

Subscribe to RSS
DOI: 10.1055/s-0042-1750012
18F-Fluorodeoxy Glucose and 11C-Methionine Accumulation in Demyelinating Lesions
Authors
Funding None.


Abstract
Background Few studies have evaluated the accumulation of 18F-fluorodeoxyglucose (FDG), 11C-methionine (MET), and other positron emission tomography (PET) tracers in patients with demyelinating disease.
Purpose This study aimed to investigate the accumulation of FDG-PET/computed tomography (CT) and MET-PET/CT in demyelinating lesions.
Material and Methods A retrospective search of the patient database in our hospital identified five patients with demyelinating disease in whom PET studies performed in the past 10 years revealed accumulation of FDG or MET. The clinical diagnoses were multiple sclerosis (n=1), myelitis (n=1), limbic encephalitis (n=1), chronic inflammatory demyelinating polyneuropathy (CIDP; n=1), and acute demyelinating encephalomyelitis (ADEM; n=1). Two patients received FDG-PET/CT alone and three patients received both FDG-PET/CT and MET-PET/CT on the same day. Images were visually and conjointly reviewed by two radiologists. In semiquantitative evaluation, the maximum standardized uptake value (SUVmax) of the lesion was measured. The lesion-to-normal brain uptake ratio (L/N ratio) was calculated.
Results FDG and/or MET accumulated to a part of the lesions seen on MRI. SUVmax on FDG-PET/CT ranged from 3.8 to 10.3, and L/N ratio on MET-PET/CT ranged from 16.6 to 2.4.
Conclusion It has been established that neoplastic and demyelinating lesions can be differentiated on the basis of FDG or MET uptake. However, as accumulation of FDG and MET can also occur in demyelinating lesions; knowledge of this possibility is of clinical importance.
Introduction
18F-fluorodeoxyglucose (FDG), the most available tracer for positron emission tomography (PET), has been used to diagnose various neoplastic diseases and to evaluate therapeutic response in these patients.[1] [2] 11C-methionine (MET) has also been widely used for imaging tumors in the brain and skull base.[3] [4] MET is particularly useful for diagnosing radiation necrosis of the brain.[5]
Tumefactive multiple sclerosis (MS)[6] exhibits large demyelinating plaques with or without contrast enhancement on MRI that resemble brain tumors. The feasibility of PET using FDG, MET, and other tracers to differentiate between neoplastic and demyelinating diseases has been reported.[7] [8] [9] [10] [11] However, few studies have evaluated the accumulation of FDG, MET, and other PET tracers in patients with demyelinating disease.[12] [13] [14] In the present study, we discuss the imaging features of demyelinating disease with regard to uptake of FDG or MET in demyelinating lesions and provide a literature review.
Material and Methods
Patients
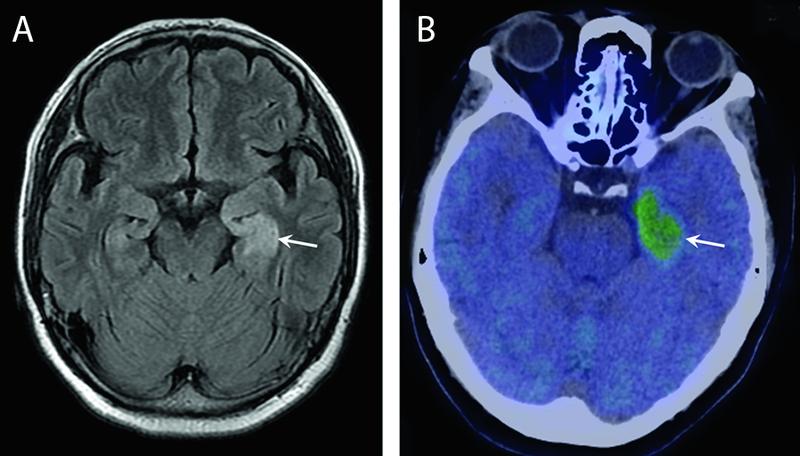
The Institutional Review Board of our hospital approved this study. A retrospective search of the patient database in our hospital identified five patients with demyelinating disease in whom PET studies performed in the past 10 years revealed accumulation of FDG or MET. There were two males and three females with age range of 40 to 63 years. The clinical diagnoses were multiple sclerosis (n=1), myelitis (n=1), limbic encephalitis (n=1), chronic inflammatory demyelinating polyneuropathy (CIDP; n=1), and acute demyelinating encephalomyelitis (ADEM; n=1; [Table 1]). The imaging diagnoses were as follows: cervical spinal cord lesion in case 1 ([Fig. 1]), CIDP with diffuse swelling of the bilateral nerve roots of the brachial plexus in case 2 ([Fig. 2]), right thalamic lesion in case 3 ([Fig. 3]), multiple lesions in the bilateral cerebral white matter in case 4 ([Fig. 4]), and a lesion in the left uncus and parahippocampal gyrus in case 5 who also had carcinoma of the lung ([Fig. 5]). All clinical diagnoses were made by a neurologist (C.K.) with 20 years' experience in neurology and were made based on the clinical manifestations and course (all cases), results of cerebrospinal fluid analysis (cases 1, 2, 4, and 5), nerve conduction velocity (case 2), and presence of malignancy (case 5; [Table 1]).
