

Subscribe to RSS
DOI: 10.1055/s-0042-1750057
Avulsion of the Lateral Head of the Gastrocnemius in a Dog: Surgical Treatment and an Ex Vivo Study on Pathomechanisms
Authors
Funding None.

Abstract
A 6-year-old Border Collie presented with a 4-month history of progressive plantigrade stance of the right hindlimb, following a jump when chasing a ball. Avulsion of the lateral head of the gastrocnemius and tearing of the medial muscular belly were confirmed radiographically and ultrasonographically. Surgical repair of the lateral head was performed using two nylon mattress sutures placed around the fabella and through femoral condylar bone tunnels, followed by the application of a cranial half cast for 5 weeks. No complications were reported and follow-up owner's questionnaire at 18 months postoperatively revealed excellent results with the dog returning to normal activity.
Avulsion of the lateral fabella was induced in a cadaveric limb and hyperflexion of the tarsus was simulated. Extreme hyperflexion of the tarsus only occurred once a subsequent tear of the medial belly of the gastrocnemius had developed, but without avulsion of the medial fabella.
Introduction
Avulsion injuries affecting the origin of the gastrocnemius muscles are rare. Few reports are published regarding the surgical management of these lesions in dogs[1] [2] [3] [4] [5] [6] [7] [8] and cats[9] [10] ([Table 1]). Some of these reports are poorly detailed and lack follow-up data, giving surgeons scarce evidence on how to optimally treat these types of lesions.
|
Author |
Animal |
Onset/Lesion |
Presentation |
Treatment |
Immobilization method |
Complications |
Follow-up/outcome |
|---|---|---|---|---|---|---|---|
|
Chaffee and Knecht (1979)[1] |
7 yo Wirehaired Fox Terrier |
Trauma/Medial head |
NWB |
Cruciate mattress sutures with 2–0 wire in figure-of-eight around fabella |
MRJB (1 week) |
Not specified |
8 weeks—began to use limb |
|
Vaughan (1979)[2] |
5 yo Alsatian (45 kg) |
Trauma/Lateral head |
Not specified |
Sutured tendon around fabella + reinforcing sutures + carbon fibre augmentation |
External support (8 weeks) |
Not specified |
Months before satisfactory leg use |
|
Vaughan (1979)[2] |
7 yo Fox Terrier |
Trauma/Medial head |
Not specified |
Sutured tendon around fabella + muscle reinforcing sutures |
Not specified |
Not specified |
Not specified |
|
Reinke et al (1982)[3] |
9 yo Beagle mix (15 kg) |
Trauma/Lateral head and distal musculotendinous lesion |
Plantigrade |
Supracondylar hole, cerclage wire distal to fabella. Apposition sutures (nylon) for distal end of gastrocnemius |
Heavily padded bandage with hock hyperextended and flexed stifle (6 weeks) |
None |
9 weeks—walked and stood normally |
|
Muir and Dueland (1994)[4] |
2 yo Schipperke (6.9 kg) |
Trauma/Medial head |
Lameness of variable severity |
Conservative (hydrotherapy, analgesia, short leash walks for 6 weeks) |
None |
None |
3 months—occasional limp after exercise |
|
Prior (1994)[5] |
6 yo Border Collie |
Trauma/Lateral head |
Plantigrade |
Spiked washer and 3.5 mm cortical bone screw |
Support dressing with stifle in extension (10 days) |
None |
6 weeks—good use of the leg, no signs of lameness or pain |
|
Robinson (1999)[11] |
8.5 yo Golden Retriever (31.2 kg) |
Atraumatic/Lateral & medial |
Stiffness progressing to hyperflexion of the right hock |
RHL: Bilateral approach + supracondylar femoral holes + Figure-of-eight wire (1 mm wire) around fabella Revision: 1.25 mm wire LHL: Same procedure only lateral head |
Plantar support in extension (12 weeks total) |
Wire breakage—at 6 and 9 weeks postop Bandage related sores |
