

Subscribe to RSS
DOI: 10.1055/s-0042-1744408
Meshed Acellular Dermal Matrix for Two-Staged Prepectoral Breast Reconstruction: An Institutional Experience
Authors
Abstract
The introduction of acellular dermal matrix (ADM) to breast reconstruction has allowed surgeons to reexplore the prepectoral implant placement technique in postmastectomy breast reconstruction. Our institution adopted a novel approach using meshed ADM to lessen the financial burden of increased ADM utilization with the prepectoral breast reconstruction. This is a retrospective, single-center review of two-stage prepectoral breast reconstruction using meshed human-derived ADM for anterior prosthesis coverage. Patient demographics, oncologic data, perioperative characteristics, and complications were examined and reported as means with standard deviations. Cost-saving with the meshed technique was evaluated. Forty-eight patients (72 breasts) with a mean age of 48.5 ± 15.0 years (range 26–70 years) were included in the study. The mean follow-up time was 13.2 ± 4.4 months (range 4.1–25.8 months). Nineteen breasts (24.6%) experienced complications, with seromas being the most common complication (12.5%, n = 9). Expander removal and reoperation occurred at a rate of 8.3 and 9.7%, respectively. The average time to drain removal was 18.8 ± 6.6 days (range 8–32 days). Meshed ADM provided an average cost savings of $6,601 for unilateral and $13,202 for bilateral reconstructions. Our study found that human-derived meshed ADM can be safely used in two-staged prepectoral tissue expander-based breast reconstruction and can result in significant cost savings.
Breast prostheses can be placed in either the prepectoral or subpectoral planes for breast reconstruction. The prepectoral technique places the prosthesis above the pectoralis major muscle. This technique dates back to the early use of implants in the 1960s but fell out of favor because of the increased rates of infection, excessive scar tissue formation causing capsular contracture, and occasional implant exposure.[1] These complications were attributed to inadequate soft tissue coverage.[2] Subsequently, surgeons placed the implants subpectorally, which provided more vascularized soft tissue coverage and addressed the aforementioned problems. This subpectoral approach became the preferred method for postmastectomy breast reconstruction for the next 15 years.[3]
The subpectoral placement of prostheses presented its own set of difficulties and complications, including functional impairment of the pectoralis muscle, animation deformities, and an increase in postoperative pain, all of which are consequences of the elevation and contraction of the pectoralis muscle.[3] [4] Aesthetically, this technique resulted in decreased projection and definition of the breast.[1] The advent of acellular dermal matrices (ADMs) has led plastic surgeons to reexplore prepectoral prosthesis placement for breast reconstruction. ADM provides an additional layer of soft tissue support for the tissue expander or implant, and reduces capsular contracture by serving as a barrier to the host's foreign body immune response.[5] [6] Prepectoral reconstruction using ADM allows for a softer reconstruction, adequate support to prevent “bottoming out,” and prevention of inframammary fold (IMF) malposition, rippling/wrinkling, and device exposure.[7]
There are various ways to use ADM in prepectoral reconstruction, including in vivo techniques whereby the prosthesis is covered anteriorly, either partially or entirely, and the ex vivo techniques of the “Wonton” wrap and the “Ravioli” wrap.[3] The “Wonton” wrap uses a single large sheet (typically a 16 × 20 cm piece) of ADM with the corners and edges sutured together on the posterior aspect of the prosthesis, and the “Ravioli” wrap uses two pieces of ADM, cut to the size of the device, and sutured to each other along the edge to completely enclose the prosthesis. Compared with dual-plane subpectoral reconstruction, where ADM is only used to provide lower breast pole coverage, prepectoral reconstruction requires one or multiple larger sheets of ADM. The additional ADM comes at a significant expense to the institution and patient.
Zammit et al[8] described the technique of meshing the ADM, using a skin mesher, to increase the surface area of a single sheet of ADM to provide adequate coverage and support for subpectoral implants. Our institution adopted the prepectoral breast reconstructive technique with anterior coverage of the tissue expander using a meshed ADM in 2018. Our study is a retrospective review of clinical outcomes and costs associated with the use of meshed ADM for prepectoral breast reconstruction in patients who underwent two-stage reconstruction. This is a novel modification to ADM, and there is a paucity of data on meshed ADM use in breast reconstruction. We will be comparing our findings to the two published studies on meshed ADM in breast reconstruction that are available in literature.
Methods
This study was exempted by the institutional review board (IRB00081784). A retrospective chart review identified consecutive postmastectomy female patients who underwent the first stage of a two-stage prepectoral tissue expander breast reconstruction with meshed ADM between May 2018 and January 2020. Procedures were performed by one of two senior plastic surgeons at one institution. Exclusion criteria were single-stage breast reconstructions, delayed reconstructions, meshed ADM introduced at later stages of reconstruction, and incomplete chart data.
