

Subscribe to RSS
DOI: 10.1055/s-0042-1750357
Preoperative Assessment and Prediction of Consistency of Intracranial Meningioma Utilizing the Apparent Diffusion Coefficient Values
Authors
Funding None.


Abstract
Objectives Consistency of meningioma is important for preoperative planning, surgical resection, and predicting surgical outcomes. We prospectively evaluated the utility of the apparent diffusion coefficient (ADC) values to assess the consistency of meningioma.
Methods Preoperative magnetic resonance imaging (MRI) was performed on 23 patients with meningioma before undergoing surgical resection and the average/mean of ADC minimum (ADCmin), maximum (ADCmax), and mean (ADCmean) values were calculated. Intraoperatively, the meningiomas were characterized as firm or soft and correlated with ADC values.
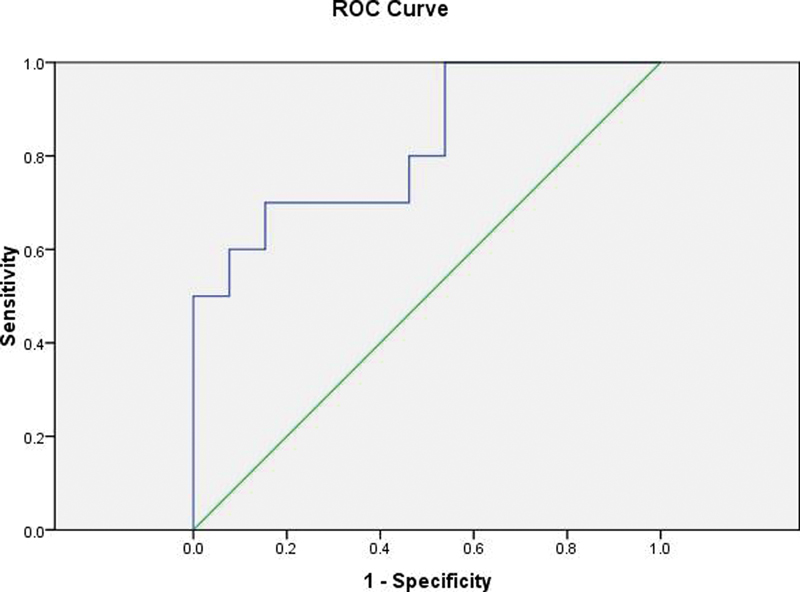
Results ADCmin, ADCmax, and ADCmean values of soft and firm meningiomas were significantly different with a p-value of < 0.05. ADCmin value of < 691.3 × 10−6 mm2/s had 80% sensitivity and 84.6% specificity for identifying firm from the soft tumors with the area under the curve (AUC) = 0.862, p-value of 0.004, positive predictive value (PPV) 80, and negative predictive value (NPV) 84.6. ADCmax value of < 933.6 × 10−6 mm2/s had 70% sensitivity and 84.6% specificity for identifying firm from the soft tumors with AUC = 0.823, p-value of 0.009, PPV 77.8, and NPV 78.6. ADCmean value of < 840.8 × 10−6 mm2/s had 90% sensitivity and 76.9% specificity for identifying firm from the soft tumors with AUC = 0.900, p-value of 0.001, PPV 75, and NPV 90.9.
Conclusion Diffusion-weighted MRI using ADC minimum, ADC maximum, and ADC mean values can be used to differentiate firm from soft meningiomas. Meningiomas with hard consistency showed relatively low ADC values.