3 months—walking almost normally on both 3 years—normal gait. Mild distalization fabellae |
|
Ridge and Owen (2005)[6] |
5.5 yo Golden Retriever |
Trauma/Lateral head |
Plantigrade |
Lateral supracondylar tunnel + fabellar bone tunnel + 2–0 PDS Revision: 80lb leader line + 3 femoral condylar tunnels + Bunnell-Mayo tendon sutures with L-lactid/glycolid (Panacryl) |
MRJB in extension (10 days) Postrevision: Type 1a transarticular ESF in extension (6 weeks) + support dressing (2 weeks) |
Wire breakage and seroma—at 10 days postop |
8 weeks—no plantigrade 1 year—normal stance and gait |
|
Ting et al (2006)[7] |
6 yo Labrador |
Trauma/lateral head + pelvic fracture same side |
Plantigrade |
Cerclage wires and tissue anchors |
Immobilization in partial extension |
Not specified |
Not specified |
|
Mueller et al (2009)[8] |
9 yo Malinois (34 kg) |
Atraumatic-chronic/Lateral fabella avulsion fracture |
Intermittent RHL lameness |
Conservative (Carprofen 5 days, 13 sessions therapeutic US—5 weeks) |
None |
None |
5 weeks—no visible lameness |
|
Mueller et al (2009)[8] |
2 yo German Shepherd dog (30 kg) |
Atraumatic-acute/Medial head |
3rd degree lameness |
Conservative (Carprofen 5 days, 12 sessions therapeutic US—4 weeks) |
None |
None |
2 months—no lameness |
|
Bali (2011)[9] |
7 yo Domestic Short Hair (6.7 kg) |
Unknown/lateral head |
Plantigrade |
Supracondylar tunnels + 2 sutures (0 PDS) modified locking loop pattern |
Calcaneo-tibial screw (5 weeks) + MRJB with lateral splint (7 weeks) |
None |
Not specified |
|
Pratesi et al (2012)[10] |
3.5 yo Domestic Short Hair |
Suspected trauma/Lateral head |
Plantigrade |
Suture anchor + modified 3-loop pulley (0 PDS) distal to fabella |
Stifle flexion device |
None |
6 weeks—no lameness 5 months—normal |
|
Lideo and Milan (2013)[18] |
4 yo German Hound (34 kg) |
Unknown/Medial head |
RHL lameness |
Conservative (shortwave, twice a week for 1 month) |
None |
None |
1 month—no lameness or pain |
Abbreviations: ESF, external skeletal fixator; MRJB, modified Robert Jones bandage; NWB, non-weight bearing; PDS, Polydioxanone; RHL/LHL, right/left hindlimb; US, ultrasound; yo, year/s-old.
Most lesions are unilateral, acute and traumatic in nature; however, atraumatic bilateral avulsion of the origin of the gastrocnemius has been reported in one dog.[11]
Cases present with a history of weight-bearing lameness with different degrees of tarsal hyperflexion, eventually leading to a complete plantigrade stance. Integrity of the musculus flexor digitorum superficialis (mFDS) can be recognized by the characteristic abnormal contracture of the digits when the tarsus is hyperflexed.[12] [13]
The aim of this report is to review the literature and to describe in a dog, the avulsion of the lateral head of the gastrocnemius combined with a tear in the medial head treated surgically using a modified technique. In addition, we studied and report the possible biomechanical mechanism of this injury in a cadaveric model.
Case Report
A 6-year-old male neutered Border Collie presented with a 4-month right hindlimb lameness, following a jump. This progressed to a plantigrade stance during the following 2 months. Concurrently the dog had hip dysplasia, managed with meloxicam (Metacam, Boehringer-Ingelheim, Germany; 0.1 mg/kg). Tramadol hydrochloride (Tramadol, Almus, United Kingdom; 2 mg/kg) was also prescribed, with no improvement seen. A 2-week course of prednisolone (Prednidale, Dechra, United Kingdom; 0.5mg/kg), combined with restricted exercise and hydrotherapy, was attempted with no success prior to referral.