Parameters recorded were age, body mass index (BMI), smoking status, comorbidities (e.g., obesity and diabetes), follow-up time, cancer stage, chemotherapy and radiation therapy, mastectomy technique, mastectomy specimen weight, expander size, initial and final expander fill volume, drain duration, ADM size and mesh ratio, complications (e.g., hematoma, seroma, infection, wound dehiscence, flap necrosis, expander removal, and reoperation), type of permanent implant (e.g., silicone or saline), and reconstruction type (e.g., none, nonautologous, autologous, or both). Complications were divided into major (requiring reoperation or tissue expander removal) and minor (resolved with therapies done in the clinic or without therapy). Smokers were required to stop smoking a minimum of 3 weeks before surgery.
Patient selection for the prepectoral meshed ADM technique was based on risk factors, body habitus, and preoperative discussions, including patient desires and activity levels. A breast oncologic surgeon performed either a skin-sparing or nipple-sparing mastectomy. After the mastectomy, the skip flaps were clinically examined to ensure adequate subcutaneous adipose layer and skin flap viability. If skin flaps were determined to be too thin, such that the dermis was exposed on pocket examination, or if there were concerns for inadequate skin flap perfusion, then the prepectoral meshed ADM technique was aborted and either the traditional subpectoral dual-plane tissue expander placement or delayed reconstruction was performed.
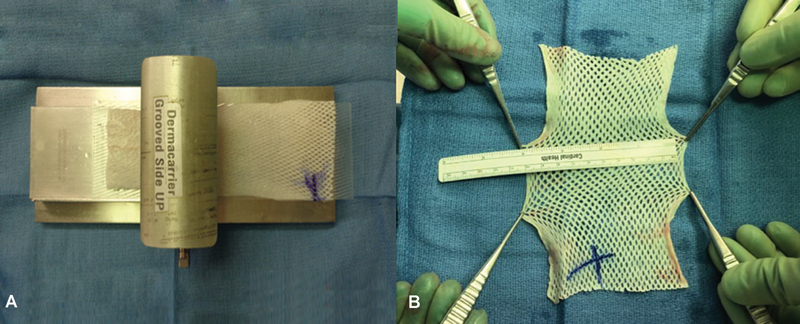
All of the ADM used were human-derived, rectangular-shaped, medium thickness, 6 × 16 cm or 8 × 16 cm, and from Alloderm RTU (LifeCell Corp., Branchburg, NJ) or DermACELL (LifeNet Health, Virginia Beach, VA). A 1:1.5 ratio Zimmer Biomet Skin Graft Mesher was used to mesh the ADM ([Fig. 1]). Both sized ADM sheets were medium thickness and easily passed through the mesher without complications.
Tissue expander sizes selected were based on patient desires and base diameter measured intraoperatively. The expander was deflated and placed against the chest wall and secured using the suture tabs. The meshed ADM was then placed into the mastectomy pocket, overlying the tissue expander, and the four “corners” were rounded to accommodate the pocket outline. The corners were then sutured to the underlying pectoralis major muscle and IMF fascia with 2.0 Vicryl interrupted suture. The superior, medial, and inferior borders were then sutured to the pectoralis major muscle and the IMF fascia with a running 2.0 Vicryl suture. Lateral overhang or redundant ADM was trimmed, and the lateral border was then sutured in a similar fashion to the serratus anterior fascia ([Fig. 2]). One or two 15-French round drains were placed between the meshed ADM and the skin flaps, depending on surgeon preference. The tissue expander was then inflated with saline to an appropriate volume to allow a tension-free skin flap closure. The incision was then closed in two layers.

Drains were removed when less than 30 mL of fluid was draining per day for 2 consecutive days, and serial expansion was initiated at 3 weeks postoperatively. Oral antibiotics were prescribed postoperatively until all drains were removed in clinic.
Patients then underwent a second-stage reconstruction with tissue expander removal and either implant placement or autologous tissue. This was performed after the patient had reached their desired tissue expansion size and a minimum of 3 months after expander placement or after all adjuvant treatments were completed. The existing mastectomy scar was reopened and the meshed ADM was incised transversely, enough to extract the tissue expander and place the permanent implant ([Fig. 3]) or perform autologous reconstruction. For implant-based reconstructions, the meshed ADM was then closed with interrupted 2.0 Vicryl sutures and the skin was closed in two layers. Superior pocket capsulotomies and fat grafting were performed in a select few patients for better contour and aesthetic outcomes ([Fig. 4]).