Abbreviations: ADEM, acute disseminated encephalomyelitis; CIDP, chronic inflammatory polyneuritis; CSF, cerebrospinal fluid; FDG, F-18 fluorodeoxy glucose; GABAbR, γ-ami-nobutyric acid-B receptor; L/N ratio, lesion-to-normal area ratio; MBP; myelin basic protein; MET, C-11 methionine; MS, multiple sclerosis; PET, positron emission tomography; rt., right; SUVmax, maximum standardized uptake value.




Positron Emission Tomography/Computed Tomography
PET/CT was performed using three different PET/CT units: GE Discovery 600 Motion (GE Healthcare, Milwaukee, Wisconsin), FWHM 5.1-mm, and 16-row CT in two patients (cases 1 and 2). GE Discovery 610 Motion (GE Healthcare), FWHM 5.1-mm, and 16-row CT in 1 patient (case 3); and GE IQ (GE Healthcare), FWHM 5.1-mm, and 16-row CT in two patients (cases 4 and 5). No intravenous contrast material was used. After CT, MET-PET was performed 20minutes after injecting MET. For FDG-PET, FDG was injected 60minutes after MET-PET, and FDG-PET was performed 60minutes after injection of FDG.
Two patients (cases 2 and 5) received FDG-PET alone, and three patients (cases 1, 3, and 4) received both FDG-PET/CT and MET-PET/CT on the same day. The protocol used in the PET/CT examinations has been described previously.[15] Coregistered images were displayed on a workstation (Advantage Workstation version 4.7, GE Healthcare).
Images were visually and conjointly reviewed by two radiologists (N.T. with 39 years' experience in neuroradiology and T.S. with 30 years' experience in radiology) who were aware of the clinical diagnoses.
In semiquantitative evaluation, the maximum standardized uptake value (SUVmax) of the lesion was measured. The lesion-to-normal brain uptake ratio (L/N ratio) was calculated as the SUVmax of the lesion divided by the SUVmax of the same site in the contralateral cerebral hemisphere.
Results
In case 1 (myelitis of the cervical spinal cord), there was obvious FDG accumulation in the lesion and MET accumulation was faint ([Fig. 1]). Case 2 (CIDP) showed FDG accumulation in some lesions ([Fig. 2]). In case 3 (suspected ADEM), FDG accumulation in the lesion in the right thalamus was equal to normal tissue, and there was obvious MET uptake in the lesion ([Fig. 3]). In Case 4 (MS), there was MET uptake but no FDG accumulation ([Fig. 4]). In case 5 (limbic encephalitis), there was FDG uptake in the lesion, and reduced FDG accumulation in normal tissue due to high blood glucose levels ([Fig. 5]). [Table 1] lists the SUVmax values and L/N ratios for MET-PET/CT in the five patients.
Discussion
FDG is the most widely available PET tracer worldwide. FDG hypermetabolism in the lesion generally suggests neoplastic etiology. It is known that accumulation of FDG in the central nervous system can indicate inflammatory diseases such as abscess, meningitis, and encephalitis.[16] [17] [18] Although the feasibility of FDG has been reported for differentiating between neoplasms and demyelinating diseases, the possibility of FDG uptake in demyelinating disease has also been reported.[19] [20] [21] [22] [23] [24] [25] [26] Our literature review revealed reports of FDG accumulation in limbic encephalitis,[12] [19] [21] [25] [26] active myelopathy,[13] progressive multifocal leukoencephalopathy,[14] [20] and MS.[22] [23] [24] In particular, FDG uptake by lesions has been often reported in limbic encephalitis, and it has been suggested that hypermetabolism of FDG in limbic encephalitis might be related to subclinical seizures.[19] A seizure occurred 5 days before the PET study in the present case 5.
