

Subscribe to RSS
DOI: 10.1055/s-0042-1754410
Temporal Trend and Risk Factors for Respiratory Distress Syndrome–Associated Neonatal Mortality in Preterm Infants: A Population-Based Study in a Middle-Income Country
Authors
Funding This research was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Project number 2017/03748-7; however, it has no role in any step of the study and report (including study design, analysis and interpretation of data, in the writing of the report, or in the decision to submit the paper for publication), which was authors' responsibility.

Abstract
Objective This article aimed to report a temporal series of respiratory distress syndrome (RDS)-associated neonatal mortality rates in preterm live births in São Paulo state, Brazil, and to identify social, maternal, and neonatal characteristics associated with these deaths.
Study Design This is a population-based study of all live births with gestational age (GA) between 22 and 36 weeks, birth weight ≥400 g, without congenital anomalies from mothers living in São Paulo state during 2004 to 2015. RDS-associated neonatal mortality was defined as death up to 27 days after birth with ICD-10 codes P22.0 or P28.0. RDS-associated neonatal mortality rate (annual percent change [APC] with 95% confidence intervals [95% CIs]) was analyzed by Prais–Winsten. Kaplan–Meier estimator identified the time after birth that the RDS-associated neonatal death occurred. Poisson's regression model compared social maternal and neonatal characteristics between preterm live births that survived the neonatal period and those with RDS-associated neonatal deaths, with results expressed in incidence rate ratio and 95% CI.
Results A total of 645,276 preterm live births were included in the study, of which 612,110 survived and 11,078 had RDS-associated neonatal deaths. RDS-associated neonatal mortality rate was 17.17 per thousand preterm live births, with a decreasing annual trend (APC: −6.50%; 95% CI: −9.11 to −3.82%). The median time of these deaths was 48 hours after birth. The following risk factors for RDS-associated neonatal death were identified: maternal schooling ≤7 years (1.18; 1.09–1.29), zero to three prenatal care visits (1.25; 1.18–1.32), multiple pregnancy (1.24; 1.16–1.33), vaginal delivery (1.29; 1.22–1.36), GA 22 to 27 weeks (106.35; 98.36–114.98), GA 28 to 31 weeks (20.12; 18.62–21.73), male sex (1.16; 1.10–1.22), and 5-minute Apgar scores of 0 to 3 (6.74; 6.08–7.47) and 4 to 6 (3.97; 3.72–4.23).
Conclusion During the study period, RDS-associated neonatal mortality rates showed significant reduction. The relationship between RDS-associated neonatal deaths and social, maternal, and neonatal factors suggests the need for perinatal strategies to reduce prematurity and to improve the initial management of preterm infants.
Key Points
-
RDS is associated with preterm live births.
-
Impact of RDS-associated neonatal mortality in middle-income countries is scarce.
-
Qualified perinatal care can reduce RDS-associated neonatal mortality.
Keywords
infant - premature - respiratory distress syndrome - newborn - neonatal mortality - epidemiological studies - factors - riskRespiratory distress syndrome (RDS) is the most common respiratory disorder and an important cause of neonatal deaths in preterm infants.[1] For many middle-income countries, the incidence of prematurity[2] and respiratory diseases is unknown[3] due to the limited available data on preterm births.[2] Nevertheless, single-center studies show that RDS is an important cause of neonatal death, varying from 13.6 (China) to 738 (Iran) RDS-associated neonatal deaths per thousand preterm live births.[3] [4]
Brazil is an upper middle-income country that showed improvements in the past 20 years in maternal and child health care coverage.[5] In the same period, advances in the collection and availability of health data by Brazilian federal system were also observed, ensuring more than 95% of live births coverage in 2015.[6] An idea of the RDS impact on morbidity and mortality of preterm neonates in the country was provided by the Brazilian Network on Neonatal Research, which has a prospective database of all very low birth weight live births in 20 referral public university hospitals. Among 1,438 very low birth weight preterm live births in 2015 with gestational age between 23 and 33 weeks, 70% presented with RDS.[7] In these infants, there was an association between RDS and unfavorable outcomes, such as in-hospital death or the presence of severe morbidity defined as one or more of the following: bronchopulmonary dysplasia, severe intraventricular hemorrhage, periventricular leukomalacia, or surgical retinopathy of prematurity.[8]
Located in the southeast region of the country, São Paulo is the richest and most populous Brazilian state.[9] Besides the federal government information system, it has its own vital statistics system that captures 99.5% of the data present in civil records.[10] Data on RDS frequency and impact in São Paulo, as in the rest of the country, are sparse. In a reference center in São Paulo city, RDS increased the risk of death in preterm live births (68%).[11] For very low birth weight preterm infants in one city of São Paulo state, severe RDS increased the mortality risk by 18 times.[12]
Considering the RDS impact on neonatal mortality described in single-center studies of São Paulo state, Brazil, our aim was to report a temporal series of RDS-associated neonatal mortality rates in preterm live births over a 12-year period, and to identify social, maternal, and neonatal characteristics associated with these deaths.