Introduction
Meningiomas are dural-based tumors that arise from arachnoid cells surrounding the brain.[1] About 90% of meningiomas are supratentorial and seen in the parasagittal region, convexities, sphenoid ridge, and olfactory groove in descending order of frequency. Infratentorial meningiomas are commonly located in petrous and clival regions.[2] These may become symptomatic or detected asymptomatically. Meningiomas are usually isointense on both T1-weighted (T1W) and T2-weighted (T2W) images to the cerebral cortex on magnetic resonance imaging (MRI) with avid enhancement on postcontrast images. Dural tail and vasogenic edema are also commonly seen.[3] Surgery is the main modality to treat symptomatic patients with meningioma. The intraoperative consistency of meningioma is vital in formulating the plan of surgical approach and predicting the surgical outcome. Soft consistency tumors can be treated by suctioning whereas those with hard consistency require meticulous prolonged dissection with the added risk of damage to vital structures in the proximity to the tumor. The surgeon needs to have a noninvasive method that can preoperatively evaluate the consistency of meningioma for optimal risk assessment and patient management. Soft tumors can thus be directly approached and treated with suctioning whereas other options such as preoperative transarterial embolization to soften tumors and aid resection can be given in the case of hard meningiomas.[4]
Few studies have employed standard T1W and T2W imaging for preoperative assessment of the consistency of meningioma; however, it remains imprecise because in addition to water content other factors also come into play in defining the consistency of tumor.[5] [6] [7] [8] A previous study by Yogi et al[9] has retrospectively demonstrated a significant correlation between the apparent diffusion coefficient (ADC)min values and intraoperative tumor consistency. The primary intention of our study was to evaluate the utility of ADC values in preoperative prediction of consistency of meningioma and comparing with intraoperative assessment by the neurosurgeon.
Materials and Methods
This was a single-institution prospective study that was approved by the Institute Ethics Committee of our institute. A total of 23 consecutive meningioma patients who were operated on during the study period of January 2015 to May 2016 were enrolled in the study. The risks and possible benefits of the procedure were fully explained to the patients and written informed consent was taken from the patient before enrollment in the study as per the attached pro forma. Inclusion criteria were surgical candidates of meningioma referred for preoperative MRI. Exclusion criteria were the presence of MRI acquisition contraindications, that is, metallic implants, claustrophobia, refusal to give consent, meningioma which was showing more than 50% areas of necrosis or calcification, and recurrent/residual meningioma.
All MR examinations were performed on a 1.5 T MR scanner—Magnetom Aera system (Siemens Healthcare, Erlangen, Germany)—using a quadrature head coil. All patients underwent MRI including T1W imaging sequence (repetition time [TR]/echo time [TE]) [ms] = 1890/4.17; section thickness, 1 mm); and axial turbo spin-echo T2W imaging sequence ([TR/TE] [ms] = 4290/109; section thickness, 4 mm). Susceptibility-weighted imaging (SWI) sequence was acquired in the axial plane (TR/TE) (ms) = 49/40; section thickness, 2.2 mm. Diffusion-weighted imaging (DWI) was acquired in the axial plane using single-shot spin-echo echo-planar (EP) sequences (field of view, 230 mm; section thickness, 4 mm; intersection gap, 2.5 mm; acquisition time, 70 s; and b values, 0 and 1,000 s/mm2) with subsequent generation of ADC maps.
The MRI-DWI data set was transferred to a workstation and systematically evaluated by a neuroradiologist with over 3 years of experience. The observer who was blinded to the patient's details created the manual regions-of-interests (ROIs) along the tumor border on T2WI. This ROI was then brought on to ADC map. The observer ensured to avoid areas with necrosis and calcification within the ROI. Areas of cystic degeneration and susceptibility artifacts derived from nearby air and bone structures were avoided. The ADC minimum, ADC maximum, and ADC mean values were generated from ROI. ROIs were drawn on all slices where the lesion was visualized. Mean of ADC minimum (ADCmin), mean of ADC maximum (ADCmax), and mean of ADC mean (ADCmean) were calculated. Necrosis was defined as the presence of T2 heterogeneous hyperintensity in the tumor which does not show contrast enhancement. Calcification was defined as the presence of a T2 hypointense area that shows blooming on SWI.
Operative technique: For all patients, surgical resection was done by a neurosurgeon who was blinded to the consistency based on imaging parameters and classified them into two groups: “soft” consistency (removed predominantly by suction) and “firm” consistency (predominantly excised) according to Sitthinamsuwan et al criteria.[10]
Statistical analyses: The statistical analysis was done by SPSS software version 20 (Statistical Packages for the Social Sciences, Chicago, Illinois, United States). The Kolmogorov–Smirnov test was done to determine the normality of data distribution. Quantitative variables like age and ADC values were calculated and presented as mean ± standard deviation (SD). For categorical data (soft/hard, malignant/benign, male/female, presence or absence of symptom) number and the percentage were calculated. Cronbach's α reliability test was used to measure the intraobserver variability of ADC values by ROI. The comparison between consistency of meningioma and ADC values (minimum, maximum, and mean) were done by using a Student's t-test because ADC values are normally distributed. A receiver operating characteristic (ROC) curve was used to calculate cutoff points of ADC value to differentiate soft from hard tumors with calculations of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of this diagnostic tool. A p-value of < 0.05 was considered to indicate statistical significance.