Results
Forty-eight patients (72 breasts) underwent the first of a two-staged prepectoral tissue expander breast reconstruction with meshed ADM between May 2018 and January 2020. The mean follow-up time was 13.2 ± 4.4 months (range 4.1–25.8 months). The average patient age was 48.5 ± 15.0 years (range 26–70 years). The mean BMI was 26.2 ± 5.3 kg/m2 (range 19.6–42.5 kg/m2). Eleven patients (22.9%) were obese, 1 (2.1%) was diabetic, 11 (22.9%) were former smokers, and 1 (2.1%) was an active smoker ([Table 1]).
Abbreviation: SD, standard deviation.
Of the 72 breasts that underwent a mastectomy, the number of breasts with cancer and their stages were as follows: 8 (11.1%) were stage 0, 14 (19.4%) were stage I, 16 (22.2%) were stage II, 5 (6.9%) were stage III, and 29 (40.3%) breasts were prophylactic. Fifty-seven breasts (79.2%) had no radiation therapy, and 15 (20.8%) had adjuvant radiation therapy. As for chemotherapy, 26 patients (54.2%) had none, 12 (25.0%) had neoadjuvant, 9 (18.8%) had adjuvant, and 1 (2.1%) had both neoadjuvant and adjuvant chemotherapy ([Table 2]).
Of the 48 patients, 24 of the cases (50%) were bilateral, and 24 (50%) were unilateral mastectomies. Fifteen mastectomies (20.8%) were nipple-sparing and 57 mastectomies (79.2%) were skin-sparing. The mean mastectomy specimen weight was 487.7 ± 195.9 g (range 132–1,056 g). The mean expander size used was 466.0 ± 93.5 mL (range 300–700 mL), mean intraoperative initial fill volume was 248.9 ± 105.0 mL (52.7% ± 18.0%), and the mean final tissue expander fill volume was 424.6 ± 145.9 mL (range 150–700 mL). The average time for drain removal was postoperative day 18.8 ± 6.6 (range 8–32 days). ADMs 6 × 16 cm (n = 46, 62.2%) and 8 × 16 cm (n = 28, 37.8%) were used, respectively ([Table 3]).
Abbreviation: SD, standard deviation.
Complications occurred in 14 (29.2%) patients and 19 (26.4%) breasts; they are listed as follows (seven breasts have a sequence of complications that contributed to the counts of multiple complications): 1 (1.4%) hematoma, 9 (12.5%) seromas, 5 (6.9%) infections, 4 (5.6%) wound dehiscences, 3 (4.2%) flap necroses, 6 (8.3%) expander removals, and 7 (9.7%) reoperations. Eight of the nine seromas resolved with aspiration or on their own. Out of the 15 (20.8%) breasts that received radiotherapy, 3 (4.2%) resulted in complications with 1 (1.4%) tissue expander removal. Additionally, one expander was removed due to flap necrosis and four expanders were removed due to infection that did not resolve with antibiotic therapy. Out of the seven (9.7%) reoperations, six (8.3%) were to remove the tissue expanders and one (1.4%) was to evacuate a hematoma ([Table 4]).
At the time of manuscript submission, 40 out of the 48 patients (83.3%) had completed second-stage reconstruction. Fifty-nine breasts (93.3%) had undergone second-stage reconstruction: 42 (58.3%) had implant-based reconstructions, 8 (11.1%) had autologous reconstructions, and 7 (9.7%) had both. Of those with implant-based reconstructions, 44 (89.8%) were with silicone, and 5 (10.2%) were with saline permanent implants ([Table 5]).
|
Characteristics |
No. (%) |
|---|---|
|
No. of second-stage reconstruction completion patients[a] |
40 (83.3) |
|
Reconstruction type (n = 72) |
|
|
None |
2 (2.8) |
|
Nonautologous |
42 (58.3) |
|
Autologous |
8 (11.1) |
|
Both |
7 (9.7) |
|
Pending |
13 (18.1) |
|
Implant exchange (n = 49) |
|
|
Silicone |
44 (89.8) |
|
Saline |
5 (10.2) |
a Total number of patients = 48.
At our institution, using a single-meshed 6 × 16 cm sheet of ADM instead of a 16 × 20 cm unmeshed sheet resulted in a saving of $6,601 for a unilateral, and $13,202 for a bilateral tissue expander reconstructive procedure. For bigger expanders with larger surface area and width, where a meshed 8 × 16 cm sheet was needed, the cost savings was $5,659 and $11,318 in unilateral and bilateral breast reconstructions, respectively (exact costs vary by institution and ADM manufacturer) when compared with a 16 × 20 cm unmeshed sheet.