Materials and Methods
This is a population-based study of all live births from mothers living in São Paulo state, Brazil, between 2004 and 2015. Neonatal deaths and live births data were obtained from “Fundação Sistema Estadual de Análise de Dados” (SEADE Foundation). The death database was composed by records of neonatal deaths linked to the live birth records using deterministic linkage. The study was approved by the Ethics Committee of Universidade Federal de São Paulo, under the number 4.055.489, with waived informed consent.
All preterm live births with gestational age between 22 and 36 weeks were included in the study. Exclusion criteria were birth weight <400 g or congenital anomalies registered in the birth or in the death certificate. The following definitions were used: neonatal death—preterm live birth that died within 27 days after birth; RDS-associated neonatal death—any neonatal death with the following ICD-10 codes in any line of the Death Certificate, P22.0 (RDS of newborn) or P28.0 (primary atelectasis of newborn)[13]; and RDS-associated neonatal mortality rate—number of RDS-associated neonatal deaths per thousand preterm live births.
The following demographic characteristics were studied for preterm live births that survived the neonatal period and those with RDS-associated neonatal deaths: maternal age (<20, 20–34, and ≥35 years), marital status (married or unmarried), maternal schooling (≤7, 8–11, and ≥12 years), parity (primiparous or multiparous), number of prenatal care visits (0–3 and ≥4), pregnancy (single or multiple), delivery mode (vaginal or cesarean section), gestational age (22–27, 28–31, and 32–36 weeks), birth weight (<1,000, 1,000–1,499 g, and ≥1,500 g), sex (male or female), and 5-minute Apgar score (0–3, 4–6, and ≥7).
The annual trend of RDS-associated neonatal mortality rate was analyzed by Prais–Winsten model.[14] This analysis considers the first and last rates and estimates the annual percent change (APC) with 95% confidence intervals (95% CI). APC is classified as stationary in time, increasing, or decreasing. For non-stationary trends in time, the Poisson model was modeled with year as the only independent variable, allowing to calculate, for each year, the incidence rate ratio (IRR) and the 95% CI, considering 2004 as the comparison.
Kaplan–Meier estimator was applied to identify the time after birth that the RDS-associated neonatal death occurred for each gestational age group during the 12-year study period. Considering competing risks, Kaplan–Meier was done only with preterm live births that survived the neonatal period and with RDS-associated neonatal deaths. Non–RDS-associated neonatal deaths were excluded from this analysis.
Poisson regression models were used including preterm live births that survived the neonatal period and those with RDS-associated neonatal deaths. Birth weight was excluded from the regression models due to the collinearity with gestational age. First, Poisson univariate analysis adjusted by year of birth was applied. Next, all significant variables were included in a multivariate model adjusted by year of birth, considering three blocks: (1) social variables: maternal age, marital status, and maternal schooling; (2) maternal variables: parity, number of prenatal care visits, delivery mode, and type of pregnancy; and (3) neonatal variables: gestational age, sex, and 5-minute Apgar score. All significant variables were included in a multivariate regression model. All procedures were done using Stata 15.1 (StataCorp LLC, Texas).
Results
From 2004 to 2015, there were 7,317,611 live births in São Paulo state, Brazil. Among them, 662,856 (9.1%) were preterm live births, and 645,276 (97.3%) were included in the study. Of these, 612,110 (94.9%) survived and 33,166 (5.1%) died during the first 27 days of birth, with 11,078 (33.4%) of these deaths classified as RDS-associated neonatal deaths ([Fig. 1]).