The usefulness of MET for differentiating between neoplastic and nonneoplastic lesions has been reported[11]; however, there are several reports of MET accumulation in tumefactive demyelinating lesions.[27] [28] We found no reports of MET uptake in myelitis. In a semiquantitative analysis using L/N ratio to differentiate between tumefactive MS and high-grade glioma,[28] the L/N ratio in tumefactive MS was 1.89±0.55 which was significantly lower than that in high-grade astrocytoma (astrocytoma grade III: 3.37±1.36 and astrocytoma grade IV: 4.35±1.30). In the present study, L/N ratio of MET was less than 2.4 in cases 1, 3, and 4. Measurement of L/N ratio could be feasible in the case of MET accumulation in nonneoplastic lesions.
Previous studies have reported inflammatory cell infiltration as an important factor in brain abscess and encephalitis as a mechanism of FDG or MET accumulation in tumefactive MS.[24] [28] These mechanisms could also be important for FDG or MET accumulation in demyelinating lesions. In the present case 2, although the brachial plexus was diffusely affected on the MRI, FDG accumulated in the most thickened nerve root. Symptoms were strong in the right side with FDG uptake. However, the mechanism of partial high uptake of FDG is unclear. Our literature review found no mention of FDG uptake by CIDP lesions. In case 4, the lesion showed no contrast enhancement on MRI, no FDG accumulation, and slight uptake of MET in the biggest one in multiple lesions. Symptoms seemed related to the lesion with MET uptake. Although MET uptake was faint in case 1, there was clear FDG uptake. In case 3, FDG uptake in the lesion was equal to that in normal tissue, and there was obvious uptake of MET. The mechanisms of uptake are quite different between MET and FDG. MET uptake is influenced by MET metabolism and active MET transport.[28] Decreased uptake of MET after treatment has been reported in a case of progressive multifocal leukoencephalopathy.[14] Case 5 showed decreased uptake of FDG in the lesion on follow-up FDG-PET study. No follow-up PET studies were performed in other cases.
In tracers other than FDG and MET, 18F-fluoromethylcholine uptake has been reported in an MS lesion.[29] A recent study has shown a quantitative correlation of myelin histology with 18F-florbetapir binding in demyelinated lesions,[29] and the authors suggested the potential of 18F-florbetapir PET for quantitative assessment of the progression of demyelinating diseases.[30]
Limitations
There are several limitations in the present study. The number of cases was small. FDG and/or MET PET studies are usually not performed when demyelinating diseases are suspected. Although an experienced neurologist diagnosed every case according to the clinical symptoms, clinical course, radiological findings, and laboratory data, a pathological diagnosis was not obtained. In general, biopsy is not clinically practical in patients with demyelinating diseases. Patients with demyelinating disease without accumulation of FDG and/or MET were unclear in our patients database.
Conclusion
In conclusion, accumulation of FDG or MET was seen in patients with demyelinating diseases. Knowledge of the possibility of FDG and MET uptake in demyelinating lesions is of clinical importance.
Conflict of Interest
None declared.
-
References
- 1 Kostakoglu L, Agress Jr., H, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer. Radigraphics 2003; 23 (02) 315-340 , quiz 533
- 2 Kazama T, Faria SC, Varavithya V, Phongkitkarun S, Ito H, Macapinlac HA. FDG PET in the evaluation of treatment for lymphoma: clinical usefulness and pitfalls. Radiographics 2005; 25 (01) 191-207