On examination, the dog was overweight; 27.5 kg, body condition score 8/9[14] and displayed a right hindlimb plantigrade lameness. There was moderate muscle atrophy of his limb with pain elicited upon deep palpation of the lateral head of the gastrocnemius. With the stifle partially flexed, the lateral fabella could be palpated distal from its usual location. The tarsus could be flexed while the stifle was held in extension, without flexion of the digits, indicative of an Achilles mechanism insufficiency and damage to the mFDS. Discomfort was elicited when performing this manoeuvre. A 1-cm diameter superficial contact ulcer was present on the plantar surface of the right tarsus. On neurological examination, placing reflexes appeared delayed, although this was suspected to be mechanical rather than neurological in origin. Segmental reflexes were intact.
Orthogonal radiographs of both stifles and tarsi were taken under a combination of medetomidine (Sedator, Dechra, United Kingdom; 0.01 mg/kg) and butorphanol (Torbugesic; Zoetis, United Kingdom; 0.1 mg/kg intravenously [IV]). Radiographs confirmed distalization and remodelling of the right lateral fabella ([Fig. 1A–C]).

Ultrasound of the gastrocnemius muscle was performed. This revealed a hypoechoic area distal to the lateral fabella, indicating avulsion of the lateral head of the gastrocnemius and the origin of the mFDS ([Fig. 2A and B]). Ultrasound of the medial belly of the gastrocnemius showed an ill-defined lesion with hyperechoic and hypoechoic areas, compatible with a mid-body muscular lesion ([Fig. 2C]).

Surgical Management
Methadone (Comfortan, Dechra, United Kingdom; 0.3 mg/kg) and acepromazine (ACP, Elanco, United Kingdom; 0.02 mg/kg) were administered intramuscular as premedication. Induction of anaesthesia with propofol (PropoFlo, Zoetis, United Kingdom; 2 mg/kg IV) and maintained with isoflurane (IsoFlo, Zoetis, United Kingdom). Amoxicillin–clavulanate (Augmentin, GlaxoSmithKline, United Kingdom; 20 mg/kg IV) was administered 30 minutes preoperatively and every 90 minutes intraoperatively.
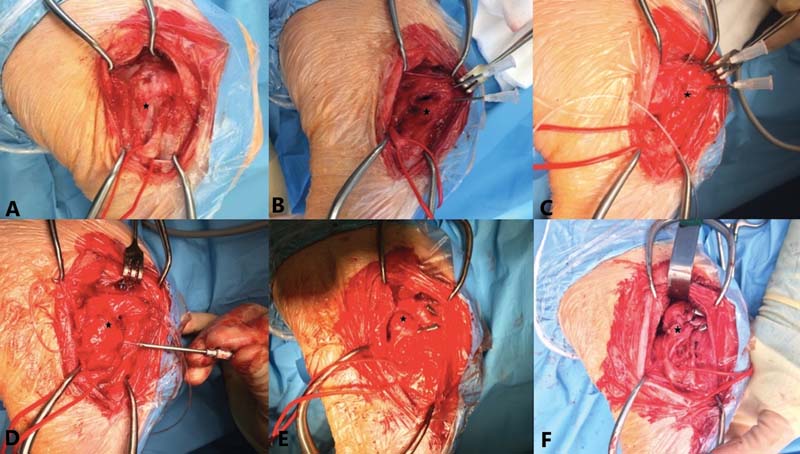
A caudolateral approach to the right stifle was performed. The avulsed lateral head of the gastrocnemius was visualized; it was fibrosed and contracted. The peroneal nerve was isolated and protected ([Fig. 3A]). Two 2 mm bone tunnels were pre-drilled in the lateral femoral condyle, craniolateral to caudomedial direction, exiting at the level of the origin of the gastrocnemius muscle ([Fig. 3B]). Two 16 G needles facilitated passage of the suture ([Fig. 3C]). While the tarsus was held in extension, the lateral head of the gastrocnemius and the fabella were pulled proximally and positioned as close as possible to its origin. Due to the amount of muscular contraction, the fabella could not be repositioned back to its anatomical position, remaining in a mildly distal location. Two 100lb Nylon (Leader Line, Veterinary Instrumentation, United Kingdom) mattress sutures were passed through the condylar bone tunnels and caudal and distal to the lateral fabella ([Fig. 3D]). These were crimped individually on the lateral aspect, with the stifle in a standing angle position ([Fig. 3E]). The disrupted gastrocnemius was then attached to the biceps femoris and associated soft tissues by placing four 0 Polydioxanone (PDS II, Ethicon, New Jersey, United States) mattress sutures ([Fig. 3F]). The Achilles test was performed at the end of the procedure, confirming satisfactory function of the tendon.