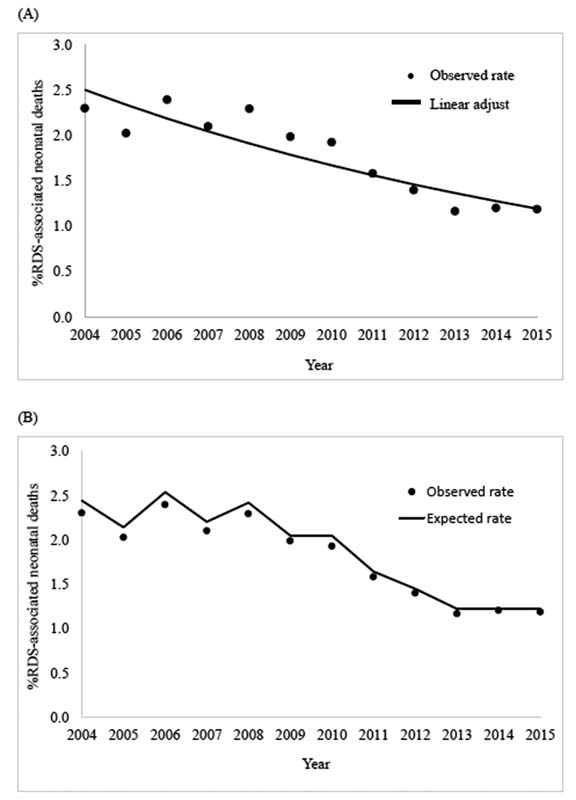
RDS-associated neonatal mortality rate, during 12-year study period, was 17.17 per thousand preterm live births ([Table 1]). The annual trend of RDS-associated neonatal mortality rate showed a decreasing pattern, with a negative APC (−6.50%; 95% CI: −9.11 to −3.82%) ([Fig. 2A]). Compared with 2004, the Poisson regression analysis showed a reduction of RDS-associated neonatal mortality in 2005 (IRR: 0.88; 95% CI: 0.80–0.96), 2007 (IRR: 0.90; 95% CI: 0.83–0.99), 2009 and 2010 (IRR: 0.84; 95% CI: 0.78–0.91), 2011 (IRR: 0.67; 95% CI: 0.61–0.74), 2012 (IRR: 0.59; 95% CI: 0.54–0.65), and 2013 to 2015 (IRR: 0.50; 95% CI: 0.47–0.54). For the years 2006 and 2008, RDS-associated neonatal mortality rates were similar to 2004 ([Fig. 2B]).
Abbreviations: N, total number; RDS, respiratory distress syndrome.
Kaplan–Meier analysis showed that the median time of these deaths was 48 hours after birth. According to gestational age, these deaths occurred with a median of 38 hours for preterm infants with gestational age of 22 to 27 weeks, and 68 hours for those with 28 to 36 weeks ([Supplementary Fig. S1] [online only]).
Most demographic variables were almost fully available, except for maternal married status, schooling, parity, and 5-minute Apgar score. For the latter variables, information was available for more than 75% of the studied live births ([Table 2]). In the multivariate regression analysis, less maternal schooling, lower number of prenatal care visits, multiple pregnancy, vaginal delivery, lower gestational age, male sex, and lower 5-minute Apgar score were risk factors for RDS-associated neonatal deaths ([Table 3]).
Abbreviations: C-section, cesarean section; n, number; RDS, respiratory distress syndrome.
Abbreviation: RDS, respiratory distress syndrome.
Notes: Univariate analysis was adjusted by year of birth; multivariate analysis (significant variables) was adjusted for maternal age, maternal schooling, prenatal care visit, type of pregnancy, delivery mode, gestational age, sex, and 5-minute Apgar score. Analyses were expressed as incidence rate ratio and 95% confidence interval.
Discussion
This population-based study evaluated the temporal trend of RDS-associated neonatal mortality in preterm live births and the characteristics associated with these deaths, in São Paulo state, Brazil. During a 12-year period, there was a significant reduction of RDS-associated neonatal mortality rates. The deaths occurred mostly in the first 3 days after birth. Social (lower maternal schooling), maternal (lower number of prenatal care visits, multiple pregnancy, and vaginal delivery), and neonatal factors (lower gestational age, male sex, and lower 5-minute Apgar score) were associated with these deaths.
In middle-income countries, RDS rates have been rising over the years.[3] Adequate prenatal care, use of antenatal corticosteroids, surfactant administration, and early continuous positive airway pressure (CPAP) are considered as good practices for RDS management.[15] Since 2004, Brazilian perinatal centers are reporting increase in the antenatal corticosteroids use, in the surfactant administration, and in the early CPAP for preterm live births <34 weeks of gestation.[7] Despite the fact that our database does not provide information about these practices, the reduction of RDS-associated mortality rate probably reflects improvements in the management of preterm infants during the study period.