Discussion
ADM is composed of extracellular collagenous material derived from decellularized xenogeneic or human cadaveric skin that serves as a biologic scaffold for host cellular integration and revascularization. First adopted in breast surgery in 2001, ADM is now utilized by 84% of plastic surgeons as an adjunct in both single- and two-stage breast reconstructive procedures.[9] Prior attempts at prepectoral breast implant placement resulted in serious complications due to the inadequacy of the thin and ischemic mastectomy skin envelope in accommodating a device.[10] With the addition of ADM, prepectoral breast implant placement was again explored, which resulted in improved aesthetic outcomes and reduced risk of capsular contracture.[5] [7]
The introduction of ADM in prepectoral breast reconstruction is a relatively new development, and a standardized technique is lacking. Variations in surgeon technique, ADM placement (e.g., complete coverage vs. anterior coverage of the device), type of ADM (e.g., bovine-, porcine-, vs. human-derived), and ADM modifications (e.g., whole sheet, fenestrated, vs. meshed) have resulted in high degrees of heterogeneity between studies that make comparisons difficult. Meshing ADM is also a relatively novel modification, therefore literature on the subject is also deficient.
Since the introduction of meshing ADM with a skin mesher by Zammit et al in 2016,[8] there have been two studies on meshed ADM in breast reconstruction. Hagarty et al[4] compared postoperative outcomes of subpectoral breast reconstruction using a 1:1 and 1:1.5 meshing ratio of human-derived ADM to unmeshed ADM. Concerned about ADM laxity, she later changed to a 1:1 mesh ratio for the ADM. This study found that meshing ADM decreases postoperative drain removal times, postoperative pain, and length of stay in the hospital. Complications were collectively reported as overall, major (resulted in reoperations), and minor complications. Lotan et al[11] compared a ratio of 1:2 meshed bovine-derived ADM to fenestrated bovine-derived ADM of mostly single-stage (84.3% direct-to-implant) breast reconstructions, and found reduced rates of seromas, hematomas, and infections, and postoperative drain removal times. Both studies have found meshed ADM in breast reconstruction as effective and safe in comparison to unmeshed ADM. The literature has reported a difference in the outcomes of xenogeneic and allogeneic ADMs. Human-derived ADM has been found to have significantly fewer complication rates than bovine- and porcine-derived ADMs.[12] Our study found that human-derived meshed ADM can be safely used in two-staged prepectoral tissue expander-based breast reconstruction and can result in significant cost savings.
In our study, 26.4% (n = 19) of breasts experienced complications, with the two other meshed ADM papers reporting similar complication rates (21.5% in the human-derived ADM subpectoral[4] and 29.5% in the bovine-derived ADM prepectoral[11]). It has been well reported in meta-analyses that ADM increases overall complication (odds ratio, 1.13–1.33) compared with no ADM use, and some case series reported rates between 4 and 41%.[13] [14] Although the rates of complications within the three meshed studies are within the reported rates in literature, the major complications requiring reoperation were relatively low (9.7% in our study, 4.6% in Hagarty et al, and 13.0% in Lotan et al).
Our study had an 8.3% and Lotan et al had a 5.2% prosthesis removal rate in the breast reconstructions with meshed ADM. These proportions are within the literature-reported rates of implant or tissue expander loss in prepectoral breast reconstruction using unmeshed ADM (3.5–10.2%).[15] [16] [17] [18]
Seroma formation is the most commonly reported complication in ADM use in breast reconstruction, with rates ranging widely from 1.5 to 14.1%.[13] [19] [20] In our study, the rate of seroma occurrences was 12.5% (n = 9), with one major seroma (1.4%) resulting in a sequence of infection, reoperation, and tissue expander removal. Lotan et al found a significant difference in major seromas between the meshed and unmeshed cohorts (0% vs. 8.2%, p < 0.01).[11] While ADM meshing is a relatively novel concept in breast reconstruction, commercially available fenestrated ADM has shown benefit in reducing the risk of postoperative seroma formation relative to nonfenestrated ADM.[21] [22] [23]
With the decrease in seroma formation, it is also speculated that meshing the ADM will decrease the time to drain removal since the two reflect the same process. Our average time of drain removal is 18.8 ± 6.6 days (range 8–32 days). The other meshed ADM studies found a significant decrease in drain removal time in their meshed cohorts compared with the unmeshed cohorts (18.78 vs. 28.81 days, p < 0.001 and 8.3 vs. 10.0 days, p < 0.01).[4] [11] The integration of the ADM to surrounding tissues is associated with the normal healing process that includes exudation of fluids.[2] The meshing and fenestrations in the ADM are hypothesized to allow the free fluid to more easily egress, enhancing the effacement between the ADM graft and skin flaps, and accelerating cellular integration and revascularization via improved tissue oxygenation and fibroblast and macrophage lineage host integration.[21] [22] [24]
The ADM's additional enhanced support is theorized to allow for increased intraoperative inflation of tissue expanders and fewer postoperative fill sessions and, therefore, clinic visits.[25] [26] Our study had a 52.7% initial fill volume, but our study did not follow the number of postoperative fills and clinic visits. Hagarty el al's study found a lower initial fill volume of tissue expanders in the meshed ADM compare with the unmeshed ADM cohort (52.89% vs. 73.51%, p < 0.001).[4] In contrast, Lotan et al[11] had an increase in initial fill volume in the meshed ADM in comparison to the fenestrated ADM cohort, although the finding was insignificant (94.9% vs. 74.9%, p = 0.125). The variations in meshing ratios likely explain the differences found in the initial fill volumes of the different studies.
