
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1750757
Reproducibility of Digital Planning in Cementless Total Hip Arthroplasty Among Experienced and Novice Surgeons
Artikel in mehreren Sprachen: português | English
Abstract
Objective The present study aims to assess the reproducibility of digital planning for cementless total hip arthroplasty (THA) among surgeons with different levels of experience. In addition, it attempts to determine the degree of planning reliability based on a contralateral THA or on a spherical marker positioned at the greater trochanter for calibration.
Methods Two evaluators with different experience levels (A1 and A2) performed independently the retrospective digital surgical planning of 64 cementless THAs. Next, we compared the planning with the implants used in the surgery. The reproducibility was excellent when planning and implants were identical; proper in case of a single-unit variation; and inappropriate if there was variation in two or more units. The present analysis also determined the calibration accuracy between the contralateral THA and the spherical marker at the greater trochanter level.
Results The present study demonstrated greater success when the most experienced evaluator performed the planning and greater accuracy for the contralateral THA. When splitting the analysis per parameter (contralateral THA or spherical marker), there was a statistical difference only for the planning of A1 and the implants used in the surgery. This difference occurred in the excellent category, with 67.3% for contralateral THA compared with 30.6% for a spherical marker (p<0.001), and in the inappropriate category, with 7.1% for contralateral THA compared with 30.6% for a spherical marker (p<0.001).
Conclusions Digital planning is more accurate when performed by an experienced evaluator. The contralateral prosthesis head was a better reference than a marker on the greater trochanter.
#
Keywords
arthroplasty, replacement, hip - hip prosthesis - digital planning - patient care planning - radiographyIntroduction
Total hip arthroplasty (THA) improves the quality of life of the patient by eliminating joint pain and restoring independence for basic activities of daily living.1 This positive outcome is a direct result of the durability of the surgery, which involves adequate component positioning and functional rehabilitation.[2] [3] [4]
The hip surgeon controls the proper positioning and choice of implant sizes during the procedure, and planning these factors leads to optimal outcomes.[2] [3] [4] Therefore, preoperative planning contributes to a successful surgery and benefits both experienced and novice surgeons.
Digital radiographs are increasingly common in large hospitals and clinics. Hip surgeons must adapt to this change and improve digital planning with the help of software.[5]
Some available software allow hip surgeons to calibrate the planning on digital radiographs with different magnifications. In addition, after choosing the implants, they automatically provide the offset value and the lengthening or shortening of the affected limb.[6]
During training, daily experience, repetition, and study are critical factors for the evolution of an orthopedist, probably preventing surgical complications.
The present study aims to evaluate the reproducibility of digital planning in cementless THA and to compare it according to the experience levels of a hip orthopedist and a physician undergoing hip specialization. In addition, the study proposes to compare the reliability of this planning based on the method of software calibration, that is, the contralateral THA or a spherical marker positioned at the greater trochanter.
#
Materials and Methods
The Research Committee of our institution approved the present project.
Two evaluators (A1, a hip specialist, and A2, a physician undergoing hip specialization) performed independently the retrospective surgical planning of 64 cementless THAs with no complications during a minimum follow-up period of 2 years. Patient selection occurred after an active search of medical records from the postoperative list of the institution.
How inclusion criteria, from the electronic medical records, we selected hip radiographs in an anteroposterior (AP) view in horizontal dorsal decubitus with the lower limbs in an internal rotation of ∼ 15° and the midline incident ray just above the pubic symphysis.[7] Among the selected patients, those with a spherical marker at the greater trochanter level or with a contralateral THA with a metallic head of known size remained in the study.