- 3 Palanichamy K, Chakravarti A. Diagnostic and prognostic significance of methionine uptake and methionine positron emission tomography imaging in gliomas. Front Oncol 2017; 7: 257
- 4 Tomura N, Mizuno Y, Saginoya T. PET/CT findings for tumors in the base of the skull: Comparison of 18F-FDG with 11C-methionine. Acta Radiol 2016; 57: 325-332
- 5 Terakawa Y, Tsuyuguchi N, Iwai Y. et al. Diagnostic accuracy of 11C-methionine PET for differentiation of recurrent brain tumors from radiation necrosis after radiotherapy. J Nucl Med 2008; 49 (05) 694-699
- 6 Suh CH, Kim HS, Jung SC, Choi CG, Kim SJ. MRI findings in tumefactive demyelinating lesions: a systematic review and meta-analysis. AJNR Am J Neuroradiol 2018; 39 (09) 1643-1649
- 7 Takenaka S, Shinoda J, Asano Y. et al. Metabolic assessment of monofocal acute inflammatory demyelination using MR spectroscopy and (11)C-methionine-, (11)C-choline-, and (18)F-fluorodeoxyglucose-PET. Brain Tumor Pathol 2011; 28 (03) 229-238
- 8 Kim JE, Choi KG, Jeong JH, Kang HJ, Kim HS. Diffuse cortical hypometabolism on (18)F-FDG-PET scan in a case of an adult variant cerebello-brainstem dominant form of ALD manifesting dementia. Parkinsonism Relat Disord 2012; 18 (02) 210-212
- 9 Dolic K, Bilic I, Buca A, Radovic D, Titlic M. differentiation of tumefactive demyelinating lesions from metastatic brain disease with FDG-PET-CT: A case report. J Mult Scler (Foster City) 2014; 1: 1-3
- 10 Abdoli M, Freedman MS. Neuro-oncology dilemma: tumour or tumefactive demyelinating lesion. Mult Scler Relat Disord 2015; 4 (06) 555-566
- 11 Ninomiya S, Hara M, Morita A. et al. Tumefactive demyelinating lesion differentiated from a brain tumor using a combination of magnetic resonance imaging and 11C-methionine positron emission tomography. Intern Med 2015; 54 (11) 1411-1414
- 12 Scheid R, Lincke T, Voltz R, von Cramon DY, Sabri O. Serial 18F-fluoro-2-deoxy-D-glucose positron emission tomography and magnetic resonance imaging of paraneoplastic limbic encephalitis. Arch Neurol 2004; 61 (11) 1785-1789
- 13 Flanagan EP, Hunt CH, Lowe V. et al. [(18)F]-fluorodeoxyglucose-positron emission tomography in patients with active myelopathy. Mayo Clin Proc 2013; 88 (11) 1204-1212
- 14 Shirai S, Yabe I, Kano T. et al. Usefulness of 11C-methionine-positron emission tomography for the diagnosis of progressive multifocal leukoencephalopathy. J Neurol 2014; 261 (12) 2314-2318
- 15 Tomura N, Ito Y, Matsuoka H. et al. PET findings of intramedullary tumors of the spinal cord using [18F] FDG and [11C] methionine. AJNR Am J Neuroradiol 2013; 34: 1278-1283
- 16 Rahman WT, Wale DJ, Viglianti BL. et al. The impact of infection and inflammation in oncologic 18F-FDG PET/CT imaging. Biomed Pharmacother 2019; 117: 109168
- 17 Rangan K, Ravina M, Yadav N, Suraj AS, Gambhir S. 18F-FDG PET/CT of tuberculosis meningitis and carotid pseudoaneurysm. Clin Nucl Med 2017; 42 (06) e304-e305
- 18 Lee BY, Newberg AB, Liebeskind DS, Kung J, Alavi A. FDG-PET findings in patients with suspected encephalitis. Clin Nucl Med 2004; 29 (10) 620-625
- 19 Kassubek J, Juengling FD, Nitzsche EU, Lücking CH. Limbic encephalitis investigated by 18FDG-PET and 3D MRI. J Neuroimaging 2001; 11 (01) 55-59
- 20 Mertens K, Acou M, Van den Broecke C. et al. Progressive multifocal leukoencephalopathy (PML) mimicking high-grade glioma on delayed F-18 FDG PET imaging. J Clin Neurosci 2012; 19 (08) 1167-1169
- 21 Masangkay N, Basu S, Moghbel M, Kwee T, Alavi A. Brain 18F-FDG-PET characteristics in patients with paraneoplastic neurological syndrome and its correlation with clinical and MRI findings. Nucl Med Commun 2014; 35 (10) 1038-1046
- 22 Maffione AM, Rampin L, Grassetto G, L'Erario R, Colletti PM, Rubello D. 18F-FDG PET/CT in tumefactive multiple sclerosis. Clin Nucl Med 2014; 39 (08) 750-751