Results
The study population consisted of 18 (78.3%) females and 5 (21.7%) males with a mean age of 47.17 years (SD: 10.391, range o29–68 years). The anatomical distribution of meningiomas includes three along the sphenoid ridge, one in the cerebellopontine angle, eight along the cerebral convexity, five in the parasagittal location, two in the tuberculum sellae, two along the tentorium, one along the cribriform plate, and one in the petroclival region. ADCmin, ADCmax, and ADCmean value of soft and firm meningiomas were significantly different. ADCmin value of < 691.3 × 10−6 mm2/s had 80% sensitivity and 84.6% specificity for identifying firm from the soft tumors with area under the curve (AUC) = 0.862, p-value of 0.004, PPV 80, and NPV 84.6 ([Figs. 1] and [2]). ADCmax value of < 933.6 × 10−6 mm2/s had 70% sensitivity and 84.6% specificity for identifying firm from the soft tumors with AUC = 0.823, p-value of 0.009, PPV 77.8, and NPV 78.6 ([Figs. 3] and [4]). ADCmean value of < 840.80 × 10−6 mm2/s had 90% sensitivity and 76.9% specificity for identifying firm from the soft tumors with AUC = 0.900, p-value of 0.001, PPV 75, and NPV 90.9 ([Figs. 5] and [6]). Cronbach's α reliability test showed excellent consistency of ADC values by ROI (ADCmin 0.975, ADCmax 0.985, and ADCmean 0.987). At surgery, 10 meningiomas were classified as hard and 13 as soft. On histopathology, the soft group ([Fig. 7]) consisted of six meningothelial, five transitional, one angiomatous, and one chordoid subtypes. The hard group ([Fig. 8]) consisted of seven meningothelial, two fibroblastic, two angiomatous, and one secretory meningioma subtypes. Out of 23 meningiomas, 21 were benign (World Health Organization [WHO] grade I) and 2 were atypical (WHO grade II). No correlation was found between the ADC values and WHO grading of meningioma.







Discussion
The intraoperative consistency of meningioma is vital for planning the surgical strategy, predicting the degree of removal, and adjunctive therapy. Differentiation of soft from firm tumors will be useful in early surgical planning. Previously, few studies have shown the correlation between MR signal and meningioma consistency. Sitthinamsuwan et al[10] showed that the signal intensity of meningiomas on T2WI and fluid-attenuated inversion recovery images were independent factors and significantly correlate with its consistency. Hoover et al[11] retrospectively included 101 patents with intracranial meningioma to characterize based on T1/T2 signal intensities. They concluded that T1WI and T2WI series can predict meningioma consistency with overall sensitivities for detecting soft and firm consistency as 90 and 56%, respectively. Maiuri et al[7] found in their study that meningiomas showing increased hyperintensity than the cortex on T2WI were usually soft whereas those with hypointensity were frequently hard. But few other studies did not demonstrate such an association between MRI signal intensity and consistency.[12] [13] The consistency of meningioma as in any tumor is based on cellularity and amount of fibrous tissue. In cases of meningioma, there is the presence of interdigitations that are connected with extracellular cisterns and junctional complexes. Increased cellularity and fibrous contents can result in low T2W signal, while the presence of widened extracellular space with increased interstitial fluid can cause high T2W signal intensity. Thus, there is a complex interplay between these factors which may limit the utility of conventional sequences to predict the consistency of meningioma. Studies done previously also suggested that the ADC value inversely correlates with fibrous tissue content and cellularity.