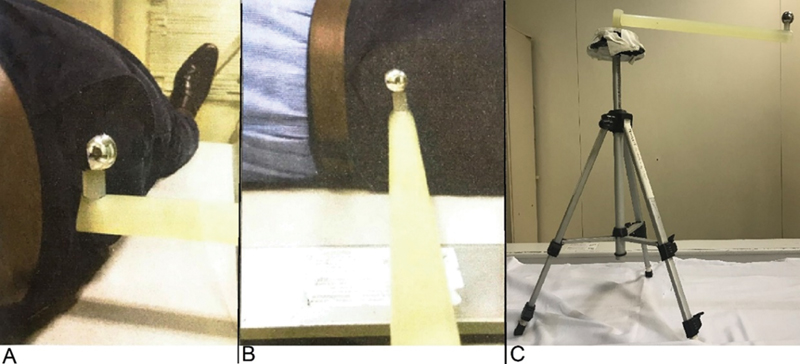
The radiograph with a spherical marker is standardized at this institute using a tripod with a 28-mm metallic head ([Figure 1]). A team of radiology technicians trained to position the sphere at the level of the greater trochanter is responsible for this test.
Arthroplasties with intraoperative complications (loss of bone stock, intraoperative fracture, instability) or requiring a revision within 2 years because of implant-related complications according to the medical records were used like exclusion criteria.
We also excluded from the study patients with no properly performed radiograph and incorrect positioned spherical marker.
The evaluators planned the size of the following components: the acetabular cup, the femoral stem, and the femoral neck. This analysis was performed with preoperative radiographs using the TraumaCad software and selecting the Targos Femoral Stem, MBA Acetabular Cup, and 28-mm metallic head implants from Groupe Lépine ([Figure 2]).

Stem and cup sizes vary from 1 to 1 and 2 to 2, respectively, and there are 3 neck sizes: - 3.5, 0, 3.5, and 7. So, if the comparison of A1 with surgery or A2 with surgery was identical, planning was excellent. Planning was proper in the case of 1 unit of variation and inappropriate in the case of ≥ 2 units of variation.
Software calibration used a 28-mm diameter metallic head with positioned at the greater trochanter level or the metallic head of known size from the contralateral THA.
The evaluators had no access to postoperative information during planning. We compared planning data with the implants used in the surgeries.
The equality of two proportions test determined planning reproducibility using either the contralateral THA or the spherical marker as parameters.
The equality of two proportions test defines whether the proportion of responses to two given variables, their levels, or both are statistically significant. In addition, we used the Wilcoxon test, which is nonparametric, to compare variables and detect differences between evaluators and calibration parameters. We also calculated the Kappa concordance index to measure the degree of agreement between two variables, results, or both. The significance level was set at 0.05% with a 95% confidence interval (CI).
The statistical analysis employed IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA), Minitab 16 (Minitab Inc., State College, PA, USA), and Microsoft Office Excel 2010 (Microsoft Corporation, Redmond, WA, USA) software.
#
Results
The study of the 64 radiographs revealed that the most experienced evaluator was better at planning and that accuracy was higher when using the contralateral THA as a parameter.
The sample had a homogeneous gender distribution, with 53.1% of women and 46.9% of men (p=0.480). However, the parameter distribution was heterogeneous, with a statistically significant majority of contralateral THAs (81.3%) compared with the spherical marker (18.8%; p<0.001) ([Table 1]).
|
n |
% |
p-value |
||
|---|---|---|---|---|
|
Gender |
Female |
34 |
53.1% |
0.480 |
|
Male |
30 |
46.9% |
||
|
Parameter |
Contralateral THA |
52 |
81.3% |
< 0.001 |
|
Spherical marker |
12 |
18.8% |
||
Initially, the total and per parameter (contralateral THA or spherical marker) analysis using the equality of two proportions test unified all implants (stem, cup, and neck).