Despite the reduction of RDS-associated neonatal mortality, the rate of 17.17 per thousand preterm live births found in our study is higher than the rates reported in high-income countries. In Italy, according to information retrieved from the Lombardy regional database, there was 10.40 RDS-associated neonatal deaths per thousand preterm live births with 23 to 36 weeks of gestation between 2010 and 2013.[16] São Paulo state RDS outcomes may be impacted by deficiencies in health care system organization, scarce policies for quality improvement, inequity in access to qualified care,[5] and disparity in utilization of perinatal healthcare resources,[17] with difficulties in access to appropriate antenatal care, especially for mothers with lower socioeconomic status.[18]
In our study, lower maternal schooling and lower prenatal care visits were associated with RDS neonatal mortality. Adequate prenatal care may prevent, detect, and treat risk factors for bad pregnancy outcomes; it may allow a pre-assignment hospital for the delivery, and ensure maternal safe transfer to a reference perinatal center for high-risk pregnancies. Among all these benefits, it includes a higher chance of receiving antenatal corticosteroids for women at risk for preterm delivery,[11] [15] [19] and an opportune indication of cesarean section, if needed.[20] In São Paulo state (2004–2013), cesarean section was protective for neonatal deaths by 37% in 22 to 27 weeks of gestation live births, and by 11% for those with 28 to 32 weeks of gestation.[21] In an Indian single-center study, vaginal delivery increased the risk for RDS-associated neonatal deaths in live births with 28 to 34 weeks of gestation by almost 17 times.[19]
The association between lower 5-Apgar score and RDS-associated neonatal deaths found in our study is probably related to inequities in the access of women at risk for preterm delivery and their newborn infants to high-quality care, associated with deficiencies in antenatal and delivery care, and in the initial postnatal management. Similar to our study, in Fiji, a lower 5-Apgar score increased the death risk among newborns with RDS.[22]
The finding that RDS-associated neonatal deaths occurred in the first 2 to 3 days after birth was similar to the timing observed for neonatal deaths associated with perinatal asphyxia in São Paulo state in the same period, suggesting that the main problem in the region of the study is not access to health care but access to qualified health care.[23] In northeast Brazil, a poorer hospital infrastructure was associated with a higher frequency of very low birth weight deaths in the first 24 hours after birth.[24] In eight Brazilian states, between 2010 and 2015, RDS was the major cause of neonatal death in the first 24 hours after birth.[25] In China, one retrospective study, including data from 39 referral neonatal intensive care units, reported that almost 50% of RDS-associated neonatal deaths in extremely low birth weight occurred during the first 48 hours after birth.[26]
Our study also showed that RDS-associated neonatal deaths among 22 to 27 weeks of gestational age occurred mostly during the first 38 hours after birth, earlier than those with 28 to 36 weeks of gestational age. Earlier deaths in the more immature infants were also reported in another Brazilian study and in China.[26] [27] In the Brazilian Surfactant Collaborative Group, with 19 centers, almost 40% of deaths of preterm infants with birth weight less than 750 g occurred during the first 72 hours after birth, compared with 5% of deaths within this period in infants with higher birth weight.[27] Lower gestational age, multiple pregnancy, and male sex are considered biological conditions with higher vulnerability for bad outcomes,[28] and, probably, with the presence of more severe disease in the first hours of life.[29] Infants with these characteristics may demand the availability of complex resources to ensure the adequate respiratory care and reduce the risk of death.[30] But quality of care is much more than the availability of technological resources.[31] To achieve the best outcomes, trained human resources, standardized care management based on best available scientific evidence, and continuous surveillance of the quality of care are necessary.[32] In Brazil, the partnership among 49 neonatal units, all over the country, with the Vermont-Oxford Network, shows the increasing pursuit for offering better neonatal care.[33] On the other hand, several Brazilian neonatal intensive care teams are still composed by high number of nonspecialist nurses, working in units without continued education initiatives, and with inadequate ratio of patients per nurse, which are problems that may impair the quality of care[34] and contribute to the high frequency of RDS-associated neonatal deaths during the first few days after birth in vulnerable preterm live births.
