufficient bone stock, severe joint deformities, and sesamoid arthritis. The complications, even with state-of-the-art implants, are infection, bone overgrowth, loosening, and persistent pain.[39] It is not yet possible to demonstrate its superiority over arthrodesis, and it shows lower satisfaction rates, higher pain scores, and worse functional results.[6] [16] [33]
Hemiarthroplasty: it consists of a unipolar implant designed to replace the articular surface of the metatarsal head or the base of the proximal phalanx. It requires lower levels of bone resection and maintains the length of the first ray. There is great disparity in relation to the results obtained.[1] [3] [6] [16] [39] In recent years, the polyvinyl alcohol hydrogel spacer (Cartiva, Inc., Alpharetta, GA, US) has been used, which would act as synthetic cartilage in the head of the first metatarsal bone, but the short- and medium-term follow-ups[40] [41] [42] only provide limited recommendations on the benefit of its use, as it is, in general, in hemiarthroplasty techniques, and it is not free of complications such as implant subsidence and fragmentation, infection, and osteolysis.[43]
#
Conclusions
Given the progressive aging of the population, it is expected that cases of degenerative pathologies will also increase. The main degenerative pathology in the foot is HR. Pain in the first metatarsophalangeal joint accompanied by a decrease in its range makes the diagnosis of an advanced stage evident; however, its identification in earlier stages is key to providing a less radical treatment, as is the current standard in the severe degree as is the arthrodesis.
#
#
Conflicto de Intereses
Los autores no tienen conflicto de intereses que declarar.
-
Referencias
- 1 Lucas DE, Hunt KJ. Hallux Rigidus: Relevant Anatomy and Pathophysiology. Foot Ankle Clin 2015; 20 (03) 381-389
- 2 Lam A, Chan JJ, Surace MF, Vulcano E. Hallux rigidus: How do I approach it?. World J Orthop 2017; 8 (05) 364-371
- 3 Anderson MR, Ho BS, Baumhauer JF. Current Concepts Review: Hallux Rigidus, Foot & Ankle Orthopaedics. 2018.
- 4 Roddy E, Thomas MJ, Marshall M. et al. The population prevalence of symptomatic radiographic foot osteoarthritis in community-dwelling older adults: cross-sectional findings from the clinical assessment study of the foot. Ann Rheum Dis 2015; 74 (01) 156-163
- 5 Wilder FV, Barrett JP, Farina EJ. The association of radiographic foot osteoarthritis and radiographic osteoarthritis at other sites. Osteoarthritis Cartilage 2005; 13 (03) 211-215
- 6 Ho B, Baumhauer J. Hallux rigidus. EFORT Open Rev 2017; 2 (01) 13-20
- 7 Seibert NR, Kadakia AR. Surgical management of hallux rigidus: cheilectomy and osteotomy (phalanx and metatarsal). Foot Ankle Clin 2009; 14 (01) 9-22
- 8 Lever CJ, , & , Robinson A. “Fred.” ( n.d. ). Midfoot and Forefoot Arthritis. Core Topics in Foot and Ankle Surgery, 120–142.
- 9 Vulcano E, Tracey III JA, Myerson MS. Accurate Measurement of First Metatarsophalangeal Range of Motion in Patients With Hallux Rigidus. Foot Ankle Int 2016; 37 (05) 537-541
- 10 Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003; 85 (11) 2072-2088
- 11 Shereff MJ, Bejjani FJ, Kummer FJ. Kinematics of the first metatarsophalangeal joint. J Bone Joint Surg Am 1986; 68 (03) 392-398
- 12 Filippi J, Briceño J. Complications after Metatarsal Osteotomies for Hallux Valgus. Foot Ankle Clin 2020; ; 25(1):169–182
- 13 Hamid KS, Parekh SG. Clinical Presentation and Management of Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 391-399
- 14 Keiserman LS, Sammarco VJ, Sammarco GJ. Surgical treatment of the hallux rigidus. Foot Ankle Clin 2005; 10 (01) 75-96
- 15 Asunción Márquez J, Martín Oliva X. Hallux rigidus: aetiology, diagnosis, classification and treatment. Rev Esp Cir Ortop Traumatol 2010; 54 (05) 321-328 (English Edition)
- 16 Polzer H, Polzer S, Brumann M, Mutschler W, Regauer M. Hallux rigidus: Joint preserving alternatives to arthrodesis - a review of the literature. World J Orthop 2014; 5 (01) 6-13
- 17 Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg 2012; 20 (06) 347-358
- 18 Hattrup SJ, Johnson KA. Subjective results of hallux rigidus following treatment with cheilectomy. Clin Orthop Relat Res 1988; (226) 182-191
- 19 Grady JF, Axe TM, Zager EJ, Sheldon LA. A retrospective analysis of 772 patients with hallux limitus. J Am Podiatr Med Assoc 2002; 92 (02) 102-108