- 23 Cózar Santiago MdelP, Sanchez Jurado R, Sanz Llorens R, Aguilar Barrios JE, Ferrer Rebolleda J. Limbic encephalitis diagnosed with 18F-FDG PET/CT. Clin Nucl Med 2016; 41 (02) e101-e103
- 24 Dong A, Gao M, Wang Y, Gao L, Zuo C. FDG PET/CT in acute tumefactive multiple sclerosis occurring in a case of chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Clin Nucl Med 2016; 41 (09) e414-e416
- 25 Moloney P, Boylan R, Elamin M, O'Riordan S, Killeen R, McGuigan C. Semi-quantitative analysis of cerebral FDG-PET reveals striatal hypermetabolism and normal cortical metabolism in a case of VGKCC limbic encephalitis. Neuroradiol J 2017; 30 (02) 160-163
- 26 Taneja S, Suri V, Ahuja A, Jena A. Simultaneous 18F-FDG PET/MRI in autoimmune limbic encephalitis. Indian J Nucl Med 2018; 33 (02) 174-176
- 27 Ishibashi K, Miura Y, Matsumura K. et al. PET imaging of 18F-FDG, 11C-methionine, 11C-fumazenil and 11C–4DST in progressive multifocal leukoencephalopathy. Intern Med 2017; 56 (10) 1219-1223
- 28 Hashimoto S, Inaji M, Nariai T. et al. Usefulness of [11C] methionine PET in the differentiation of tumefactive multiple sclerosis from high grade astrocytoma. Neurol Med Chir (Tokyo) 2019; 59 (05) 176-183
- 29 Bolcaen J, Acou M, Mertens K. et al. Structural and metabolic features of two different variants of multiple sclerosis: a PET/MRI study. J Neuroimaging 2013; 23 (03) 431-436
- 30 Zhang M, Liu J, Li B, Chen S. 18F-florbetapir PET/MRI for quantitatively monitoring demyelination and remyelination in acute disseminated encephalomyelitis. EJNMMI Res 2019; 9 (01) 96
Address for correspondence
Publication History
Article published online:
02 September 2022
© 2022. World Association of Radiopharmaceutical and Molecular Therapy (WARMTH). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Kostakoglu L, Agress Jr., H, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer. Radigraphics 2003; 23 (02) 315-340 , quiz 533
- 2 Kazama T, Faria SC, Varavithya V, Phongkitkarun S, Ito H, Macapinlac HA. FDG PET in the evaluation of treatment for lymphoma: clinical usefulness and pitfalls. Radiographics 2005; 25 (01) 191-207
- 3 Palanichamy K, Chakravarti A. Diagnostic and prognostic significance of methionine uptake and methionine positron emission tomography imaging in gliomas. Front Oncol 2017; 7: 257
- 4 Tomura N, Mizuno Y, Saginoya T. PET/CT findings for tumors in the base of the skull: Comparison of 18F-FDG with 11C-methionine. Acta Radiol 2016; 57: 325-332
- 5 Terakawa Y, Tsuyuguchi N, Iwai Y. et al. Diagnostic accuracy of 11C-methionine PET for differentiation of recurrent brain tumors from radiation necrosis after radiotherapy. J Nucl Med 2008; 49 (05) 694-699
- 6 Suh CH, Kim HS, Jung SC, Choi CG, Kim SJ. MRI findings in tumefactive demyelinating lesions: a systematic review and meta-analysis. AJNR Am J Neuroradiol 2018; 39 (09) 1643-1649
- 7 Takenaka S, Shinoda J, Asano Y. et al. Metabolic assessment of monofocal acute inflammatory demyelination using MR spectroscopy and (11)C-methionine-, (11)C-choline-, and (18)F-fluorodeoxyglucose-PET. Brain Tumor Pathol 2011; 28 (03) 229-238
- 8 Kim JE, Choi KG, Jeong JH, Kang HJ, Kim HS. Diffuse cortical hypometabolism on (18)F-FDG-PET scan in a case of an adult variant cerebello-brainstem dominant form of ALD manifesting dementia. Parkinsonism Relat Disord 2012; 18 (02) 210-212
- 9 Dolic K, Bilic I, Buca A, Radovic D, Titlic M. differentiation of tumefactive demyelinating lesions from metastatic brain disease with FDG-PET-CT: A case report. J Mult Scler (Foster City) 2014; 1: 1-3
- 10 Abdoli M, Freedman MS. Neuro-oncology dilemma: tumour or tumefactive demyelinating lesion. Mult Scler Relat Disord 2015; 4 (06) 555-566