Postoperative radiographs confirmed residual distalization of the lateral fabella ([Fig. 1D and E]).
A half cast was placed dorsally using resin-epoxy material (VetCast Plus; 3M, Saint Paul, Minnesota, United States), extending from the digits to the proximal tibia with the tarsus extended.
The patient was discharged the following day with oral meloxicam (Metacam, Boehringer-Ingelheim, Germany; 0.1 mg/kg) every 24 hours, and oral Trazodone (Trazodone Hydrochloride, Strides Pharma, United Kingdom) at a dose of 4 mg/kg, every 12 hours, to assist with the post-surgical exercise restriction.[15] A regime of strict exercise control was advised for 6 weeks. A holding-assisting device (Help-em-up Harness, Orthopets, United Kingdom) was provided and a calorie restricted diet was initiated.
Bandage changes were performed under sedation on a weekly basis for the first 2 weeks. The calcaneal wound was healing satisfactorily, and further dressing changes were performed every 2 weeks until complete cast removal, 5 weeks post-surgery.
At 5 weeks, the dog walked with a mild lameness. Muscle atrophy and mild reduction of tarsal flexion were evident. Standing angles of both tarsi were normal and Achilles function was restored. No cast related complications were present. Short on-the-lead controlled walks were recommended for a further 4 weeks.
Upon examination during follow-up appointments at 9.5 and 12 weeks postoperatively, the animal was sound at a walk/trot and displayed a normal tarsal standing angle. Muscle atrophy had improved, and Achilles function remained normal. At the 6-month re-examination, there were no signs of lameness or discomfort on palpation of the surgical site. The medial and lateral heads of the gastrocnemius were symmetrical and comparable to the contralateral limb. Range of motion was within normal limits and Achilles tendon had normal function.
Liverpool Osteoarthritis in Dogs questionnaire (LOAD)[16] was completed 1 year and 6 months following the procedure and the dog was reported to have returned to normal exercise levels, with a total LOAD score of 3/52. No complications were reported, and no medication was required.
Cadaveric Experiment
To understand the mechanism of concurrent muscle injury, a cadaveric experiment was performed. A Border Collie was euthanatized for reasons unrelated to the study, frozen at -20°C and thawed overnight. The dog was placed in sternal recumbency with the stifle extended. The common tendon of the biceps femoris, semitendinosus and gracilis muscle was incised midline and separated, exposing both bellies of the gastrocnemius muscle ([Fig. 4A]). The femoral attachment of the lateral fabella was incised with a no.11 blade. Manual pressure was applied to the tarsus in a cyclic fashion forcing the joint into a hyperflexed position. Hyperflexion could only be achieved following tearing of the muscle fibres of the medial head of the gastrocnemius on its medial aspect, at the level of the proximal third of the muscle belly. As tarsal flexion was continued, the muscle fibres continued to separate in a longitudinal direction. As extreme hyperflexion was reached, further disruption of the muscle was observed ([Fig. 4B]). The medial fabella and proximal muscle attachment remained in situ at all times. The mFDS was seen to displace distally along with the lateral head of the gastrocnemius.