- 20 Grice J, Marsland D, Smith G, Calder J. Efficacy of Foot and Ankle Corticosteroid Injections. Foot Ankle Int 2017; 38 (01) 8-13
- 21 Pons M, Alvarez F, Solana J, Viladot R, Varela L. Sodium hyaluronate in the treatment of hallux rigidus. A single-blind, randomized study. Foot Ankle Int 2007; 28 (01) 38-42
- 22 Shurnas PS. Hallux rigidus: etiology, biomechanics, and nonoperative treatment. Foot Ankle Clin 2009; 14 (01) 1-8
- 23 Wülker N, Rudert M. Hallux rigidus. Foot Ankle Surg 1999; 5 (02) 61-71
- 24 Easley ME, Davis WH, Anderson RB. Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999; 20 (03) 147-152
- 25 McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int 2013; 34 (01) 15-32
- 26 Sidon E, Rogero R, Bell T. et al. Long-term Follow-up of Cheilectomy for Treatment of Hallux Rigidus. Foot Ankle Int 2019; 40 (10) 1114-1121
- 27 Iqbal MJ, Chana GS. Arthroscopic cheilectomy for hallux rigidus. Arthroscopy 1998; 14 (03) 307-310
- 28 Warganich T, Harris T. Moberg Osteotomy for Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 433-450
- 29 Shariff R, Myerson MS. The Use of Osteotomy in the Management of Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 493-502
- 30 Galois L, Hemmer J, Ray V, Sirveaux F. Surgical options for hallux rigidus: state of the art and review of the literature. Eur J Orthop Surg Traumatol 2020; ; 30(1):57–65
- 31 Rongstad KM, Miller GJ, Vander Griend RA, Cowin D. A biomechanical comparison of four fixation methods of first metatarsophalangeal joint arthrodesis. Foot Ankle Int 1994; 15 (08) 415-419
- 32 Politi J, John H, Njus G, Bennett GL, Kay DB. First metatarsal-phalangeal joint arthrodesis: a biomechanical assessment of stability. Foot Ankle Int 2003; 24 (04) 332-337
- 33 Raikin SM, Ahmad J, Pour AE, Abidi N. Comparison of arthrodesis and metallic hemiarthroplasty of the hallux metatarsophalangeal joint. J Bone Joint Surg Am 2007; 89 (09) 1979-1985
- 34 Massimi S, Caravelli S, Fuiano M, Pungetti C, Mosca M, Zaffagnini S. Management of high-grade hallux rigidus: a narrative review of the literature. Musculoskelet Surg 2020; 104 (03) 237-243
- 35 Konkel KF, Menger AG. Mid-term results of titanium hemi-great toe implants. Foot Ankle Int 2006; 27 (11) 922-929
- 36 Mackey RB, Thomson AB, Kwon O, Mueller MJ, Johnson JE. The modified oblique keller capsular interpositional arthroplasty for hallux rigidus. J Bone Joint Surg Am 2010; 92 (10) 1938-1946
- 37 Hahn MP, Gerhardt N, Thordarson DB. Medial capsular interpositional arthroplasty for severe hallux rigidus. Foot Ankle Int 2009; 30 (06) 494-499
- 38 Hamilton WG, O'Malley MJ, Thompson FM, Kovatis PE. Roger Mann Award 1995. Capsular interposition arthroplasty for severe hallux rigidus. Foot Ankle Int 1997; 18 (02) 68-70
- 39 Gibson JNA, Thomson CE. Arthrodesis or total replacement arthroplasty for hallux rigidus: a randomized controlled trial. Foot Ankle Int 2005; 26 (09) 680-690
- 40 Bernasconi A, De Franco C, Iorio P, Smeraglia F, Rizzo M, Balato G. Use of synthetic cartilage implant (Cartiva®) for degeneration of the first and second metatarsophalangeal joint: what is the current evidence?. J Biol Regul Homeost Agents 2020; 34 (03, Suppl 2): 15-21, 2019
- 41 Smyth NA, Murawski CD, Hannon CP, Kaplan JR, Aiyer AA. The Use of a Synthetic Cartilage Implant for Hallux Rigidus: A Systematic Review. Foot Ankle Spec 2021; 14 (04) 366-371
- 42 Chrea B, Eble SK, Day J, Ellis SJ, Drakos MC, Orthopaedic Foot HSS. HSS Orthopaedic Foot and Ankle Surgery Group. Comparison Between Polyvinyl Alcohol Implant and Cheilectomy With Moberg Osteotomy for Hallux Rigidus. Foot Ankle Int 2020; 41 (09) 1031-1040
- 43 Metikala S, Mahmoud K, O'Connor KM, Chao W, Wapner KL, Farber DC. Adverse Events Related to Cartiva Hemiarthroplasty of First Metatarsal: An Analysis of Reports to the United States Food and Drug Administration. Foot Ankle Spec 2020; •••: 1938640020943715
Address for correspondence
Publication History
Received: 13 November 2021
Accepted: 11 January 2022
Article published online:
17 June 2022
© 2022. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referencias
- 1 Lucas DE, Hunt KJ. Hallux Rigidus: Relevant Anatomy and Pathophysiology. Foot Ankle Clin 2015; 20 (03) 381-389
- 2 Lam A, Chan JJ, Surace MF, Vulcano E. Hallux rigidus: How do I approach it?. World J Orthop 2017; 8 (05) 364-371
- 3 Anderson MR, Ho BS, Baumhauer JF. Current Concepts Review: Hallux Rigidus, Foot & Ankle Orthopaedics. 2018.
