

RSS-Feed abonnieren
DOI: 10.1055/s-0042-1744427
Novel Three-Dimensional Knitted Fabric for Pressure Ulcer Prevention: Preliminary Clinical Application and Testing in a Diabetic Mouse Model of Pressure Ulcers
Autor*innen
Funding This work was supported by the R&D Program (S2097930) funded by the Small and Medium Business Administration (SMBA, Korea).
Abstract
Background Population aging has led to an increased incidence of pressure ulcers, resulting in a social burden and economic costs. We developed a three-dimensional knitted fabric (3-DKF) with a pressure-reducing function that can be applied topically in the early stages of pressure ulcers to prevent progression.
Methods We evaluated the effects of the 3-DKF in a streptozotocin-induced diabetes mellitus pressure ulcer mouse model, and the fabric was preliminarily applied to patients. Twelve-week-old male C57BL/6 mice were used for the animal experiments. In the pressure ulcer mouse model, an ischemia-reperfusion injury was created using a magnet on the dorsa of the mice. Pressure was measured with BodiTrak before and after applying the 3-DKF to 14 patients at risk of sacral pressure ulcers.
Results In the 3-DKF-applied mice group, the ulcers were shallower and smaller than those in the control group. Compared with the mice in the control group, the 3-DKF group had lower platelet-derived growth factor-α and neutrophil elastase expression, as parameters related to inflammation, and increased levels of transforming growth factor (TGF)-β1, TGF-β3, proliferating cell nuclear antigen, and α-smooth muscle actin, which are related to growth factors and proliferation. Additionally, typical normal tissue staining patterns were observed in the 3-DKF group. In the preliminary clinical analysis, the average skin pressure was 26.2 mm Hg before applying the 3-DKF, but it decreased to an average of 23.4 mm Hg after 3-DKF application.
Conclusion This study demonstrated that the newly developed 3-DKF was effective in preventing pressure ulcers through testing in a pressure ulcer animal model and preliminary clinical application.
Pressure ulcers are chronic wounds that occur in a localized area subjected to continuous pressure and shearing force, typically involving the skin, subcutaneous fat, and muscle. The degree and duration of pressure are the main determinants of pressure ulcer severity. Thus, these ulcers occur mainly in bedridden patients in the intensive care unit and patients with spinal cord injuries.[1] The incidence of pressure ulcers is also increasing as more patients are diagnosed with diabetes mellitus (DM) and chronic kidney disease, two conditions known to increase the risk of pressure ulcers.[2] Pressure ulcers, in turn, seriously affect patients' quality of life and survival rates and pose a major economic burden, as the costs of pressure ulcer treatment and extended hospital stays are high.
Various strategies and protocols have been developed to prevent pressure ulcers.[3] [4] [5] [6] Regardless of the specific method, the prevention of pressure ulcers is primarily aimed at reducing the cause of the pressure.
Among the dressing materials developed to date, studies have shown that a five-layer soft silicone bordered dressing is effective for pressure ulcer prevention.[7] However, using this type of dressing imposes a substantial cost burden, and it is difficult to conclude that any wound dressing is effective for pressure ulcers.[8]
The authors developed a three-dimensional knitted fabric (3-DKF) with a pressure-reducing function that could be applied topically in the early stages of pressure ulcers to prevent progression. We further evaluated the effect of the 3-DKF in a streptozotocin (STZ)-induced DM pressure ulcer mouse model and preliminarily applied the 3-DKF to patients.
Methods
Animal Experiments
Male C57BL/6 mice (11 weeks of age) were allowed to acclimate for 1 week in an animal room with a 12-hour light/dark cycle and ad libitum access to water and food. The animal experimental protocols were approved by the Animal Experiments Ethics Committee of our hospital (approval number: KM-2015–4R1) and complied with the Guide for the Care and Use of Laboratory Animals of our hospital.
Induction of Diabetes in Mice by STZ
Twelve-week-old mice were fasted for 4 hours and injected intraperitoneally with STZ (50 mg/kg body weight; Sigma-Aldrich, St. Louis, MO) dissolved in 100 mM sodium citrate buffer (pH 4.5) for 5 days consecutively ([Fig. 1]). Blood glucose levels were monitored via the tail vein for 4 weeks. The mice were considered to have diabetes when their blood glucose levels exceeded 250 mg/dL on two consecutive measurements.