Discussion
Injury to the gastrocnemius muscle often results in postural changes that can be severe if left untreated. Conservative management has been successfully reported in cases where there is no plantigradism, either due to partial avulsion of the origin of the gastrocnemius or due to gastrocnemius musculo-tendinopathy[4] [8] [17] [18] however, complete avulsion injuries require surgical repair to restore function of the Achilles tendon.[6] [7] [9]
Different surgical techniques have been described for the reattachment of the lateral and medial heads of the gastrocnemius, including the use of orthopaedic wire passed through supracondylar holes in the femur and either around the fabella[1] [7] or through bone tunnels drilled in the fabella,[6] carbon fibre augmentation[2] and reattachment by placement of a 3.5 mm cortical screw and a washer.[3] [5] Breakage of the orthopaedic wire was the main reason for failure of the repair, requiring revision surgery in two cases[6] [11] and long recovery times were frequently seen[1] [2] ([Table 1]).
The use of polydioxanone or polyamide suture material for the reattachment of the origin of the gastrocnemius has been reported in one dog during revision surgery[6] and in two cats.[9] [10] In our case, two 100 lb monofilament leader lines were chosen due to the size of the patient and the superior resistance to cyclic loading of the leader line when compared with orthopaedic wires.[6] In our case, the suture was encircling around the fabella instead of being passed through a bone tunnel created in the fabella. This provided excellent tissue purchase, eliminating the need to drill through the fabella, reducing the risk of fabella fracture and stress concentration effect[6]
Condylar instead of supracondylar bone tunnels were drilled in the femur, which has not been reported before. This was due to the severe distalization of the fabella and muscle contraction, impairing intraoperative approximation of the lateral fabella to its original anatomical position. This residual malposition did not appear to have any clinical significance, in agreement with previous reports.[4] [11] Based on these findings, if excessive tension is found intraoperatively, such as in chronic cases, it may be prudent to use condylar instead of supracondylar tunnels. This reduces the risk of suture breakage and muscle tear, without compromising the outcome, as shown in our case.
Following Achilles tendon repair, reported postoperative complications have also been attributable to the immobilization method.[19] These methods included application of a transarticular external fixator,[20] placement of a calcaneotibial bone screw,[9] [19] [21] [22] [23] a stifle flexion device[10] and different configurations of splints and casts. No clear superiority of one specific method has been proven and immobilization periods vary among authors.[19] Brinker and colleagues[24] suggested placement of a cast or lateral splint for 8 to 10 weeks followed by a Robert Jones bandage for 7 to 10 days, with a total of 8 to 10 weeks of severely restricted exercise.
In our case, a calcaneotibial screw was not placed due to the presence of a pressure ulcer near the point of insertion of a screw, which, if placed, would increase the risks of infection and wound complications. Despite the dog being overweight and very active, 5 weeks of immobilization with a cranial cast with the tarsus in extension, followed by gradual increases in exercise over 10 weeks, resulted in complete muscle healing, normal posture and gait. No complications associated with the duration or type of coaptation were seen and the pre-existing ulcer healed uneventfully.
The gastrocnemius muscle is the most powerful tarsal extensor during stance and locomotion.[13] The lateral head of this muscle is firmly united to the superficial digital flexor muscle proximally, sharing attachment to the lateral fabella.[3] [13] By repairing the lateral head of the gastrocnemius with an encircling leader line around the fabella, including enough healthy tissue to provide good suture purchase, the mFDS is also returned to its anatomical location, restoring function of both muscles, as shown in this case. Lesions distal to the fabella ([Fig. 2A]) may be repaired using mattress PDS sutures. It is unknown if these muscular tears occurred at the time of injury or subsequently.