- 4 Roddy E, Thomas MJ, Marshall M. et al. The population prevalence of symptomatic radiographic foot osteoarthritis in community-dwelling older adults: cross-sectional findings from the clinical assessment study of the foot. Ann Rheum Dis 2015; 74 (01) 156-163
- 5 Wilder FV, Barrett JP, Farina EJ. The association of radiographic foot osteoarthritis and radiographic osteoarthritis at other sites. Osteoarthritis Cartilage 2005; 13 (03) 211-215
- 6 Ho B, Baumhauer J. Hallux rigidus. EFORT Open Rev 2017; 2 (01) 13-20
- 7 Seibert NR, Kadakia AR. Surgical management of hallux rigidus: cheilectomy and osteotomy (phalanx and metatarsal). Foot Ankle Clin 2009; 14 (01) 9-22
- 8 Lever CJ, , & , Robinson A. “Fred.” ( n.d. ). Midfoot and Forefoot Arthritis. Core Topics in Foot and Ankle Surgery, 120–142.
- 9 Vulcano E, Tracey III JA, Myerson MS. Accurate Measurement of First Metatarsophalangeal Range of Motion in Patients With Hallux Rigidus. Foot Ankle Int 2016; 37 (05) 537-541
- 10 Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of operative treatment. J Bone Joint Surg Am 2003; 85 (11) 2072-2088
- 11 Shereff MJ, Bejjani FJ, Kummer FJ. Kinematics of the first metatarsophalangeal joint. J Bone Joint Surg Am 1986; 68 (03) 392-398
- 12 Filippi J, Briceño J. Complications after Metatarsal Osteotomies for Hallux Valgus. Foot Ankle Clin 2020; ; 25(1):169–182
- 13 Hamid KS, Parekh SG. Clinical Presentation and Management of Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 391-399
- 14 Keiserman LS, Sammarco VJ, Sammarco GJ. Surgical treatment of the hallux rigidus. Foot Ankle Clin 2005; 10 (01) 75-96
- 15 Asunción Márquez J, Martín Oliva X. Hallux rigidus: aetiology, diagnosis, classification and treatment. Rev Esp Cir Ortop Traumatol 2010; 54 (05) 321-328 (English Edition)
- 16 Polzer H, Polzer S, Brumann M, Mutschler W, Regauer M. Hallux rigidus: Joint preserving alternatives to arthrodesis - a review of the literature. World J Orthop 2014; 5 (01) 6-13
- 17 Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg 2012; 20 (06) 347-358
- 18 Hattrup SJ, Johnson KA. Subjective results of hallux rigidus following treatment with cheilectomy. Clin Orthop Relat Res 1988; (226) 182-191
- 19 Grady JF, Axe TM, Zager EJ, Sheldon LA. A retrospective analysis of 772 patients with hallux limitus. J Am Podiatr Med Assoc 2002; 92 (02) 102-108
- 20 Grice J, Marsland D, Smith G, Calder J. Efficacy of Foot and Ankle Corticosteroid Injections. Foot Ankle Int 2017; 38 (01) 8-13
- 21 Pons M, Alvarez F, Solana J, Viladot R, Varela L. Sodium hyaluronate in the treatment of hallux rigidus. A single-blind, randomized study. Foot Ankle Int 2007; 28 (01) 38-42
- 22 Shurnas PS. Hallux rigidus: etiology, biomechanics, and nonoperative treatment. Foot Ankle Clin 2009; 14 (01) 1-8
- 23 Wülker N, Rudert M. Hallux rigidus. Foot Ankle Surg 1999; 5 (02) 61-71
- 24 Easley ME, Davis WH, Anderson RB. Intermediate to long-term follow-up of medial-approach dorsal cheilectomy for hallux rigidus. Foot Ankle Int 1999; 20 (03) 147-152
- 25 McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int 2013; 34 (01) 15-32