Development of the 3-DKF
The 3-DKF had a three-dimensional knitted structure. Threads were placed between the upper and lower layers to connect them, thereby dispersing the pressure. These threads formed the thickness of the cushion fabric and were knitted in various directions, allowing the fabric to absorb pressure effectively. The connecting threads between the layers were designed to form an air-permeating layer. Therefore, the fabric was crafted to adapt its form to fit the curved areas of the body. In addition, the fabric had a mesh, allowing air to pass through the material, and the threads were antimicrobial to prevent infection. The yarn was made by spinning synthetic zeolite and the master batch at a 10:90 ratio. This zeolite-based EVERVACC yarn contained 1% of an antibacterial substance and showed 99.9% antibacterial effectiveness (KS K 0693: 2011) against Staphylococcus aureus and Pneumococcus. To impart bulkiness to the fibers of the woven fabric, we used draw-textured yarn (DTY). Finally, polyester DTY 150 denier (d)/48 filament semi-dull was used. The fibers' characteristics were as follows: fiber size, 118.76 days; cutting intensity, 2.03 gf/d; and fiber elasticity, 119.04%. With standardized measurements, the 3-DKF had a moisture vapor transmission rate of 2,404 g/m2/24 h, antibacterial activity of 99.9%, a wear time of over 24 hours, an absorption time of 1 second, an absorption rate greater than 120%, and air permeability greater than 1,977.6 cm3/cm2/s ([Fig. 2]).

Pressure Ulcer Mouse Model of Ischemia-Reperfusion Injury Made Using a Magnet
The mice were anesthetized using Zoletil (30 mg/kg, tiletamine and zolazepam; Virbac, Corros, France) and Rompun (10 mg/kg, xylazine; Bayer, Leverkusen, Germany), and the hair on the dorsa was shaved. The dorsal skin was gently elevated and placed between a pair of magnets (12 mm in diameter and 5 mm thick) which were applied for 5 hours over two consecutive days and removed to induce an ischemia-reperfusion (IR) injury.[9] The IR cycles were performed twice for ulcer formation. The 3-DKF was applied between the skin and magnet during the IR cycle for ulcer formation in the experimental group. The 3-DKF used in the animal experiment was square-shaped, 6-mm thick, and slightly larger than the 12 × 5 mm circular magnet ([Fig. 1]). After removal of the magnets, the mice were individually housed. All mice developed two ulcers. The day when the magnets were removed was designated as day 0, and photographs were made of the healing wounds on days 1, 3, 5, and 7. Ulcer tissues were sampled on days 3 and 7 under anesthesia using Zoletil and Rompun and used for Western blot analyses and immunohistochemical (IHC) staining.
Ulcer Wound Analysis
Digital photographs were acquired on days 1, 3, 5, and 7. Ulcer closure was defined as the time when complete reepithelization of the wound was observed. The ulcer wound area was quantified using ImageJ software (National Institutes of Health, Bethesda, MD; http://rsb.info.nih.gov/ij/download.html).
Hematoxylin-Eosin and IHC Staining
After the mice were euthanized, skin samples were harvested, fixed in 10% formalin solution, and embedded in paraffin. Hematoxylin-eosin (H&E) and IHC staining were performed using standard protocols with 5-μm-thick sections of the skin wounds. For IHC staining, deparaffinized sections were incubated with the following antibodies: mouse anti-α-smooth muscle actin (α-SMA; 1:1,000; Sigma-Aldrich), rat anti-neutrophil elastase (1:200; Abcam, Cambridge, UK), and mouse anti-proliferating cell nuclear antigen (PCNA; 1:800, Abcam). The primary antibodies were detected using horseradish peroxidase (HRP)-conjugated anti-mouse or anti-rat immunoglobulin G (IgG) (EnVision+ System; Dako, Glostrup, Denmark) and 3,3′-diaminobenzidine substrate as a chromogen, yielding a brown precipitate at the reaction site.