A review of the literature shows that all cases that sustained isolated avulsion injury to the lateral head of the gastrocnemius progressed into complete plantigrade stance.[2] [3] [5] [6] [7] [10] [11] Only one of the published cases had an additional lesion at the distal musculotendinous unit of the gastrocnemius muscle.[3] In all cases, including in the latter, repair to the lateral head of the gastrocnemius alone resulted in restoration of the Achilles function. In addition to this, the literature suggests that isolated injury to the medial head of the gastrocnemius does not cause complete plantigradism.[4] [18]
Different hypotheses have been raised to explain the various degrees of plantigradism, in cases where only the lateral head of the gastrocnemius has been grossly affected. Reinke and colleagues[3] suggested that tarsal hyperflexion only occurs whenever the three components of the Achilles tendon are severed, based on an undetailed cadaveric study cited in the same report. It was speculated that, in cases where a lesion had occurred at the origin of the muscle, to develop a full plantigrade stance, injury to the medial head of the gastrocnemius must have occurred simultaneously but been undiagnosed and healed spontaneously. This was confirmed by ultrasound assessment in our case report and equally observed in the cadaveric experiment we performed.
Based on our findings, we believe that initially the lateral head of the gastrocnemius combined with the associated mFDS, avulses with the fabella. Damage to the medial head of the gastrocnemius occurs subsequently as the forces continue to act on the Achilles musculotendinous unit, resulting in a complete plantigrade stance.
We conclude that in this one case, repair of the lateral head of the gastrocnemius was sufficient to restore Achilles mechanism function, even if the muscular unit of the medial head of the gastrocnemius has been damaged. This may be taken into consideration when treating similar injuries.
To the author's knowledge, this is the first report in a dog of a lateral head of the gastrocnemius muscle avulsion repaired using two 100 lb Nylon (Leader Line, Veterinary Instrumentation, United Kingdom) mattress sutures through two condylar bone tunnels and around the lateral fabella, without surgical repair of the medial gastrocnemius, with no complications and an excellent long-term outcome. We also tried to describe on a cadaver model, the biomechanical mechanism whereby an isolated avulsion of the lateral head of the gastrocnemius may progress into a complete plantigrade stand due to subsequent medial gastrocnemius muscular tear.
Conflict of Interest
The authors declare no conflict of interest related to this report.
Acknowledgments
We would like to thank Alison King for her assistance with acquiring the ultrasound images and Vets Now Referrals Glasgow Ltd for providing the experimental materials and equipment used in this study.
Authors' Contributions
D.A. performed the surgery described. L.R. drafted the manuscript and D.A. approved the final version prior to submission.
-
References
- 1 Chaffee VW, Knecht CD. Avulsion of the medical head of the gastrocnemius in the dog. Vet Med Small Anim Clin 1975; 70 (08) 929-931
- 2 Vaughan LC. Muscle and tendon injuries in dogs. J Small Anim Pract 1979; 20 (12) 711-736
- 3 Reinke JD, Kus SP, Ownes JM. Traumatic avulsion of the lateral head of the gastrocnemius and superficial digital flexor muscles in a dog. J Am Anim Hosp Assoc 1982; 18: 252-258
- 4 Muir P, Dueland RT. Avulsion of the origin of the medial head of the gastrocnemius muscle in a dog. Vet Rec 1994; 135 (15) 359-360