[Table 2] shows the findings from each classification (excellent, proper, and inappropriate) according to the parameter used for planning and to the evaluator. In all parameters, the proper classification showed no difference between evaluators. The digital planning performed by A1 (expert) was excellent in 60.4% of the radiographs, compared with 26.0% for A2 (novice). This difference is statistically significant (p<0.001) ([Table 3]). The classification was inappropriate in 11.5% of the cases analyzed by A1 and in 39.6% of those assessed by A2 (p<0.001), a statistically significant finding.
|
Excellent |
Proper |
Inappropriate |
|||||
|---|---|---|---|---|---|---|---|
|
n |
% |
n |
% |
n |
% |
||
|
Contralateral THA |
Surgery – Expert (A1) |
105 |
67.3% |
40 |
25.6% |
11 |
7.1% |
|
Surgery – Novice (A2) |
44 |
28.2% |
50 |
32.1% |
62 |
39.7% |
|
|
Novice – Expert (B) |
51 |
32.7% |
55 |
35.3% |
50 |
32.1% |
|
|
Head, 28-mm |
Surgery – Expert (A1) |
11 |
30.6% |
14 |
38.9% |
11 |
30.6% |
|
Surgery – Novice (A2) |
6 |
16.7% |
16 |
44.4% |
14 |
38.9% |
|
|
Novice – Expert (B) |
13 |
36.1% |
7 |
19.4% |
16 |
44.4% |
|
|
All |
Surgery – Expert (A1) |
116 |
60.4% |
54 |
28.1% |
22 |
11.5% |
|
Surgery – Novice (A2) |
50 |
26.0% |
66 |
34.4% |
76 |
39.6% |
|
|
Novice – Expert (B) |
64 |
33.3% |
62 |
32.3% |
66 |
34.4% |
|
|
Excellent |
Proper |
Inappropriate |
||
|---|---|---|---|---|
|
Contralateral THA |
A1-A2 |
< 0.001 |
0.211 |
< 0.001 |
|
A1-B |
< 0.001 |
0.065 |
< 0.001 |
|
|
A2-B |
0.389 |
0.549 |
0.157 |
|
|
Head, 28mm |
A1-A2 |
0.165 |
0.633 |
0.458 |
|
A1-B |
0.617 |
0.070 |
0.224 |
|
|
A2-B |
0.061 |
0.023 |
0.633 |
|
|
All |
A1-A2 |
< 0.001 |
0.186 |
< 0.001 |
|
A1-B |
< 0.001 |
0.374 |
< 0.001 |
|
|
A2-B |
0.118 |
0.665 |
0.290 |
|
When fragmenting the analysis according to the parameter (contralateral THA or spherical marker), only the excellent and inappropriate plannings of A1 had statistical differences. Most excellent plannings (67.3%) used the contralateral THA as a parameter compared with 30.6% employing a spherical marker (p<0.001). For inappropriate plannings, 7.1% used the contralateral THA, and 30.6% employed a spherical marker (p<0.001). The plannings of A2 showed no statistically significant differences in the fragmented assessment.
The isolate analysis ([Table 4]) of each implant (stem, cup, and neck) revealed a statistically significant difference (p<0.001) ([Table 5]) for neck and cup with the contralateral THA as parameter. In addition, A1 was superior in plannings deemed excellent (76.9 and 67.3% for neck and cup, respectively) compared with A2 (28.8 and 23.1%, respectively). The stem analysis showed no statistical difference. Other isolated comparisons of implants with a spherical marker as a parameter revealed no statistical difference between evaluators.