Western Blotting
Protein from the skin tissues was homogenized in radioimmunoprecipitation assay lysis buffer (50 mM Tris, 150 mM NaCl, 1 mM ethylenediaminetetraacetic acid, 0.5% sodium deoxycholate, 0.1% sodium dodecyl sulfate, and 1% NP-40, pH 7.4) with a protease inhibitor cocktail (GenDEPOT, Barker, TX), 10 mM NaF, and 1 mM Na3VaO4. Proteins from the skin lysates were loaded onto 10 or 12% polyacrylamide gels and separated by sodium dodecyl sulfate–polyacrylamide gel electrophoresis, followed by transfer to polyvinylidene difluoride membranes (GE Healthcare, Princeton, NJ). After transfer, the membranes were blocked with 5% nonfat milk and then incubated with specific primary antibodies, as follows: rabbit anti-transforming growth factor (TGF)-β1 antibodies (1:500; Abcam), rabbit anti-TGF-β3 antibodies (1:500; Abcam), rabbit anti-platelet-derived growth factor (PDGF)-α antibodies (1:500; Santa Cruz Biotechnology, Dallas, TX), mouse anti-PCNA antibodies (1:1,000; Abcam), rabbit anti-vascular endothelial growth factor (VEGF) antibodies (1:1,000; Abcam), goat anti-neutrophil elastase antibodies (1:500; Santa Cruz Biotechnology), mouse anti-α-SMA antibodies (1:5,000; Sigma-Aldrich), and mouse anti-β-actin antibodies (1:10,000; Sigma-Aldrich). The membranes were then stained with HRP-conjugated goat anti-rabbit IgG, goat anti-mouse IgG, and donkey anti-goat IgG secondary antibodies (1:2,000 to 1:10,000; Santa Cruz Biotechnology) and detected using ECL Prime Western blotting detection reagent (GE Healthcare).
Preliminary Clinical Application
A clinical study was conducted to determine whether the 3-DKF had a pressure-relieving effect in patients with early pressure ulcers. The Institutional Review Board at our hospital reviewed and approved this study (DSMC-2014–08–013). The patients included in the study were those at risk of pressure ulcers. The Braden scale was used as evaluation criteria and all patients were determined to be at risk of sacral pressure ulcers.[10] BodiTrak (Vista Medical, Winnipeg, Canada) was used for pressure mapping and measurements. The pressure was measured before and after the application of the 3-DKF for a comparative analysis. The 3-DKF attached to the sacral area was 8-mm thick and covered with Coolmax fabric to minimize damage due to direct skin contact ([Fig. 3]).

Statistical Analysis
All animal experimental values are expressed as the mean and standard error of the mean. The statistical analyses were performed using the unpaired Student's t-test. Differences with p-values of less than 0.05 were considered statistically significant. All analyses were performed using Prism 4.0 (GraphPad Software, San Diego, CA). For the statistical analysis of the preliminary clinical test, the Student's t-test (R stats package, version 3.6.3) was used.
Results
Effects of the 3-DKF on Pressure Ulcer Prevention in a Streptozotocin-Induced Diabetic Mouse Model
After removing the magnets, pressure ulcer-like wounds appeared on the skin of the mice within 3 days, and the depth of the ulcers stabilized after 5 days. The wounds in the 3-DKF group were smaller and shallower than those in the control group. There were slight differences between the mice. However, the size of the ulcers in the control group was similar to that of the magnet, and the ulcers reached the deep dermal layer ([Fig. 4A]). When the size of the ulcers in the control group on day 1 was set to 100%, the size of the ulcers in the 3-DKF group was only 25% ([Fig. 4B]). Some mice in the 3-DKF group did not have any ulcers or had ulcers with a depth equal only to the superficial dermis (i.e., shallower than that of the control group). On day 7, no noticeable improvement was observed in either group, suggesting that wound recovery may have been delayed due to diabetes.

Analysis of Tissue Protection Effects by H&E Staining
Skin biopsies were performed on the pressure ulcer sites on days 3 and 7. In the 3-DKF group, serum crust and partial epidermal necrosis were observed on day 3, and most hair follicles were well preserved. However, the dermal layer had collapsed, the hair follicles were destroyed, and red blood cell extravasation and necrosis were observed in the entire epidermis in the control group ([Fig. 5]). On day 7, the skin appendage was maintained, and the normal skin structure was also maintained overall in the 3-DKF group. In contrast, the control group still exhibited hemorrhagic crust and ulcers, and the follicles were completely destroyed.

Analysis of Variation in Wound Healing-Related Components by Western Blotting
To examine the differences in various factors related to the wound healing of pressure ulcers between the 3-DKF and control groups, the expression levels of cytokines and growth factors were analyzed by Western blots on day 3 after ulcer formation ([Fig. 6]). The TGF-β1 and TGF-β3 expression levels were higher in the 3-DKF group than in the control group. PDGF-α was upregulated in the control group compared with the 3-DKF group. These data suggest that the ulcers were deeper and that the platelets were more strongly affected by dermal hemorrhage. Notably, VEGF expression was not different between the groups. Moreover, although PCNA and α-SMA were upregulated, and neutrophil elastase was downregulated in the 3-DKF group compared with the control group, these differences were not statistically significant.