The present study has limitations. This is a population-based study performed using a database built from birth and death certificates that does not include information related to maternal conditions, such as chorioamnionitis and preeclampsia, which could impact in preterm births and RDS-associated neonatal mortality. In addition, accuracy of critical variables for this study such as gestational age and diagnosis codes of causes of death cannot be checked. Despite the risk of information bias, the data provided by SEADE Foundation is based on improved deterministic linkage method of death and live birth certificates, ensuring consistent and detailed information for epidemiologic studies.[10] On the other hand, the linkage process has a manual component, and it is time consuming; therefore, 2015 is the most recent year data available for the study.
This study is one of the first population-based analysis of a temporal trend of RDS-associated neonatal deaths in a middle-income country and their associated factors. The temporal trend of one of the main causes of death in preterm infants found in this study and the variables associated to these deaths highlight the unique characteristics of the health care provided to mother–infant dyads in regions such as São Paulo state of Brazil, where issues related to quality of care need special attention. Discussion of perinatal care should not classify low- and middle-income settings as a homogeneous group with similar problems.
In conclusion, during a 12-year period in São Paulo state, Brazil, RDS-associated neonatal mortality rate showed a significant reduction, but it is still high compared with rates reported in high-income countries. The relationship between RDS-associated neonatal deaths and social, maternal, and neonatal factors suggests the need for perinatal strategies to reduce prematurity and to improve the initial management of preterm infants.
Conflict of Interest
None declared. Database use was possible due to FAPESP (Project number 2017/03748–7) and due to agreements numbers 23089.004297/2008–11 and 23089.000057/2014–95 between Fundação SEADE and Universidade Federal de São Paulo.
Acknowledgments
We thank FAPESP for the funding, all technical staff of SEADE Foundation for their work with the database, and Josiane Quintiliano Xavier de Castro, MD, for helping in the deterministic linkage between live birth certificates and death certificates.
-
References
- 1 McPherson C, Wambach JA. Prevention and treatment of respiratory distress syndrome in preterm neonates. Neonatal Netw 2018; 37 (03) 169-177
- 2 Chawanpaiboon S, Vogel JP, Moller AB. et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health 2019; 7 (01) e37-e46
- 3 Sun H, Xu F, Xiong H. et al. Characteristics of respiratory distress syndrome in infants of different gestational ages. Lung 2013; 191 (04) 425-433
- 4 Basiri B, Ashari FE, Shokouhi M, Sabzehei MK. Neonatal mortality and its main determinants in premature infants hospitalized in neonatal intensive care unit in Fatemieh Hospital, Hamadan, Iran. J Compr Ped 2015; 6 (03) e26965
- 5 Victora CG, Aquino EML, do Carmo Leal M, Monteiro CA, Barros FC, Szwarcwald CL. Maternal and child health in Brazil: progress and challenges. Lancet 2011; 377 (9780): 1863-1876
- 6 IBGE. Sistemas de estatísticas vitais no Brasil: avanços, perspectivas e desafios. Rio de Janeiro: Ministério do Planejamento, Desenvolvimento e Gestão. 2018 Accessed October 26, 2021 at: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101575.pdf
- 7 Rede Brasileira de Pesquisas Neonatais. Relatórios Anuais. Accessed September 03, 2021 at: http://www.redeneonatal.fiocruz.br/index.php/10-destaque/29-relatoriosanuais
- 8 Guinsburg R, de Almeida MF, de Castro JS. et al. Death or survival with major morbidity in VLBW infants born at Brazilian neonatal research network centers. J Matern Fetal Neonatal Med 2016; 29 (06) 1005-1009
- 9 IBGE. Censo Demográfico 2010 - resultados gerais da amostra. Rio de Janeiro: Ministério do Planejamento, Orçamento e Gestão;. 2012 . Accessed September 25, 2020 at: https://biblioteca.ibge.gov.br/visualizacao/periodicos/99/cd_2010_resultados_gerais_amostra.pdf