In our study, 3 (4.1%) of the 15 breasts (20.8%) that had adjuvant radiotherapy resulted in complications: one infection that resolved with antibiotic treatment, one flap necrosis and infection that resulted in tissue expander removal, and one hematoma that resulted in reoperation for evacuation, but the tissue expander was retained. Of the six (8.3%) tissue expander losses, only one breast had radiotherapy. The literature is overall conflicted on the long-term impact of radiotherapy when ADM is used in breast reconstruction, and there is no data on the impact of radiotherapy on ADM that is meshed.[27]
Anterior coverage of the breast prosthesis often requires one 16 × 20 cm or two 6 × 16 cm sheets of ADM per breast, and complete wrapping (anterior and posterior coverage) can require two 16 × 20 cm sheets of ADM per breast. Given the significant expense of ADM, many surgeons have questioned whether it is a worthwhile adjunct in breast reconstruction procedures. Bank et al determined that ADM placement reduced the number of expansion visits for fill volumes greater than 350 mL, although these economic savings failed to offset the cost of the graft.[28] By increasing the surface area of ADM up to 50% through meshing, we were able to obviate the need for larger, 16 × 20 cm sheets of ADM, resulting in an average cost reduction of $6,601 for unilateral and $13,202 for bilateral reconstructions with a single sheet of 6 × 16 cm meshed ADM per side.
The anterior coverage technique of ADM must span the length and width of the implant or expander.[29] Sheets that are too short to cover the implant fully may cause compression of the inferior pole, superior migration, and limited projection.[29] In the case of two-staged reconstruction, the ADM should be sutured into place with some laxity to accommodate eventual inflation of the tissue expander.[30] Our use of meshed ADM increases the sheet's surface area to allow for full anterior coverage of a tissue expander by a single piece of ADM, while maintaining structural integrity.
This study's goal was an early assessment of the safety and efficacy of meshed ADM in two-staged prepectoral breast reconstruction; however, it is not without limitations. The prepectoral technique was first adopted along with ADM meshing at our institution, so there is no unmeshed ADM prepectoral cohort for comparison. Due to the relatively new introduction and modification in ADM use in breast reconstruction, more long-term and high-quality studies are needed to understand the incidence and causality of complications associated with meshing ADM. We hope to continue patient accrual and follow-up to ensure adequate long-term aesthetic and patient-reported outcomes with prepectoral meshed ADM. Meanwhile, we believe that a single sheet of meshed ADM for anterior prosthesis coverage is a safe and effective option for women who desire prepectoral breast reconstruction.
Conflict of Interest
J.P.A. is a consultant for DonJoy Orthopedics. The rest of the authors have nothing to disclose.
Author Contributions
Conceptualization: R.N.W.-Jr, N.M., A.C.K., J.P.A. Data curation: J.L., R.N.W.-Jr, S.M.O., M.P. Investigation: J.L., R.N.W.-Jr, A.C.K., J.P.A. Methodology: J.L., R.N.W.-Jr, A.C.K., J.P.A. Project administration: J.L., R.N.W.-Jr, A.C.K., J.P.A. Supervision, validation, visualization: A.C.K., J.P.A. Writing - original draft: J.L., R.N.W.-Jr, S.M.O. Writing - review and editing: J.L., A.C.K., J.P.A.
Ethical Approval
This study was exempted by the Institutional Review Board of University of Utah Hospital (IRB00081784) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived because this study design is a retrospective chart review.
Patient Consent
The patients provided written informed consent for the publication and the use of their images.
Prior Presentation
This article was presented at the Mountain West Society of Plastic Surgeons, Squaw Valley, Lake Tahoe, March 7–10, 2019.
* The two authors contributed equally to this work.