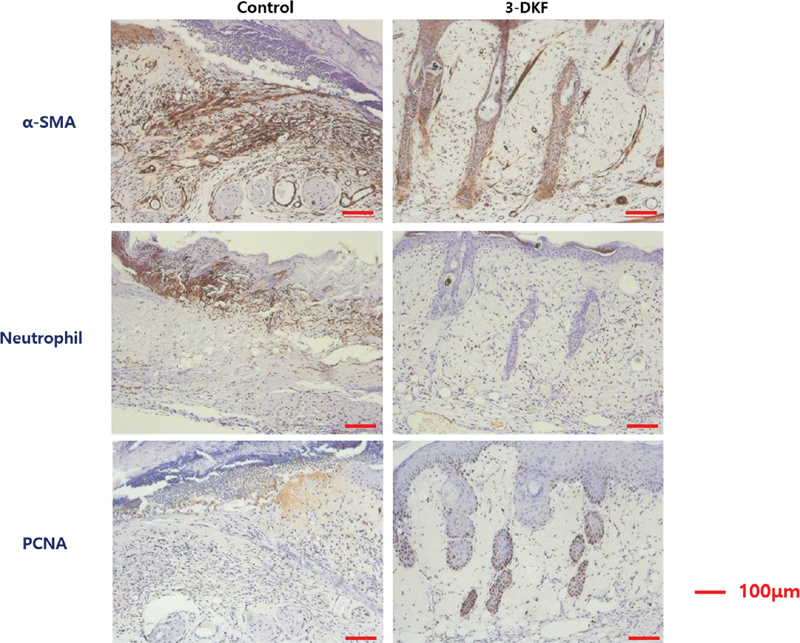
IHC Staining of Wound Contraction, Inflammation, and Proliferation
The expression of α-SMA, neutrophil elastase, and PCNA are associated with wound contraction, inflammation, and proliferation, which are related to the healing of pressure ulcers. On day 7, IHC analysis revealed that α-SMA was evenly expressed throughout the upper dermis of the specimens from the control group ([Fig. 7]). In contrast, in the 3-DKF group, staining was only observed in some areas around the adnexa, including the hair follicles and vessels that normally express α-SMA. It is thought that α-SMA was expressed in the overall ulcer area, since wound contraction occurred on day 7 after ulcer formation in the control group. The neutrophil elastase staining became stronger as inflammation increased in the control group. In contrast, PCNA was more thoroughly and evenly stained in the 3-DKF group, in which the basal layer was better preserved, because PCNA usually stains the basal cell layer of hair follicles, where mitosis occurs.
Clinical Pressure Mapping Results
The 3-DKF was applied to all 14 patients. The average age of the patients was 66.4 years, their average body mass index was 23.6 kg/m2, and their average score on the Braden scale was 17.6 points ([Table 1]). In the pressure mapping analysis, the average was 26.2 mm Hg before applying the 3-DKF, but it decreased to an average of 23.4 mm Hg after application ([Fig. 8]). Therefore, there was a pressure-decreasing effect of 2.80 mm Hg on average. This difference was statistically significant (p < 0.001).
Abbreviation: BMI, body mass index.

Discussion
Pressure ulcers are chronic wounds requiring extended treatment. In bedridden patients, if the pressure is not adequately reduced in stage 1 ulcers, the ulcers will develop into stage 2 to 3 ulcers, resulting in extended hospitalization and increased medical costs. Therefore, various strategies have been implemented for preventing pressure ulcers, including alternating pressure mattresses, air suspension beds, nutritional treatment, and repositioning.[11] In this study, we present an alternative approach using the 3-DKF to prevent pressure ulcers and examined the effects of this 3-DKF on pressure reduction.