|
Excellent |
Proper |
Inappropriate |
||||||
|---|---|---|---|---|---|---|---|---|
|
n |
% |
n |
% |
n |
% |
|||
|
Contralateral THA |
Neck |
Surgery – Expert (A) |
40 |
76.90% |
10 |
19.20% |
2 |
3.80% |
|
Surgery – Novice (B) |
15 |
28.80% |
13 |
25.00% |
24 |
46.20% |
||
|
Novice – Expert (C) |
14 |
26.90% |
18 |
34.60% |
20 |
38.50% |
||
|
Stem |
Surgery – Expert (A) |
30 |
57.70% |
15 |
28.80% |
7 |
13.50% |
|
|
Surgery – Novice (B) |
17 |
32.70% |
18 |
34.60% |
17 |
32.70% |
||
|
Novice – Expert (C) |
22 |
42.30% |
16 |
30.80% |
14 |
26.90% |
||
|
Cup |
Surgery – Expert (A) |
35 |
67.30% |
15 |
28.80% |
2 |
3.80% |
|
|
Surgery – Novice (B) |
12 |
23.10% |
19 |
36.50% |
21 |
40.40% |
||
|
Novice – Expert (C) |
15 |
28.80% |
21 |
40.40% |
16 |
30.80% |
||
|
Spherical marker |
Neck |
Surgery – Expert (A) |
7 |
58.30% |
5 |
41.70% |
0 |
0.00% |
|
Surgery – Novice (B) |
3 |
25.00% |
6 |
50.00% |
3 |
25.00% |
||
|
Novice – Expert (C) |
4 |
33.30% |
3 |
25.00% |
5 |
41.70% |
||
|
Stem |
Surgery – Expert (A) |
2 |
16.70% |
4 |
33.30% |
6 |
50.00% |
|
|
Surgery – Novice (B) |
1 |
8.30% |
6 |
50.00% |
5 |
41.70% |
||
|
Novice – Expert (C) |
6 |
50.00% |
1 |
8.30% |
5 |
41.70% |
||
|
Cup |
Surgery – Expert (A) |
2 |
16.70% |
5 |
41.70% |
5 |
41.70% |
|
|
Surgery – Novice (B) |
2 |
16.70% |
4 |
33.30% |
6 |
50.00% |
||
|
Novice – Expert (C) |
3 |
25.00% |
3 |
25.00% |
6 |
50.00% |
||
|
Excellent |
Proper |
Inappropriate |
|||
|---|---|---|---|---|---|
|
Contralateral THA |
Neck |
A-B |
< 0.001 |
0.478 |
< 0.001 |
|
A-C |
< 0.001 |
0.077 |
< 0.001 |
||
|
B-C |
0.827 |
0.284 |
0.427 |
||
|
Stem |
A-B |
0.01 |
0.527 |
0.02 |
|
|
A-C |
0.117 |
0.83 |
0.087 |
||
|
B-C |
0.311 |
0.676 |
0.52 |
||
|
Cup |
A-B |
< 0.001 |
0.403 |
< 0.001 |
|
|
A-C |
< 0.001 |
0.216 |
< 0.001 |
||
|
B-C |
0.502 |
0.687 |
0.306 |
||
|
Spherical marker |
Neck |
A-B |
0.098 |
0.682 |
0.064 |
|
A-C |
0.219 |
0.386 |
0.012 |
||
|
B-C |
0.653 |
0.206 |
0.386 |
||
|
Stem |
A-B |
0.537 |
0.408 |
0.682 |
|
|
A-C |
0.083 |
0.132 |
0.682 |
||
|
B-C |
0.025 |
0.025 |
1 |
||
|
Cup |
A-B |
1 |
0.673 |
0.682 |
|
|
A-C |
0.615 |
0.386 |
0.682 |
||
|
B-C |
0.615 |
0.653 |
1 |
||
#
Discussion
Digital or conventional surgical planning is the initial step toward a surgical approach and a postoperative period with fewer potential issues.2 However, inadequate magnification can give the surgeon a false sense of security. Thus, when digital planning is available, the presence of a spherical marker with a known size allows circumventing improper magnification.
Positioning the spherical marker at the greater trochanter level is an adequate method5 and a reproducible option for many cases.
However, the present study demonstrated that planning is more dependable using a contralateral THA than a spherical marker. Even an expert (A1) performed more excellent plannings when using a contralateral THA (67.3%) instead of a spherical marker (30.6%). In addition, A1 had fewer inappropriate plannings when using the contralateral THA (30.6%) instead of the spherical marker (7.1%) ([Table 2]).
Analyzing the excellence in planning for each implant, the quality of stem selection is similar. A1 was superior when choosing necks and cups, demonstrating that expertise helps selecting implants with many variables to consider for ideal planning. For instance, the cup requires considering the height of the tear, not exceeding the Kohler line, the correct angulation, and the percentage of cup coverage. This is also true when the influence of other improperly planned implants is greater, as in the case of the neck.