[8] [14] [15] Thus, it is assumed that the tumors with low ADC value may have a hard consistency. At present, there are only a few studies that established the ability of DWI in the preoperative characterization of intracranial meningiomas. We tried to compare the ADCmin, ADCmax, and ADCmean values of meningiomas among soft and firm groups. In our study, when using ADCmin value of < 691.33 × 10−6 mm2/s for identification of hard tumors, it shows 80% sensitivity and 84.6% specificity with AUC = 0.862, p-value of 0.004, PPV 80, and NPV 84.6. When using ADCmax value of < 933.67 × 10−6 mm2/s for identification of the hard tumors, it shows 70% sensitivity and 84.6% specificity with AUC = 0.823, p-value of 0.009, PPV 77.8, and NPV 78.6. When using ADCmean value of < 840.8 × 10−6 mm2/s giving 90% sensitivity and 76.9% specificity for identifying firm from the soft tumors with AUC = 0.900, p-value of 0.001, PPV 75, and NPV 90.9. Hoover et al found no correlation in their study with ADC and tumor consistency; however, they did not calculate ADC values and only qualitative analysis was performed.[11] Watanabe et al found no correlation between the ADC value and meningioma consistency. They believed that the ADC value is affected not only by the extracellular volume fraction but also by tumor cellularity.[16]
A study performed in meningiomas by Yogi et al[9] showed that hard meningiomas compared with soft meningiomas has significantly lower ADCmin value (p0.001). But, ADCmax and ADCmean values showed no significant difference between the two groups, though these values of the hard group are likely to be lower (p = 0.52 and 0.21, respectively). According to the ADCmin value, the ROC curve had shown 0.64 × 10–3 mm2/s as the best cutoff value in their study. According to this cutoff value, sensitivity and specificity were 88 and 81%, respectively, and the AUC was 0.9. These values are similar to the values of our study except for mild differences. Besides, ADCmax and ADCmean values also showed a significant difference between firm and soft groups in our study. This may be due to the inherent difference in the study composition of the meningiomas encountered in the two studies and the differences in the study protocol and anatomical location. We intentionally avoided areas of cystic degeneration and susceptibility artifacts. Similar to previous studies our study also evaluated the correlation between ADC values and histopathological subtypes but found no significant association.[17] [18] [19]
Multiple studies have demonstrated the association between ADC values and meningioma grades with atypical and malignant meningiomas showing lower ADC values as compared with benign meningiomas.[20] [21] We could not find any correlation between ADC values and WHO grading of meningioma, likely due to predominant study population (21 out of 23) had benign/WHO grade I meningiomas. There were few limitations in our study. The sample size in our study was relatively small. Further studies with a larger sample size are needed to know the exact diagnostic accuracy of DWI. No histopathological correlation was found with ADC values with this small sample size. DWI was on echo planar sequences which are highly susceptible to artifacts especially at the skull base and along the air sinuses.
Conclusion
Diffusion-weighted MRI using ADC minimum, ADC maximum, and ADC mean values can be used to differentiate firm from soft meningioma. Meningiomas with low ADC values are considered to have a hard consistency. DWI is a basic sequence available in most MRI scanners and the findings are easily reproducible. We promise that this quick and easily applied system using ADC can be used to predict the intraoperative consistency of cranial meningioma on preoperative MRI. It is vital to know the consistency of meningioma for proper surgical planning and utilization of devices to minimize the complication and improve surgical outcomes.
Conflict of Interest
None declared.