In normal mice, epithelization is completed in approximately 14 days. However, in our diabetic mouse model, epithelialization required a total of 21 days (data not shown), resulting in delayed wound healing similar to the clinical state of patients with pressure ulcers. Owing to the specific weaving patterns of the layers in the 3-DKF, the 3-DKF appeared to absorb the pressure created by the magnet, thereby decreasing the size and depth of the ulcers. Thus, the 3-DKF acted as a buffering material, creating a thick cushion for shock absorption. Moreover, in addition to reducing the size and depth of the pressure ulcers, the 3-DKF also maintained intact hair follicles and epidermis, and the crust that formed on the wound was focal. In contrast, H&E and IHC analyses showed that the ulcers in the control group were larger and exhibited more severe inflammation.
TGF-β1 has been shown to have various effects on wound healing.[12] For example, TGF-β1 is upregulated in the early stages of wound healing, stimulating neutrophil, endothelial cell, and fibroblast infiltration. Moreover, TGF-β1 induces α-SMA expression, thereby stimulating wound contraction, and is important for the formation of the extracellular matrix, including collagen.[12] However, if excessive inflammation is present, TGF-β1 functions as a negative regulator of reepithelization, and wound healing is delayed.[12] Therefore, the upregulation of this factor is beneficial for wound healing during the initial state of an injury. TGF-β3 stimulates the migration of epidermal keratinocytes in injured skin and suppresses the migration of dermal fibroblasts and endothelial cells.[13] Interestingly, in chronic wounds, TGF-β isoforms are downregulated owing to degranulation by neutrophil elastase.[14] Accordingly, our results suggest that lesions in the 3-DKF group could undergo a rapid wound healing process due to the upregulation of TGF-β1 and TGF-β3.[15] Additionally, TGF-β, which is normally expressed at relatively high levels, was downregulated due to the increase in neutrophil elastase in the larger wounds in the control group. This downregulation may have influenced the speed of wound healing. PDGF, which is secreted from platelet α-granules during platelet aggregation in hemostasis, recruits a variety of inflammatory cells, including neutrophils, macrophages, and fibroblasts. Interestingly, increased ulcer size was associated with greater levels of PDGF secretion, which could explain the results observed in the control group.
VEGF induces wound healing by stimulating angiogenesis through endothelial cell migration and proliferation.[16] Reduced expression of VEGF would be expected to delay wound healing in cases of chronic pressure ulcers. One study showed that the topical application of recombinant human VEGF was effective for enhancing wound healing.[17] However, in our study, no differences in VEGF expression were observed according to the size of the ulcers. This likely was because VEGF is produced by many cell types, including macrophages, platelets, and keratinocytes,[14] and the 3-DKF group exhibited ample keratinocytes, whereas the control group exhibited ample inflammatory cells, including macrophages and platelets.
PCNA is expressed in the S-phase of the cell cycle and plays an essential role in the repair of damaged deoxyribonucleic acid.[18] [19] Consistent with this, PCNA was highly expressed in the basal layer and hair follicles in the 3-DKF group, with moderate expression in the tissues where proliferation typically occurs. Additionally, α-SMA is normally expressed in the walls of blood vessels and in the skin adnexa and stimulates wound healing by enhancing wound contraction by myofibroblasts.[19] [20] In this study, mice in the 3-DKF group exhibited small wounds with normal staining patterns. However, diabetic wounds usually recover through granulation rather than wound contraction, and staining over the entire ulcer region is thought to be associated with the destruction of hair follicles.[19] Lastly, neutrophil elastase was expressed at higher levels in the control group and appeared to be correlated with inflammation according to the size and depth of the ulcers.
The newly invented 3-DKF that was analyzed in this study relieved pressure, thereby reducing the size and depth of pressure ulcers. In the 3-DKF mice group, growth factor-, inflammation-, and proliferation-related molecules associated with wound healing were expressed at levels similar to those in normal tissues. Thus, it will be important to ensure adequate pressure absorption to maintain the normal state of tissues because of delays in wound healing in the diabetic state.
The 14 patients to whom the 3-DKF was preliminarily applied to reduce pressure had no side effects, such as discomfort, a skin tone change, or itching. The 3-DKF should be applied to more patients to confirm its effectiveness, but it showed considerable potential and could be applied to patients at risk of pressure ulcers in a variety of ways. It is expected that the 3-DKF can be applied to a variety of areas under pressure by forming it into various shapes, such as diapers, small mattresses, hats, socks, and underwear. Another advantage of the newly developed 3-DKF is that it is not expensive. Many patients worldwide living out their lives in nursing homes suffer from bedsores, which motivated the authors to develop this product.