- 11 Ninomiya S, Hara M, Morita A. et al. Tumefactive demyelinating lesion differentiated from a brain tumor using a combination of magnetic resonance imaging and 11C-methionine positron emission tomography. Intern Med 2015; 54 (11) 1411-1414
- 12 Scheid R, Lincke T, Voltz R, von Cramon DY, Sabri O. Serial 18F-fluoro-2-deoxy-D-glucose positron emission tomography and magnetic resonance imaging of paraneoplastic limbic encephalitis. Arch Neurol 2004; 61 (11) 1785-1789
- 13 Flanagan EP, Hunt CH, Lowe V. et al. [(18)F]-fluorodeoxyglucose-positron emission tomography in patients with active myelopathy. Mayo Clin Proc 2013; 88 (11) 1204-1212
- 14 Shirai S, Yabe I, Kano T. et al. Usefulness of 11C-methionine-positron emission tomography for the diagnosis of progressive multifocal leukoencephalopathy. J Neurol 2014; 261 (12) 2314-2318
- 15 Tomura N, Ito Y, Matsuoka H. et al. PET findings of intramedullary tumors of the spinal cord using [18F] FDG and [11C] methionine. AJNR Am J Neuroradiol 2013; 34: 1278-1283
- 16 Rahman WT, Wale DJ, Viglianti BL. et al. The impact of infection and inflammation in oncologic 18F-FDG PET/CT imaging. Biomed Pharmacother 2019; 117: 109168
- 17 Rangan K, Ravina M, Yadav N, Suraj AS, Gambhir S. 18F-FDG PET/CT of tuberculosis meningitis and carotid pseudoaneurysm. Clin Nucl Med 2017; 42 (06) e304-e305
- 18 Lee BY, Newberg AB, Liebeskind DS, Kung J, Alavi A. FDG-PET findings in patients with suspected encephalitis. Clin Nucl Med 2004; 29 (10) 620-625
- 19 Kassubek J, Juengling FD, Nitzsche EU, Lücking CH. Limbic encephalitis investigated by 18FDG-PET and 3D MRI. J Neuroimaging 2001; 11 (01) 55-59
- 20 Mertens K, Acou M, Van den Broecke C. et al. Progressive multifocal leukoencephalopathy (PML) mimicking high-grade glioma on delayed F-18 FDG PET imaging. J Clin Neurosci 2012; 19 (08) 1167-1169
- 21 Masangkay N, Basu S, Moghbel M, Kwee T, Alavi A. Brain 18F-FDG-PET characteristics in patients with paraneoplastic neurological syndrome and its correlation with clinical and MRI findings. Nucl Med Commun 2014; 35 (10) 1038-1046
- 22 Maffione AM, Rampin L, Grassetto G, L'Erario R, Colletti PM, Rubello D. 18F-FDG PET/CT in tumefactive multiple sclerosis. Clin Nucl Med 2014; 39 (08) 750-751
- 23 Cózar Santiago MdelP, Sanchez Jurado R, Sanz Llorens R, Aguilar Barrios JE, Ferrer Rebolleda J. Limbic encephalitis diagnosed with 18F-FDG PET/CT. Clin Nucl Med 2016; 41 (02) e101-e103
- 24 Dong A, Gao M, Wang Y, Gao L, Zuo C. FDG PET/CT in acute tumefactive multiple sclerosis occurring in a case of chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Clin Nucl Med 2016; 41 (09) e414-e416
- 25 Moloney P, Boylan R, Elamin M, O'Riordan S, Killeen R, McGuigan C. Semi-quantitative analysis of cerebral FDG-PET reveals striatal hypermetabolism and normal cortical metabolism in a case of VGKCC limbic encephalitis. Neuroradiol J 2017; 30 (02) 160-163
- 26 Taneja S, Suri V, Ahuja A, Jena A. Simultaneous 18F-FDG PET/MRI in autoimmune limbic encephalitis. Indian J Nucl Med 2018; 33 (02) 174-176
- 27 Ishibashi K, Miura Y, Matsumura K. et al. PET imaging of 18F-FDG, 11C-methionine, 11C-fumazenil and 11C–4DST in progressive multifocal leukoencephalopathy. Intern Med 2017; 56 (10) 1219-1223
- 28 Hashimoto S, Inaji M, Nariai T. et al. Usefulness of [11C] methionine PET in the differentiation of tumefactive multiple sclerosis from high grade astrocytoma. Neurol Med Chir (Tokyo) 2019; 59 (05) 176-183
- 29 Bolcaen J, Acou M, Mertens K. et al. Structural and metabolic features of two different variants of multiple sclerosis: a PET/MRI study. J Neuroimaging 2013; 23 (03) 431-436
- 30 Zhang M, Liu J, Li B, Chen S. 18F-florbetapir PET/MRI for quantitatively monitoring demyelination and remyelination in acute disseminated encephalomyelitis. EJNMMI Res 2019; 9 (01) 96