- 10 Waldvogel BC, Ferreira CEC, Camargo ABM, Jordani MS, Ortiz LP. Base unificada de nascimentos e óbitos no estado de São Paulo. São Paulo em Perspectiva 2008; 22 (01) 5-18
- 11 Meneguel JF, Guinsburg R, Miyoshi MH. et al. Antenatal treatment with corticosteroids for preterm neonates: impact on the incidence of respiratory distress syndrome and intra-hospital mortality. Sao Paulo Med J 2003; 121 (02) 45-52
- 12 Prigenzi MHL, Trindade CEP, Rugolo LMSS, Silveira LVA. Fatores de risco associados à mortalidade de recém-nascidos de muito baixo peso na cidade de Botucatu, São Paulo, no período 1995–2000. Rev Bras Saúde Mater Infant 2008; 8 (01) 93-101
- 13 WHO. ICD-10: International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. 2nd ed. Geneva: World Health Organization; 2004
- 14 Prais SJ, Winsten CB. Trend Estimators and Serial Correlation. Chicago: Cowles Commission; 1954: 1-27
- 15 Sweet D, Bevilacqua G, Carnielli V. et al; Working Group on Prematurity of the World Association of Perinatal Medicine, European Association of Perinatal Medicine. European consensus guidelines on the management of neonatal respiratory distress syndrome. J Perinat Med 2007; 35 (03) 175-186
- 16 Condò V, Cipriani S, Colnaghi M. et al. Neonatal respiratory distress syndrome: are risk factors the same in preterm and term infants?. J Matern Fetal Neonatal Med 2017; 30 (11) 1267-1272
- 17 Tapia JL, Toso A, Vaz Ferreira C. et al. The unfinished work of neonatal very low birthweight infants quality improvement: Improving outcomes at a continental level in South America. Semin Fetal Neonatal Med 2021; 26 (01) 101193
- 18 Domingues RMSM, Viellas EF, Dias MAB. et al. [Adequacy of prenatal care according to maternal characteristics in Brazil]. Rev Panam Salud Publica 2015; 37 (03) 140-147
- 19 Gahlawat V, Chellani H, Saini I, Gupta S. Predictors of mortality in premature babies with respiratory distress syndrome treated by early rescue surfactant therapy. J Neonatal Perinatal Med 2021; 14 (04) 547-552
- 20 Betran AP, Torloni MR, Zhang JJ, Gülmezoglu AM. WHO Working Group on Caesarean Section. WHO statement on caesarean section rates. BJOG 2016; 123 (05) 667-670
- 21 Guinsburg R, Sanudo A, Kiffer CRV. et al. Annual trend of neonatal mortality and its underlying causes: population-based study - São Paulo State, Brazil, 2004-2013. BMC Pediatr 2021; 21 (01) 54
- 22 Szanyi J, Tuibeqa I, Ratu T. et al. The epidemiology of respiratory distress syndrome in neonates in Fiji: a retrospective cohort study. Pacific Health 2019; 2: 1-16
- 23 Kawakami MD, Sanudo A, Teixeira MLP. et al. Neonatal mortality associated with perinatal asphyxia: a population-based study in a middle-income country. BMC Pregnancy Childbirth 2021; 21 (01) 169
- 24 Castro ECM, Leite AJM, Guinsburg R. [Mortality in the first 24h of very low birth weight preterm infants in the Northeast of Brazil]. Rev Paul Pediatr 2016; 34 (01) 106-113
- 25 Teixeira JAM, Araujo WRM, Maranhão AGK, Cortez-Escalante JJ, Rezende LFM, Matijasevich A. Mortality on the first day of life: trends, causes of death and avoidability in eight Brazilian Federative Units, between 2010 and 2015. Epidemiol Serv Saude 2019; 28 (01) e2018132
- 26 Zhou J, Ba Y, Du Y, Lin SB, Chen C. Chinese Collaborative Study Group for Etiologies of NICU Deaths. The etiology of neonatal intensive care unit death in extremely low birth weight infants: a multicenter survey in China. Am J Perinatol 2021; 38 (10) 1048-1056
- 27 Rebello CM, Precioso AR, Mascaretti RS. Grupo Colaborativo do Estudo Brasileiro Multicêntrico de Surfactante. A multicenter, randomized, double-blind trial of a new porcine surfactant in premature infants with respiratory distress syndrome. Einstein (Sao Paulo) 2014; 12 (04) 397-404
- 28 Boghossian NS, Geraci M, Edwards EM, Horbar JD. Sex differences in mortality and morbidity of infants born at less than 30 weeks' gestation. Pediatrics 2018; 142 (06) e20182352