In this study, we developed a novel 3-DKF and evaluated the effect of this fabric in a STZ-induced mouse model of diabetes. In the 3-DKF application group, the depth and area of the ulcers were reduced compared with those in the control group, and lower tissue expression of proteins related to inflammation and higher levels of findings related to growth factors, wound contraction, and proliferation were seen in the 3-DKF group than in the control group. The authors found that the 3-DKF reduced pressure in patients through a preliminary clinical application. Thus, the study showed that the newly developed 3-DKF was effective in preventing pressure ulcers through animal testing and preliminary clinical application.
Conflict of Interest
None declared.
Author Contributions
S.K. analyzed and interpreted the data and wrote the manuscript. J.H. collected the data and revised the manuscript. Y.L. designed and manufactured the experimental material. D.S. conceived the study, provided the experimental design, and supervised the entire drafting and revision process of the manuscript.
Ethical Approval
The animal experimental protocols were approved by the Animal Experiments Ethics Committee of Keimyung University School of Medicine (approval number: KM-2015–4R1) and complied with the Guide for Care and Use of Laboratory Animals of Keimyung University School of Medicine.
-
References
- 1 Demarré L, Van Lancker A, Van Hecke A. et al. The cost of prevention and treatment of pressure ulcers: a systematic review. Int J Nurs Stud 2015; 52 (11) 1754-1774
- 2 Frankel H, Sperry J, Kaplan L. Risk factors for pressure ulcer development in a best practice surgical intensive care unit. Am Surg 2007; 73 (12) 1215-1217
- 3 Yokoseki T, Kobayashi T, Nishizawa M. Use of a specially designed air-mat for the prevention of decubitus ulcer [in Japanese]. Kango Gijutsu 1977; 23 (08) 57-63
- 4 Mita K, Akataki K, Itoh K, Yoshida M, Shinoda T, Ishida Y. Physical characteristics of a new synthetic fiber mattress in relation to pressure sores. Front Med Biol Eng 1997; 8 (03) 221-230
- 5 Stuque AG, Sasaki VDM, da Silva Teles AA. et al. Protocolo para prevenção de úlcera por pressão. Revista da Rede de Enfermagem do Nordeste 2017; 18: 272-282
- 6 Wilborn D, Halfens R, Dassen T. Pressure ulcer: prevention protocols and prevalence. J Eval Clin Pract 2006; 12 (06) 630-638
- 7 Black J, Clark M, Dealey C. et al. Dressings as an adjunct to pressure ulcer prevention: consensus panel recommendations. Int Wound J 2015; 12 (04) 484-488
- 8 Clark M, Black J, Alves P. et al. Systematic review of the use of prophylactic dressings in the prevention of pressure ulcers. Int Wound J 2014; 11 (05) 460-471
- 9 Stadler I, Zhang R-Y, Oskoui P, Whittaker MS, Lanzafame RJ. Development of a simple, noninvasive, clinically relevant model of pressure ulcers in the mouse. J Invest Surg 2004; 17 (04) 221-227
- 10 Bergstrom N, Demuth PJ, Braden BJ. A clinical trial of the Braden scale for predicting pressure sore risk. Nurs Clin North Am 1987; 22 (02) 417-428
- 11 Medical Advisory Secretariat. Pressure ulcer prevention: an evidence-based analysis. Ont Health Technol Assess Ser 2009; 9 (02) 1-104
- 12 Wang X-J, Han G, Owens P, Siddiqui Y, Li AG. Role of TGF beta-mediated inflammation in cutaneous wound healing. J Investig Dermatol Symp Proc 2006; 11 (01) 112-117
- 13 Bandyopadhyay B, Fan J, Guan S. et al. A “traffic control” role for TGFbeta3: orchestrating dermal and epidermal cell motility during wound healing. J Cell Biol 2006; 172 (07) 1093-1105
- 14 Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen 2008; 16 (05) 585-601
- 15 Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res 2009; 37 (05) 1528-1542
- 16 Barrientos S, Brem H, Stojadinovic O, Tomic-Canic M. Clinical application of growth factors and cytokines in wound healing. Wound Repair Regen 2014; 22 (05) 569-578