-
References
- 1 Drevelegas A. Extra-axial brain tumors. Eur Radiol 2005; 15 (03) 453-467
- 2 Weber DC, Lovblad KO, Rogers L. New pathology classification, imagery techniques and prospective trials for meningiomas: the future looks bright. Curr Opin Neurol 2010; 23 (06) 563-570
- 3 Simis A, Pires de Aguiar PH, Leite CC, Santana Jr PA, Rosemberg S, Teixeira MJ. Peritumoral brain edema in benign meningiomas: correlation with clinical, radiologic, and surgical factors and possible role on recurrence. Surg Neurol 2008; 70 (05) 471-477 , discussion 477
- 4 Campbell BA, Jhamb A, Maguire JA, Toyota B, Ma R, Roy M. Meningiomas in 2009: controversies and future challenges. Am J Clin Oncol 2009; 32 (01) 73-85
- 5 Eis M, Els T, Hoehn-Berlage M, Hossmann KA. Quantitative diffusion MR imaging of cerebral tumor and edema. Acta Neurochir Suppl (Wien) 1994; 60: 344-346
- 6 Chen TC, Zee CS, Miller CA. et al. Magnetic resonance imaging and pathological correlates of meningiomas. Neurosurgery 1992; 31 (06) 1015-1021 , discussion 1021–1022
- 7 Maiuri F, Iaconetta G, de Divitiis O, Cirillo S, Di Salle F, De Caro ML. Intracranial meningiomas: correlations between MR imaging and histology. Eur J Radiol 1999; 31 (01) 69-75
- 8 Guo AC, Cummings TJ, Dash RC, Provenzale JM. Lymphomas and high-grade astrocytomas: comparison of water diffusibility and histologic characteristics. Radiology 2002; 224 (01) 177-183
- 9 Yogi A, Koga T, Azama K. et al. Usefulness of the apparent diffusion coefficient (ADC) for predicting the consistency of intracranial meningiomas. Clin Imaging 2014; 38 (06) 802-807
- 10 Sitthinamsuwan B, Khampalikit I, Nunta-aree S, Srirabheebhat P, Witthiwej T, Nitising A. Predictors of meningioma consistency: a study in 243 consecutive cases. Acta Neurochir (Wien) 2012; 154 (08) 1383-1389
- 11 Hoover JM, Morris JM, Meyer FB. Use of preoperative magnetic resonance imaging T1 and T2 sequences to determine intraoperative meningioma consistency. Surg Neurol Int 2011; 2: 142
- 12 Carpeggiani P, Crisi G, Trevisan C. MRI of intracranial meningiomas: correlations with histology and physical consistency. Neuroradiology 1993; 35 (07) 532-536
- 13 Kasoff SS, Spiller M, Valsamis MP. et al. Relaxometry of noncalcified human meningiomas. Correlation with histology and solids content. Invest Radiol 1995; 30 (01) 49-55
- 14 Kono K, Inoue Y, Nakayama K. et al. The role of diffusion-weighted imaging in patients with brain tumors. AJNR Am J Neuroradiol 2001; 22 (06) 1081-1088
- 15 Sugahara T, Korogi Y, Kochi M. et al. Usefulness of diffusion-weighted MRI with echo-planar technique in the evaluation of cellularity in gliomas. J Magn Reson Imaging 1999; 9 (01) 53-60
- 16 Watanabe Y, Yamasaki F, Kajiwara Y. et al. Preoperative histological grading of meningiomas using apparent diffusion coefficient at 3T MRI. Eur J Radiol 2013; 82 (04) 658-663
- 17 Yamasaki F, Kurisu K, Satoh K. et al. Apparent diffusion coefficient of human brain tumors at MR imaging. Radiology 2005; 235 (03) 985-991
- 18 Hakyemez B, Yildirim N, Gokalp G, Erdogan C, Parlak M. The contribution of diffusion-weighted MR imaging to distinguishing typical from atypical meningiomas. Neuroradiology 2006; 48 (08) 513-520
- 19 Santelli L, Ramondo G, Della Puppa A. et al. Diffusion-weighted imaging does not predict histological grading in meningiomas. Acta Neurochir (Wien) 2010; 152 (08) 1315-1319 , discussion 1319
- 20 Bano S, Waraich MM, Khan MA, Buzdar SA, Manzur S. Diagnostic value of apparent diffusion coefficient for the accurate assessment and differentiation of intracranial meningiomas. Acta Radiol Short Rep 2013; 2 (07) 2047981613512484
- 21 Surov A, Gottschling S, Mawrin C. et al. Diffusion weighted imaging in meningioma: prediction of tumor grade and association with histopathological parameters. Transl Oncol 2015; 8 (06) 517-523
Address for correspondence
Publication History
Article published online:
27 September 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Drevelegas A. Extra-axial brain tumors. Eur Radiol 2005; 15 (03) 453-467
- 2 Weber DC, Lovblad KO, Rogers L. New pathology classification, imagery techniques and prospective trials for meningiomas: the future looks bright. Curr Opin Neurol 2010; 23 (06) 563-570
- 3 Simis A, Pires de Aguiar PH, Leite CC, Santana Jr PA, Rosemberg S, Teixeira MJ. Peritumoral brain edema in benign meningiomas: correlation with clinical, radiologic, and surgical factors and possible role on recurrence. Surg Neurol 2008; 70 (05) 471-477 , discussion 477
- 4 Campbell BA, Jhamb A, Maguire JA, Toyota B, Ma R, Roy M. Meningiomas in 2009: controversies and future challenges. Am J Clin Oncol 2009; 32 (01) 73-85
- 5 Eis M, Els T, Hoehn-Berlage M, Hossmann KA. Quantitative diffusion MR imaging of cerebral tumor and edema. Acta Neurochir Suppl (Wien) 1994; 60: 344-346
- 6 Chen TC, Zee CS, Miller CA. et al. Magnetic resonance imaging and pathological correlates of meningiomas. Neurosurgery 1992; 31 (06) 1015-1021 , discussion 1021–1022
- 7 Maiuri F, Iaconetta G, de Divitiis O, Cirillo S, Di Salle F, De Caro ML. Intracranial meningiomas: correlations between MR imaging and histology. Eur J Radiol 1999; 31 (01) 69-75
- 8 Guo AC, Cummings TJ, Dash RC, Provenzale JM. Lymphomas and high-grade astrocytomas: comparison of water diffusibility and histologic characteristics. Radiology 2002; 224 (01) 177-183
- 9 Yogi A, Koga T, Azama K. et al. Usefulness of the apparent diffusion coefficient (ADC) for predicting the consistency of intracranial meningiomas. Clin Imaging 2014; 38 (06) 802-807
- 10 Sitthinamsuwan B, Khampalikit I, Nunta-aree S, Srirabheebhat P, Witthiwej T, Nitising A. Predictors of meningioma consistency: a study in 243 consecutive cases. Acta Neurochir (Wien) 2012; 154 (08) 1383-1389
- 11 Hoover JM, Morris JM, Meyer FB. Use of preoperative magnetic resonance imaging T1 and T2 sequences to determine intraoperative meningioma consistency. Surg Neurol Int 2011; 2: 142
- 12 Carpeggiani P, Crisi G, Trevisan C. MRI of intracranial meningiomas: correlations with histology and physical consistency. Neuroradiology 1993; 35 (07) 532-536
- 13 Kasoff SS, Spiller M, Valsamis MP. et al. Relaxometry of noncalcified human meningiomas. Correlation with histology and solids content. Invest Radiol 1995; 30 (01) 49-55
- 14 Kono K, Inoue Y, Nakayama K. et al. The role of diffusion-weighted imaging in patients with brain tumors. AJNR Am J Neuroradiol 2001; 22 (06) 1081-1088
- 15 Sugahara T, Korogi Y, Kochi M. et al. Usefulness of diffusion-weighted MRI with echo-planar technique in the evaluation of cellularity in gliomas. J Magn Reson Imaging 1999; 9 (01) 53-60
- 16 Watanabe Y, Yamasaki F, Kajiwara Y. et al. Preoperative histological grading of meningiomas using apparent diffusion coefficient at 3T MRI. Eur J Radiol 2013; 82 (04) 658-663
- 17 Yamasaki F, Kurisu K, Satoh K. et al. Apparent diffusion coefficient of human brain tumors at MR imaging. Radiology 2005; 235 (03) 985-991
- 18 Hakyemez B, Yildirim N, Gokalp G, Erdogan C, Parlak M. The contribution of diffusion-weighted MR imaging to distinguishing typical from atypical meningiomas. Neuroradiology 2006; 48 (08) 513-520
- 19 Santelli L, Ramondo G, Della Puppa A. et al. Diffusion-weighted imaging does not predict histological grading in meningiomas. Acta Neurochir (Wien) 2010; 152 (08) 1315-1319 , discussion 1319
- 20 Bano S, Waraich MM, Khan MA, Buzdar SA, Manzur S. Diagnostic value of apparent diffusion coefficient for the accurate assessment and differentiation of intracranial meningiomas. Acta Radiol Short Rep 2013; 2 (07) 2047981613512484
- 21 Surov A, Gottschling S, Mawrin C. et al. Diffusion weighted imaging in meningioma: prediction of tumor grade and association with histopathological parameters. Transl Oncol 2015; 8 (06) 517-523