- 5 Prior JE. Avulsion of the lateral head of the gastrocnemius muscle in a working dog. Vet Rec 1994; 134 (15) 382-383
- 6 Ridge PA, Owen MR. Unusual presentation of avulsion of the lateral head of the gastrocnemius muscle in a dog. J Small Anim Pract 2005; 46 (04) 196-198
- 7 Ting D, Petersen SW, Mazzaferro EM, Worth LT, Petersen SW. American College of Veterinary Radiology. What is your diagnosis? Avulsion of the origin of the gastrocnemius muscle. J Am Vet Med Assoc 2006; 228 (10) 1497-1498
- 8 Mueller MC, Gradner G, Hittmair KM, Dupre G, Bockstahler BA. Conservative treatment of partial gastrocnemius muscle avulsions in dogs using therapeutic ultrasound – a force plate study. Vet Comp Orthop Traumatol 2009; 22 (03) 243-248
- 9 Bali MS. Avulsion of the lateral head of the gastrocnemius muscle in a cat. J Feline Med Surg 2011; 13 (10) 784-786
- 10 Pratesi A, Grierson J, Moores AP. The use of a stifle flexion device to manage avulsion of the lateral head of the gastrocnemius muscle in a cat. Vet Comp Orthop Traumatol 2012; 25 (03) 246-249
- 11 Robinson A. Atraumatic bilateral avulsion of the origins of the gastrocnemius muscle. J Small Anim Pract 1999; 40 (10) 498-500
- 12 Meutstege FJ. The classification of Canine Achilles' tendon lesions. Vet Comp Orthop Traumatol 1993; 6: 53-55
- 13 Evans HE, de Lahunta A. Miller's Anatomy of the Dog. 4th edition. St Louis: Elsevier; 2013. :273
- 14 Laflamme DP. Development and validation of a body condition score system for dogs. Canine Pract 1997; 22: 10-15
- 15 Gruen ME, Roe SC, Griffith EH, Sherman BL. The use of trazodone to facilitate calm behavior after elective orthopedic surgery in dogs: results and lessons learned from a clinical trial. J Vet Behav 2017; 22: 41-45
- 16 Walton MB, Cowderoy E, Lascelles D, Innes JF. Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PLoS One 2013; 8 (03) e58125
- 17 Kaiser SM, Harms O, Konar M. et al. Clinical, radiographic, and magnetic resonance imaging findings of gastrocnemius musculotendinopathy in various dog breeds. Vet Comp Orthop Traumatol 2016; 29 (06) 515-521
- 18 Lideo L, Milan R. Ultrasound monitoring of shortwave diathermic treatment of gastrocnemius strain in a dog. J Ultrasound 2013; 16 (04) 231-234
- 19 Nielsen C, Pluhar GE. Outcome following surgical repair of Achilles tendon rupture and comparison between postoperative tibiotarsal immobilization methods in dogs: 28 cases (1997–2004). Vet Comp Orthop Traumatol 2006; 19 (04) 246-249
- 20 De Haan JJ, Goring RL, Renberg C, Bertrand S. Modified transarticular external skeletal fixation for support of achilles tenorrhaphy in four dogs. Vet Comp Orthop Traumatol 1995; 8: 32-35
- 21 Guerin S, Burbidge H, Firth E, Fox S. Achilles tenorrhaphy in five dogs: a modified surgical technique and evaluation of a cranial half cast. Vet Comp Orthop Traumatol 1998; 11: 205-210
- 22 Sivacolundhu RK, Marchevsky AM, Read RA, Eger C. Achilles mechanism reconstruction in four dogs. Vet Comp Orthop Traumatol 2001; 14: 25-31
- 23 Corr SA, Draffan D, Kulendra E, Carmichael S, Brodbelt D. Retrospective study of Achilles mechanism disruption in 45 dogs. Vet Rec 2010; 167 (11) 407-411
- 24 Brinker WO, Piermattei DL, Flo GL. Handbook of Small Animal Orthopedics and Fracture Treatment. 2nd edition. Philadelphia: WB Saunders; 1992. :722–724
Address for correspondence
Publication History
Received: 02 August 2021
Accepted: 22 November 2021
Article published online:
12 July 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Chaffee VW, Knecht CD. Avulsion of the medical head of the gastrocnemius in the dog. Vet Med Small Anim Clin 1975; 70 (08) 929-931
- 2 Vaughan LC. Muscle and tendon injuries in dogs. J Small Anim Pract 1979; 20 (12) 711-736