- 17 Hanft JR, Pollak RA, Barbul A. et al. Phase I trial on the safety of topical rhVEGF on chronic neuropathic diabetic foot ulcers. J Wound Care 2008; 17 (01) 30-32
- 18 Mailand N, Gibbs-Seymour I, Bekker-Jensen S. Regulation of PCNA-protein interactions for genome stability. Nat Rev Mol Cell Biol 2013; 14 (05) 269-282
- 19 Bazrafshan A, Owji M, Yazdani M, Varedi M. Activation of mitosis and angiogenesis in diabetes-impaired wound healing by processed human amniotic fluid. J Surg Res 2014; 188 (02) 545-552
- 20 Darby I, Skalli O, Gabbiani G. Alpha-smooth muscle actin is transiently expressed by myofibroblasts during experimental wound healing. Lab Invest 1990; 63 (01) 21-29
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
06. April 2022
© 2022. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Demarré L, Van Lancker A, Van Hecke A. et al. The cost of prevention and treatment of pressure ulcers: a systematic review. Int J Nurs Stud 2015; 52 (11) 1754-1774
- 2 Frankel H, Sperry J, Kaplan L. Risk factors for pressure ulcer development in a best practice surgical intensive care unit. Am Surg 2007; 73 (12) 1215-1217
- 3 Yokoseki T, Kobayashi T, Nishizawa M. Use of a specially designed air-mat for the prevention of decubitus ulcer [in Japanese]. Kango Gijutsu 1977; 23 (08) 57-63
- 4 Mita K, Akataki K, Itoh K, Yoshida M, Shinoda T, Ishida Y. Physical characteristics of a new synthetic fiber mattress in relation to pressure sores. Front Med Biol Eng 1997; 8 (03) 221-230
- 5 Stuque AG, Sasaki VDM, da Silva Teles AA. et al. Protocolo para prevenção de úlcera por pressão. Revista da Rede de Enfermagem do Nordeste 2017; 18: 272-282
- 6 Wilborn D, Halfens R, Dassen T. Pressure ulcer: prevention protocols and prevalence. J Eval Clin Pract 2006; 12 (06) 630-638
- 7 Black J, Clark M, Dealey C. et al. Dressings as an adjunct to pressure ulcer prevention: consensus panel recommendations. Int Wound J 2015; 12 (04) 484-488
- 8 Clark M, Black J, Alves P. et al. Systematic review of the use of prophylactic dressings in the prevention of pressure ulcers. Int Wound J 2014; 11 (05) 460-471
- 9 Stadler I, Zhang R-Y, Oskoui P, Whittaker MS, Lanzafame RJ. Development of a simple, noninvasive, clinically relevant model of pressure ulcers in the mouse. J Invest Surg 2004; 17 (04) 221-227
- 10 Bergstrom N, Demuth PJ, Braden BJ. A clinical trial of the Braden scale for predicting pressure sore risk. Nurs Clin North Am 1987; 22 (02) 417-428
- 11 Medical Advisory Secretariat. Pressure ulcer prevention: an evidence-based analysis. Ont Health Technol Assess Ser 2009; 9 (02) 1-104
- 12 Wang X-J, Han G, Owens P, Siddiqui Y, Li AG. Role of TGF beta-mediated inflammation in cutaneous wound healing. J Investig Dermatol Symp Proc 2006; 11 (01) 112-117
- 13 Bandyopadhyay B, Fan J, Guan S. et al. A “traffic control” role for TGFbeta3: orchestrating dermal and epidermal cell motility during wound healing. J Cell Biol 2006; 172 (07) 1093-1105
- 14 Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen 2008; 16 (05) 585-601
- 15 Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res 2009; 37 (05) 1528-1542
- 16 Barrientos S, Brem H, Stojadinovic O, Tomic-Canic M. Clinical application of growth factors and cytokines in wound healing. Wound Repair Regen 2014; 22 (05) 569-578
- 17 Hanft JR, Pollak RA, Barbul A. et al. Phase I trial on the safety of topical rhVEGF on chronic neuropathic diabetic foot ulcers. J Wound Care 2008; 17 (01) 30-32
- 18 Mailand N, Gibbs-Seymour I, Bekker-Jensen S. Regulation of PCNA-protein interactions for genome stability. Nat Rev Mol Cell Biol 2013; 14 (05) 269-282
- 19 Bazrafshan A, Owji M, Yazdani M, Varedi M. Activation of mitosis and angiogenesis in diabetes-impaired wound healing by processed human amniotic fluid. J Surg Res 2014; 188 (02) 545-552
- 20 Darby I, Skalli O, Gabbiani G. Alpha-smooth muscle actin is transiently expressed by myofibroblasts during experimental wound healing. Lab Invest 1990; 63 (01) 21-29