-
References
- 1 Bloom JA, Patel K, Cohen S. et al. Prepectoral breast reconstruction: an overview of the history, technique, and reported complications. Open Access Surg 2020; 13: 1-9
- 2 Zenn MR. Indications and controversies for implant-based breast reconstruction utilizing biological meshes. Clin Plast Surg 2018; 45 (01) 55-63
- 3 Sigalove S. Options in acellular dermal matrix-device assembly. Plast Reconstr Surg 2017; 140 (6S Prepectoral Breast Reconstruction): 39S-42S
- 4 Hagarty SE, Yen LL, Luo J, Fosco CR, Gomez K, Khare M. Decreased length of postoperative drain use, parenteral opioids, length of stay, and complication rates in patients receiving meshed versus unmeshed acellular dermal matrix in 194 submuscular tissue expander-based breast reconstructions: a single-surgeon cohort study. Plast Reconstr Surg 2020; 145 (04) 889-897
- 5 Uzunismail A, Duman A, Perk C. et al. The effects of acellular dermal allograft (AlloDerm®) interface on silicone-related capsule formation—experimental study. Eur J Plast Surg 2008; 31: 179-185
- 6 Salzberg CA, Ashikari AY, Berry C, Hunsicker LM. Acellular dermal matrix-assisted direct-to-implant breast reconstruction and capsular contracture: a 13-year experience. Plast Reconstr Surg 2016; 138 (02) 329-337
- 7 Sigalove S, Maxwell GP, Sigalove NM. et al. Prepectoral implant-based breast reconstruction: rationale, indications, and preliminary results. Plast Reconstr Surg 2017; 139 (02) 287-294
- 8 Zammit D, Kanevsky J, Meng FY. et al. Meshed acellular dermal matrix: technique and application in implant based breast reconstruction. Plast Aesthet Res 2016; 3: 254-256
- 9 Ibrahim AM, Koolen PG, Ashraf AA. et al. Acellular dermal matrix in reconstructive breast surgery: survey of current practice among plastic surgeons. Plast Reconstr Surg Glob Open 2015; 3 (04) e381
- 10 Kim SE. Prepectoral breast reconstruction. Yeungnam Univ J Med 2019; 36 (03) 201-207
- 11 Lotan AM, Ben Yehuda D, Allweis TM, Scheflan M. Comparative study of meshed and nonmeshed acellular dermal matrix in immediate breast reconstruction. Plast Reconstr Surg 2019; 144 (05) 1045-1053
- 12 Paprottka FJ, Krezdorn N, Sorg H. et al. Evaluation of complication rates after breast surgery using acellular dermal matrix: median follow-up of three years. Plast Surg Int 2017; 2017: 1283735
- 13 Gravina PR, Pettit RW, Davis MJ, Winocour SJ, Selber JC. Evidence for the use of acellular dermal matrix in implant-based breast reconstruction. Semin Plast Surg 2019; 33 (04) 229-235
- 14 Hallberg H, Rafnsdottir S, Selvaggi G. et al. Benefits and risks with acellular dermal matrix (ADM) and mesh support in immediate breast reconstruction: a systematic review and meta-analysis. J Plast Surg Hand Surg 2018; 52 (03) 130-147
- 15 Nealon KP, Weitzman RE, Sobti N. et al. Prepectoral direct-to-implant breast reconstruction: safety outcome endpoints and delineation of risk factors. Plast Reconstr Surg 2020; 145 (05) 898e-908e
- 16 Baker BG, Irri R, MacCallum V, Chattopadhyay R, Murphy J, Harvey JR. A prospective comparison of short-term outcomes of subpectoral and prepectoral Strattice-based immediate breast reconstruction. Plast Reconstr Surg 2018; 141 (05) 1077-1084
- 17 Wormer BA, Valmadrid AC, Ganesh Kumar N. et al. Reducing expansion visits in immediate implant-based breast reconstruction: a comparative study of prepectoral and subpectoral expander placement. Plast Reconstr Surg 2019; 144 (02) 276-286
- 18 Jafferbhoy S, Chandarana M, Houlihan M. et al. Early multicentre experience of pre-pectoral implant based immediate breast reconstruction using Braxon® . Gland Surg 2017; 6 (06) 682-688
- 19 Lee JS, Kim JS, Lee JH. et al. Prepectoral breast reconstruction with complete implant coverage using double-crossed acellular dermal matrixs. Gland Surg 2019; 8 (06) 748-757
- 20 Heidemann LN, Gunnarsson GL, Salzberg CA, Sørensen JA, Thomsen JB. Complications following nipple-sparing mastectomy and immediate acellular dermal matrix implant-based breast reconstruction: a systematic review and meta-analysis. Plast Reconstr Surg Glob Open 2018; 6 (01) e1625