- 29 John BM, Venkateshwar V, Dagar V. Predictors of outcome in neonates with respiratory distress. J Nepal Paediatr Soc 2015; 35 (01) 31-37
- 30 Chang JH, Hsu CH, Tsou KI, Jim WT. Taiwan Premature Infant Developmental Collaborative Study Group. Outcomes and related factors in a cohort of infants born in Taiwan over a period of five years (2007-2011) with borderline viability. J Formos Med Assoc 2018; 117 (05) 365-373
- 31 Spitzer AR. Has quality improvement really improved outcomes for babies in the neonatal intensive care unit?. Clin Perinatol 2017; 44 (03) 469-483
- 32 Biban P, Marlow N, Te Pas AB, Fanaroff AA, Jobe AH. Advances in neonatal critical care: pushing at the boundaries and connecting to long-term outcomes. Crit Care Med 2021; 49 (12) 2003-2016
- 33 Rede Brasileira de Pesquisas Neonatais. Histórico da Rede Brasileira de Pesquisas Neonatais. 2019 . Accessed October 25, 2020 at: https://redeneonatal.com.br/historico-da-rede-brasileira-de-pesquisas-neonatais/
- 34 Torres LM, Paiva ABF, Diniz AEO. et al. Nursing care to newborns with respiratory distress syndrome in intensive care unit. Int Arch Med 2016; 9 (80) 1-8
Address for correspondence
Publication History
Received: 05 December 2021
Accepted: 01 June 2022
Article published online:
16 August 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 McPherson C, Wambach JA. Prevention and treatment of respiratory distress syndrome in preterm neonates. Neonatal Netw 2018; 37 (03) 169-177
- 2 Chawanpaiboon S, Vogel JP, Moller AB. et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health 2019; 7 (01) e37-e46
- 3 Sun H, Xu F, Xiong H. et al. Characteristics of respiratory distress syndrome in infants of different gestational ages. Lung 2013; 191 (04) 425-433
- 4 Basiri B, Ashari FE, Shokouhi M, Sabzehei MK. Neonatal mortality and its main determinants in premature infants hospitalized in neonatal intensive care unit in Fatemieh Hospital, Hamadan, Iran. J Compr Ped 2015; 6 (03) e26965
- 5 Victora CG, Aquino EML, do Carmo Leal M, Monteiro CA, Barros FC, Szwarcwald CL. Maternal and child health in Brazil: progress and challenges. Lancet 2011; 377 (9780): 1863-1876
- 6 IBGE. Sistemas de estatísticas vitais no Brasil: avanços, perspectivas e desafios. Rio de Janeiro: Ministério do Planejamento, Desenvolvimento e Gestão. 2018 Accessed October 26, 2021 at: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101575.pdf
- 7 Rede Brasileira de Pesquisas Neonatais. Relatórios Anuais. Accessed September 03, 2021 at: http://www.redeneonatal.fiocruz.br/index.php/10-destaque/29-relatoriosanuais
- 8 Guinsburg R, de Almeida MF, de Castro JS. et al. Death or survival with major morbidity in VLBW infants born at Brazilian neonatal research network centers. J Matern Fetal Neonatal Med 2016; 29 (06) 1005-1009
- 9 IBGE. Censo Demográfico 2010 - resultados gerais da amostra. Rio de Janeiro: Ministério do Planejamento, Orçamento e Gestão;. 2012 . Accessed September 25, 2020 at: https://biblioteca.ibge.gov.br/visualizacao/periodicos/99/cd_2010_resultados_gerais_amostra.pdf
- 10 Waldvogel BC, Ferreira CEC, Camargo ABM, Jordani MS, Ortiz LP. Base unificada de nascimentos e óbitos no estado de São Paulo. São Paulo em Perspectiva 2008; 22 (01) 5-18
- 11 Meneguel JF, Guinsburg R, Miyoshi MH. et al. Antenatal treatment with corticosteroids for preterm neonates: impact on the incidence of respiratory distress syndrome and intra-hospital mortality. Sao Paulo Med J 2003; 121 (02) 45-52
- 12 Prigenzi MHL, Trindade CEP, Rugolo LMSS, Silveira LVA. Fatores de risco associados à mortalidade de recém-nascidos de muito baixo peso na cidade de Botucatu, São Paulo, no período 1995–2000. Rev Bras Saúde Mater Infant 2008; 8 (01) 93-101
- 13 WHO. ICD-10: International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. 2nd ed. Geneva: World Health Organization; 2004
- 14 Prais SJ, Winsten CB. Trend Estimators and Serial Correlation. Chicago: Cowles Commission; 1954: 1-27