Even with reliable parameters, such as contralateral THA, the indexes between excellent, proper, and inappropriate plannings were statistically similar. Thus, for a novice surgeon, training in digital planning and the presence of a more experienced colleague are essential for the success of the surgery.
Moreover, we need to improve spherical marker positioning methods. This improvement could increase the spherical marker reproducibility to levels statistically closer to those obtained with the contralateral THA.
#
#
Conflito de interesses
Os autores declaram não haver conflito de interesses.
Study developed at the Hip and Arthroplasties Group, Institute of Orthopedics and Traumatology, Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo, SP, Brazil.
-
Referências
- 1 Schwartsmann CR, Boschin LC. Quadril do adulto. In: Herbert S, Barros Filho TEP, Xavier R, Pardini Junior A, eds. Ortopedia e traumatologia: princípios e prática 4ª. ed. Porto Alegre: Artmed; 2009: 407-442
- 2 Muller ME. Total hip replacement: planning, technique and complications. In: Cruess RL, Mitchell NS, eds. Surgical management of degenerative arthritis of the lower limb. Philadelphia: Lea & Faber; 1975: 90-113
- 3 Müller ME. Lessons of 30 years of total hip arthroplasty. Clin Orthop Relat Res 1992; (274) 12-21
- 4 Knight JL, Atwater RD. Preoperative planning for total hip arthroplasty. Quantitating its utility and precision. J Arthroplasty 1992; 7 (Suppl): 403-409
- 5 Polesello GC, Salerno TT, Rezende JHZ, de Queiroz MC, Rabelo ND, Ricioli Junior W. Is it Important to Know Where to Place the Spherical Marker for Hip Replacement Digital Planning?. Rev Bras Ortop (Sao Paulo) 2020; 55 (03) 353-359
- 6 TraumaCad® Joints. BRAINLAB, 25/04/2021. Acesso em: 20 de maio de 2021. Disponível em: https://www.traumacad.com/pdf/MK2U00579_C_TraumaCad_Joints_Brochure_EN_DIGITAL.pdf
- 7 Polesello GC, Nakao TS, Queiroz MC. et al. Proposta de padronização do estudo radiográfico do quadril e da pelve. Rev Bras Ortop 2011; 46 (06) 634-642
Endereço para correspondência
Publikationsverlauf
Eingereicht: 21. Juli 2021
Angenommen: 24. September 2021
Artikel online veröffentlicht:
05. September 2022
© 2022. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Schwartsmann CR, Boschin LC. Quadril do adulto. In: Herbert S, Barros Filho TEP, Xavier R, Pardini Junior A, eds. Ortopedia e traumatologia: princípios e prática 4ª. ed. Porto Alegre: Artmed; 2009: 407-442
- 2 Muller ME. Total hip replacement: planning, technique and complications. In: Cruess RL, Mitchell NS, eds. Surgical management of degenerative arthritis of the lower limb. Philadelphia: Lea & Faber; 1975: 90-113
- 3 Müller ME. Lessons of 30 years of total hip arthroplasty. Clin Orthop Relat Res 1992; (274) 12-21
- 4 Knight JL, Atwater RD. Preoperative planning for total hip arthroplasty. Quantitating its utility and precision. J Arthroplasty 1992; 7 (Suppl): 403-409
- 5 Polesello GC, Salerno TT, Rezende JHZ, de Queiroz MC, Rabelo ND, Ricioli Junior W. Is it Important to Know Where to Place the Spherical Marker for Hip Replacement Digital Planning?. Rev Bras Ortop (Sao Paulo) 2020; 55 (03) 353-359
- 6 TraumaCad® Joints. BRAINLAB, 25/04/2021. Acesso em: 20 de maio de 2021. Disponível em: https://www.traumacad.com/pdf/MK2U00579_C_TraumaCad_Joints_Brochure_EN_DIGITAL.pdf
- 7 Polesello GC, Nakao TS, Queiroz MC. et al. Proposta de padronização do estudo radiográfico do quadril e da pelve. Rev Bras Ortop 2011; 46 (06) 634-642