- 21 Martin JB, Moore R, Paydar KZ, Wirth GA. Use of fenestrations in acellular dermal allograft in two-stage tissue expander/implant breast reconstruction. Plast Reconstr Surg 2014; 134 (05) 901-904
- 22 Palaia DA, Arthur KS, Cahan AC, Rosenberg MH. Incidence of seromas and infections using fenestrated versus nonfenestrated acellular dermal matrix in breast reconstructions. Plast Reconstr Surg Glob Open 2015; 3 (11) e569
- 23 Wirth GA, Mowlds DS, Guidotti P. et al. Acellular dermal matrix fenestrations and their effect on breast shape. Eur J Plast Surg 2015; 38: 267-272
- 24 Cottler PS, Olenczak JB, Ning B. et al. Fenestration improves acellular dermal matrix biointegration: an investigation of revascularization with photoacoustic microscopy. Plast Reconstr Surg 2019; 143 (04) 971-981
- 25 Hoppe IC, Yueh JH, Wei CH, Ahuja NK, Patel PP, Datiashvili RO. Complications following expander/implant breast reconstruction utilizing acellular dermal matrix: a systematic review and meta-analysis. Eplasty 2011; 11: e40
- 26 Lee KT, Mun GH. Updated evidence of acellular dermal matrix use for implant-based breast reconstruction: a meta-analysis. Ann Surg Oncol 2016; 23 (02) 600-610
- 27 Kim JYS, Mlodinow AS. What's new in acellular dermal matrix and soft-tissue support for prosthetic breast reconstruction. Plast Reconstr Surg 2017; 140 (5S Advances in Breast Reconstruction): 30S-43S
- 28 Bank J, Phillips NA, Park JE, Song DH. Economic analysis and review of the literature on implant-based breast reconstruction with and without the use of the acellular dermal matrix. Aesthetic Plast Surg 2013; 37 (06) 1194-1201
- 29 Nahabedian MY. Acellular dermal matrices in primary breast reconstruction: principles, concepts, and indications. Plast Reconstr Surg 2012; 130 (5, Suppl 2): 44S-53S
- 30 Nahabedian MY. Prosthetic breast reconstruction with acellular dermal matrices: achieving predictability and reproducibility. Plast Reconstr Surg Glob Open 2016; 4 (05) e698
Address for correspondence
Publication History
Article published online:
06 April 2022
© 2022. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Bloom JA, Patel K, Cohen S. et al. Prepectoral breast reconstruction: an overview of the history, technique, and reported complications. Open Access Surg 2020; 13: 1-9
- 2 Zenn MR. Indications and controversies for implant-based breast reconstruction utilizing biological meshes. Clin Plast Surg 2018; 45 (01) 55-63
- 3 Sigalove S. Options in acellular dermal matrix-device assembly. Plast Reconstr Surg 2017; 140 (6S Prepectoral Breast Reconstruction): 39S-42S
- 4 Hagarty SE, Yen LL, Luo J, Fosco CR, Gomez K, Khare M. Decreased length of postoperative drain use, parenteral opioids, length of stay, and complication rates in patients receiving meshed versus unmeshed acellular dermal matrix in 194 submuscular tissue expander-based breast reconstructions: a single-surgeon cohort study. Plast Reconstr Surg 2020; 145 (04) 889-897
- 5 Uzunismail A, Duman A, Perk C. et al. The effects of acellular dermal allograft (AlloDerm®) interface on silicone-related capsule formation—experimental study. Eur J Plast Surg 2008; 31: 179-185
- 6 Salzberg CA, Ashikari AY, Berry C, Hunsicker LM. Acellular dermal matrix-assisted direct-to-implant breast reconstruction and capsular contracture: a 13-year experience. Plast Reconstr Surg 2016; 138 (02) 329-337
- 7 Sigalove S, Maxwell GP, Sigalove NM. et al. Prepectoral implant-based breast reconstruction: rationale, indications, and preliminary results. Plast Reconstr Surg 2017; 139 (02) 287-294
- 8 Zammit D, Kanevsky J, Meng FY. et al. Meshed acellular dermal matrix: technique and application in implant based breast reconstruction. Plast Aesthet Res 2016; 3: 254-256
- 9 Ibrahim AM, Koolen PG, Ashraf AA. et al. Acellular dermal matrix in reconstructive breast surgery: survey of current practice among plastic surgeons. Plast Reconstr Surg Glob Open 2015; 3 (04) e381
- 10 Kim SE. Prepectoral breast reconstruction. Yeungnam Univ J Med 2019; 36 (03) 201-207