- 15 Sweet D, Bevilacqua G, Carnielli V. et al; Working Group on Prematurity of the World Association of Perinatal Medicine, European Association of Perinatal Medicine. European consensus guidelines on the management of neonatal respiratory distress syndrome. J Perinat Med 2007; 35 (03) 175-186
- 16 Condò V, Cipriani S, Colnaghi M. et al. Neonatal respiratory distress syndrome: are risk factors the same in preterm and term infants?. J Matern Fetal Neonatal Med 2017; 30 (11) 1267-1272
- 17 Tapia JL, Toso A, Vaz Ferreira C. et al. The unfinished work of neonatal very low birthweight infants quality improvement: Improving outcomes at a continental level in South America. Semin Fetal Neonatal Med 2021; 26 (01) 101193
- 18 Domingues RMSM, Viellas EF, Dias MAB. et al. [Adequacy of prenatal care according to maternal characteristics in Brazil]. Rev Panam Salud Publica 2015; 37 (03) 140-147
- 19 Gahlawat V, Chellani H, Saini I, Gupta S. Predictors of mortality in premature babies with respiratory distress syndrome treated by early rescue surfactant therapy. J Neonatal Perinatal Med 2021; 14 (04) 547-552
- 20 Betran AP, Torloni MR, Zhang JJ, Gülmezoglu AM. WHO Working Group on Caesarean Section. WHO statement on caesarean section rates. BJOG 2016; 123 (05) 667-670
- 21 Guinsburg R, Sanudo A, Kiffer CRV. et al. Annual trend of neonatal mortality and its underlying causes: population-based study - São Paulo State, Brazil, 2004-2013. BMC Pediatr 2021; 21 (01) 54
- 22 Szanyi J, Tuibeqa I, Ratu T. et al. The epidemiology of respiratory distress syndrome in neonates in Fiji: a retrospective cohort study. Pacific Health 2019; 2: 1-16
- 23 Kawakami MD, Sanudo A, Teixeira MLP. et al. Neonatal mortality associated with perinatal asphyxia: a population-based study in a middle-income country. BMC Pregnancy Childbirth 2021; 21 (01) 169
- 24 Castro ECM, Leite AJM, Guinsburg R. [Mortality in the first 24h of very low birth weight preterm infants in the Northeast of Brazil]. Rev Paul Pediatr 2016; 34 (01) 106-113
- 25 Teixeira JAM, Araujo WRM, Maranhão AGK, Cortez-Escalante JJ, Rezende LFM, Matijasevich A. Mortality on the first day of life: trends, causes of death and avoidability in eight Brazilian Federative Units, between 2010 and 2015. Epidemiol Serv Saude 2019; 28 (01) e2018132
- 26 Zhou J, Ba Y, Du Y, Lin SB, Chen C. Chinese Collaborative Study Group for Etiologies of NICU Deaths. The etiology of neonatal intensive care unit death in extremely low birth weight infants: a multicenter survey in China. Am J Perinatol 2021; 38 (10) 1048-1056
- 27 Rebello CM, Precioso AR, Mascaretti RS. Grupo Colaborativo do Estudo Brasileiro Multicêntrico de Surfactante. A multicenter, randomized, double-blind trial of a new porcine surfactant in premature infants with respiratory distress syndrome. Einstein (Sao Paulo) 2014; 12 (04) 397-404
- 28 Boghossian NS, Geraci M, Edwards EM, Horbar JD. Sex differences in mortality and morbidity of infants born at less than 30 weeks' gestation. Pediatrics 2018; 142 (06) e20182352
- 29 John BM, Venkateshwar V, Dagar V. Predictors of outcome in neonates with respiratory distress. J Nepal Paediatr Soc 2015; 35 (01) 31-37
- 30 Chang JH, Hsu CH, Tsou KI, Jim WT. Taiwan Premature Infant Developmental Collaborative Study Group. Outcomes and related factors in a cohort of infants born in Taiwan over a period of five years (2007-2011) with borderline viability. J Formos Med Assoc 2018; 117 (05) 365-373
- 31 Spitzer AR. Has quality improvement really improved outcomes for babies in the neonatal intensive care unit?. Clin Perinatol 2017; 44 (03) 469-483
- 32 Biban P, Marlow N, Te Pas AB, Fanaroff AA, Jobe AH. Advances in neonatal critical care: pushing at the boundaries and connecting to long-term outcomes. Crit Care Med 2021; 49 (12) 2003-2016
- 33 Rede Brasileira de Pesquisas Neonatais. Histórico da Rede Brasileira de Pesquisas Neonatais. 2019 . Accessed October 25, 2020 at: https://redeneonatal.com.br/historico-da-rede-brasileira-de-pesquisas-neonatais/
- 34 Torres LM, Paiva ABF, Diniz AEO. et al. Nursing care to newborns with respiratory distress syndrome in intensive care unit. Int Arch Med 2016; 9 (80) 1-8