- 26 Sidon E, Rogero R, Bell T. et al. Long-term Follow-up of Cheilectomy for Treatment of Hallux Rigidus. Foot Ankle Int 2019; 40 (10) 1114-1121
- 27 Iqbal MJ, Chana GS. Arthroscopic cheilectomy for hallux rigidus. Arthroscopy 1998; 14 (03) 307-310
- 28 Warganich T, Harris T. Moberg Osteotomy for Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 433-450
- 29 Shariff R, Myerson MS. The Use of Osteotomy in the Management of Hallux Rigidus. Foot Ankle Clin 2015; 20 (03) 493-502
- 30 Galois L, Hemmer J, Ray V, Sirveaux F. Surgical options for hallux rigidus: state of the art and review of the literature. Eur J Orthop Surg Traumatol 2020; ; 30(1):57–65
- 31 Rongstad KM, Miller GJ, Vander Griend RA, Cowin D. A biomechanical comparison of four fixation methods of first metatarsophalangeal joint arthrodesis. Foot Ankle Int 1994; 15 (08) 415-419
- 32 Politi J, John H, Njus G, Bennett GL, Kay DB. First metatarsal-phalangeal joint arthrodesis: a biomechanical assessment of stability. Foot Ankle Int 2003; 24 (04) 332-337
- 33 Raikin SM, Ahmad J, Pour AE, Abidi N. Comparison of arthrodesis and metallic hemiarthroplasty of the hallux metatarsophalangeal joint. J Bone Joint Surg Am 2007; 89 (09) 1979-1985
- 34 Massimi S, Caravelli S, Fuiano M, Pungetti C, Mosca M, Zaffagnini S. Management of high-grade hallux rigidus: a narrative review of the literature. Musculoskelet Surg 2020; 104 (03) 237-243
- 35 Konkel KF, Menger AG. Mid-term results of titanium hemi-great toe implants. Foot Ankle Int 2006; 27 (11) 922-929
- 36 Mackey RB, Thomson AB, Kwon O, Mueller MJ, Johnson JE. The modified oblique keller capsular interpositional arthroplasty for hallux rigidus. J Bone Joint Surg Am 2010; 92 (10) 1938-1946
- 37 Hahn MP, Gerhardt N, Thordarson DB. Medial capsular interpositional arthroplasty for severe hallux rigidus. Foot Ankle Int 2009; 30 (06) 494-499
- 38 Hamilton WG, O'Malley MJ, Thompson FM, Kovatis PE. Roger Mann Award 1995. Capsular interposition arthroplasty for severe hallux rigidus. Foot Ankle Int 1997; 18 (02) 68-70
- 39 Gibson JNA, Thomson CE. Arthrodesis or total replacement arthroplasty for hallux rigidus: a randomized controlled trial. Foot Ankle Int 2005; 26 (09) 680-690
- 40 Bernasconi A, De Franco C, Iorio P, Smeraglia F, Rizzo M, Balato G. Use of synthetic cartilage implant (Cartiva®) for degeneration of the first and second metatarsophalangeal joint: what is the current evidence?. J Biol Regul Homeost Agents 2020; 34 (03, Suppl 2): 15-21, 2019
- 41 Smyth NA, Murawski CD, Hannon CP, Kaplan JR, Aiyer AA. The Use of a Synthetic Cartilage Implant for Hallux Rigidus: A Systematic Review. Foot Ankle Spec 2021; 14 (04) 366-371
- 42 Chrea B, Eble SK, Day J, Ellis SJ, Drakos MC, Orthopaedic Foot HSS. HSS Orthopaedic Foot and Ankle Surgery Group. Comparison Between Polyvinyl Alcohol Implant and Cheilectomy With Moberg Osteotomy for Hallux Rigidus. Foot Ankle Int 2020; 41 (09) 1031-1040
- 43 Metikala S, Mahmoud K, O'Connor KM, Chao W, Wapner KL, Farber DC. Adverse Events Related to Cartiva Hemiarthroplasty of First Metatarsal: An Analysis of Reports to the United States Food and Drug Administration. Foot Ankle Spec 2020; •••: 1938640020943715