- 11 Lotan AM, Ben Yehuda D, Allweis TM, Scheflan M. Comparative study of meshed and nonmeshed acellular dermal matrix in immediate breast reconstruction. Plast Reconstr Surg 2019; 144 (05) 1045-1053
- 12 Paprottka FJ, Krezdorn N, Sorg H. et al. Evaluation of complication rates after breast surgery using acellular dermal matrix: median follow-up of three years. Plast Surg Int 2017; 2017: 1283735
- 13 Gravina PR, Pettit RW, Davis MJ, Winocour SJ, Selber JC. Evidence for the use of acellular dermal matrix in implant-based breast reconstruction. Semin Plast Surg 2019; 33 (04) 229-235
- 14 Hallberg H, Rafnsdottir S, Selvaggi G. et al. Benefits and risks with acellular dermal matrix (ADM) and mesh support in immediate breast reconstruction: a systematic review and meta-analysis. J Plast Surg Hand Surg 2018; 52 (03) 130-147
- 15 Nealon KP, Weitzman RE, Sobti N. et al. Prepectoral direct-to-implant breast reconstruction: safety outcome endpoints and delineation of risk factors. Plast Reconstr Surg 2020; 145 (05) 898e-908e
- 16 Baker BG, Irri R, MacCallum V, Chattopadhyay R, Murphy J, Harvey JR. A prospective comparison of short-term outcomes of subpectoral and prepectoral Strattice-based immediate breast reconstruction. Plast Reconstr Surg 2018; 141 (05) 1077-1084
- 17 Wormer BA, Valmadrid AC, Ganesh Kumar N. et al. Reducing expansion visits in immediate implant-based breast reconstruction: a comparative study of prepectoral and subpectoral expander placement. Plast Reconstr Surg 2019; 144 (02) 276-286
- 18 Jafferbhoy S, Chandarana M, Houlihan M. et al. Early multicentre experience of pre-pectoral implant based immediate breast reconstruction using Braxon® . Gland Surg 2017; 6 (06) 682-688
- 19 Lee JS, Kim JS, Lee JH. et al. Prepectoral breast reconstruction with complete implant coverage using double-crossed acellular dermal matrixs. Gland Surg 2019; 8 (06) 748-757
- 20 Heidemann LN, Gunnarsson GL, Salzberg CA, Sørensen JA, Thomsen JB. Complications following nipple-sparing mastectomy and immediate acellular dermal matrix implant-based breast reconstruction: a systematic review and meta-analysis. Plast Reconstr Surg Glob Open 2018; 6 (01) e1625
- 21 Martin JB, Moore R, Paydar KZ, Wirth GA. Use of fenestrations in acellular dermal allograft in two-stage tissue expander/implant breast reconstruction. Plast Reconstr Surg 2014; 134 (05) 901-904
- 22 Palaia DA, Arthur KS, Cahan AC, Rosenberg MH. Incidence of seromas and infections using fenestrated versus nonfenestrated acellular dermal matrix in breast reconstructions. Plast Reconstr Surg Glob Open 2015; 3 (11) e569
- 23 Wirth GA, Mowlds DS, Guidotti P. et al. Acellular dermal matrix fenestrations and their effect on breast shape. Eur J Plast Surg 2015; 38: 267-272
- 24 Cottler PS, Olenczak JB, Ning B. et al. Fenestration improves acellular dermal matrix biointegration: an investigation of revascularization with photoacoustic microscopy. Plast Reconstr Surg 2019; 143 (04) 971-981
- 25 Hoppe IC, Yueh JH, Wei CH, Ahuja NK, Patel PP, Datiashvili RO. Complications following expander/implant breast reconstruction utilizing acellular dermal matrix: a systematic review and meta-analysis. Eplasty 2011; 11: e40
- 26 Lee KT, Mun GH. Updated evidence of acellular dermal matrix use for implant-based breast reconstruction: a meta-analysis. Ann Surg Oncol 2016; 23 (02) 600-610
- 27 Kim JYS, Mlodinow AS. What's new in acellular dermal matrix and soft-tissue support for prosthetic breast reconstruction. Plast Reconstr Surg 2017; 140 (5S Advances in Breast Reconstruction): 30S-43S
- 28 Bank J, Phillips NA, Park JE, Song DH. Economic analysis and review of the literature on implant-based breast reconstruction with and without the use of the acellular dermal matrix. Aesthetic Plast Surg 2013; 37 (06) 1194-1201
- 29 Nahabedian MY. Acellular dermal matrices in primary breast reconstruction: principles, concepts, and indications. Plast Reconstr Surg 2012; 130 (5, Suppl 2): 44S-53S
- 30 Nahabedian MY. Prosthetic breast reconstruction with acellular dermal matrices: achieving predictability and reproducibility. Plast Reconstr Surg Glob Open 2016; 4 (05) e698