- 3 Reinke JD, Kus SP, Ownes JM. Traumatic avulsion of the lateral head of the gastrocnemius and superficial digital flexor muscles in a dog. J Am Anim Hosp Assoc 1982; 18: 252-258
- 4 Muir P, Dueland RT. Avulsion of the origin of the medial head of the gastrocnemius muscle in a dog. Vet Rec 1994; 135 (15) 359-360
- 5 Prior JE. Avulsion of the lateral head of the gastrocnemius muscle in a working dog. Vet Rec 1994; 134 (15) 382-383
- 6 Ridge PA, Owen MR. Unusual presentation of avulsion of the lateral head of the gastrocnemius muscle in a dog. J Small Anim Pract 2005; 46 (04) 196-198
- 7 Ting D, Petersen SW, Mazzaferro EM, Worth LT, Petersen SW. American College of Veterinary Radiology. What is your diagnosis? Avulsion of the origin of the gastrocnemius muscle. J Am Vet Med Assoc 2006; 228 (10) 1497-1498
- 8 Mueller MC, Gradner G, Hittmair KM, Dupre G, Bockstahler BA. Conservative treatment of partial gastrocnemius muscle avulsions in dogs using therapeutic ultrasound – a force plate study. Vet Comp Orthop Traumatol 2009; 22 (03) 243-248
- 9 Bali MS. Avulsion of the lateral head of the gastrocnemius muscle in a cat. J Feline Med Surg 2011; 13 (10) 784-786
- 10 Pratesi A, Grierson J, Moores AP. The use of a stifle flexion device to manage avulsion of the lateral head of the gastrocnemius muscle in a cat. Vet Comp Orthop Traumatol 2012; 25 (03) 246-249
- 11 Robinson A. Atraumatic bilateral avulsion of the origins of the gastrocnemius muscle. J Small Anim Pract 1999; 40 (10) 498-500
- 12 Meutstege FJ. The classification of Canine Achilles' tendon lesions. Vet Comp Orthop Traumatol 1993; 6: 53-55
- 13 Evans HE, de Lahunta A. Miller's Anatomy of the Dog. 4th edition. St Louis: Elsevier; 2013. :273
- 14 Laflamme DP. Development and validation of a body condition score system for dogs. Canine Pract 1997; 22: 10-15
- 15 Gruen ME, Roe SC, Griffith EH, Sherman BL. The use of trazodone to facilitate calm behavior after elective orthopedic surgery in dogs: results and lessons learned from a clinical trial. J Vet Behav 2017; 22: 41-45
- 16 Walton MB, Cowderoy E, Lascelles D, Innes JF. Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PLoS One 2013; 8 (03) e58125
- 17 Kaiser SM, Harms O, Konar M. et al. Clinical, radiographic, and magnetic resonance imaging findings of gastrocnemius musculotendinopathy in various dog breeds. Vet Comp Orthop Traumatol 2016; 29 (06) 515-521
- 18 Lideo L, Milan R. Ultrasound monitoring of shortwave diathermic treatment of gastrocnemius strain in a dog. J Ultrasound 2013; 16 (04) 231-234
- 19 Nielsen C, Pluhar GE. Outcome following surgical repair of Achilles tendon rupture and comparison between postoperative tibiotarsal immobilization methods in dogs: 28 cases (1997–2004). Vet Comp Orthop Traumatol 2006; 19 (04) 246-249
- 20 De Haan JJ, Goring RL, Renberg C, Bertrand S. Modified transarticular external skeletal fixation for support of achilles tenorrhaphy in four dogs. Vet Comp Orthop Traumatol 1995; 8: 32-35
- 21 Guerin S, Burbidge H, Firth E, Fox S. Achilles tenorrhaphy in five dogs: a modified surgical technique and evaluation of a cranial half cast. Vet Comp Orthop Traumatol 1998; 11: 205-210
- 22 Sivacolundhu RK, Marchevsky AM, Read RA, Eger C. Achilles mechanism reconstruction in four dogs. Vet Comp Orthop Traumatol 2001; 14: 25-31
- 23 Corr SA, Draffan D, Kulendra E, Carmichael S, Brodbelt D. Retrospective study of Achilles mechanism disruption in 45 dogs. Vet Rec 2010; 167 (11) 407-411
- 24 Brinker WO, Piermattei DL, Flo GL. Handbook of Small Animal Orthopedics and Fracture Treatment. 2nd edition. Philadelphia: WB Saunders; 1992. :722–724