

Subscribe to RSS
DOI: 10.1055/s-0042-1756205
Arterial Vascularization of the Fingers: Anatomy and Clinical Applications in Reconstructive Surgery
Article in several languages: español | EnglishAuthors

Abstract
Several authors have reported variations in the size of the proper palmar and dorsal arteries of each digit of the hand, which could affect the success of a reconstructive hand surgery, especially regarding the use of flaps. The aim of the present study is to perform a qualitative comparison of the size of these arteries in each finger. In order to do so, six hands from cryopreserved fresh cadavers were injected with latex. The fingers were prepared using the tissue-clearing technique by Spalteholz and a variation of it with glycerine.
The results show a predominance of the proper digital palmar artery in the ulnar side of the index and middle fingers, as well as in the radial side of the small finger. The only proper dorsal digital arteries that were visible were those of the thumb and of the radial side of the index finger. Despite the consistency of the pattern described, anatomic variations can occur in any digit, which force the surgeon to explore the patient through the modified Allen test and Doppler-ultrasound before any surgical intervention.
Introduction
Several authors have described variations in the caliber of the proper palmar and dorsal arteries of each digit of the hand. Since multiple flaps described in reconstructive hand surgery are based on the proper palmar digital arteries, such as the reverse-flow ipsilateral flap and the heterodigital or Littler flap, an asymmetry in the caliber of the palmar digital arteries would condition the choice of donor area and therefore the result of the surgery. The aim of the present study is to perform a qualitative comparison of the caliber of the proper palmar and dorsal digital arteries of the ulnar and radial sides of each finger.
The first study on the arterial vascularization of the fingers was carried out by Edwards in 1960,[1] based on arteriograms and a specimen prepared with nitrocellulose etching. Edwards showed that not all palmar digital arteries have the same diameter, and that these variations in size follow a fixed pattern in the thumb, index, and little fingers. The predominant artery is located on the ulnar side of the thumb and index finger, and on the radial side of the little finger. This predominant artery is larger in caliber than the artery on the opposite side of the same finger. In contrast, the arteries of the middle and ring fingers tend to have a more similar diameter and, if not, they do not follow any specific pattern. Edwards believed that this arrangement offered greater protection to the larger artery. The same author described transverse palmar connections between the palmar digital arteries of each finger, known as transverse digital arches, with consistent origins relative to the pulleys of the flexor tendons.
Later, Leslie et al.[2] compared the diameter of the digital arteries on the ulnar and radial sides of each finger at the level of the diaphysis of the proximal phalanx. The authors[2] concluded that, in general, the predominant artery is located on the ulnar side in the index and middle fingers, and on the radial side in the ring and little fingers.
In 1990, Strauch and De Moura[3] carried out an anatomical study of the arterial system of the fingers by dissecting 141 fingers from non-cryopreserved cadavers. These authors[3] concluded that, in the thumb, index and middle finger, the proper palmar digital artery on the ulnar side tends to have a larger caliber. In the ring finger and little finger, the predominant artery would be on the radial side. Consequently, they recommended prioritizing the reconstruction of the artery on the ulnar side in case of trauma to the first three fingers, the opposite being true for the ring and little fingers.
Recently, a study by Coderech Carretero et al.[4] on the caliber and flow dominance of the arteries of the hand and fingers using Doppler ultrasound has shown results similar to those previously discussed. Thus, in the first three fingers of the hand, the proper palmar digital artery on the ulnar side had a larger caliber. In contrast, the predominant artery in the ring and little fingers was located on the radial side.[4]
Other authors have focused their studies on the vascularization of the thumb, such as Earley,[5] who in 1986 showed that in 90% of the cases the proper palmar digital artery on the ulnar side of the thumb (mean diameter: 1.8 mm) has a larger caliber than that of the artery on the radial side (mean diameter: 1.1mm), thus being between 25% and 30% larger.
The transverse digital palmar arches, originally described by Edwards[1] in 1960, provide transverse communication to the proper palmar digital arteries of both sides of each finger. These branches, with consistent origins relative to the pulleys of the flexor tendons, are the proximal transverse digital, middle transverse digital, and distal transverse digital arteries ([fig. 1]). In the thumb, we find the proximal digital transverse arch at the neck of the phalanx, and the distal transverse arch, at the level of the fingertip.[1] [3]

As for the arterial vascularization of the dorsal aspect of the fingers, it depends on the proper palmar digital arteries and the proper dorsal digital arteries.
The proper palmar digital arteries give off three dorsal branches on each side of each phalanx. These branches, which have a regular distribution, are: the condylar artery, the metaphyseal artery, and the dorsal cutaneous artery ([fig.1]).[3]
The proper dorsal digital arteries also contribute to the arterial supply of the dorsal aspect of the fingers. Edwards[1] considered the proper dorsal digital arteries to be insignificant branches of the dorsal metacarpal arteries, with the exception of those of the thumb. And even in cases in which the proper dorsal digital arteries were more developed, they tended to disappear at the level of the proximal phalanx.
The results of the study carried out by Earley,[5] focused on the vasculature of the thumb, indicate that its proper dorsal digital arteries are extremely variable and small, even absent when the dorsal branches of the first palmar metacarpal artery are large. Parks et al.[6] agree with the fact that the dorsal arteries of the thumb have a small caliber, and conclude that they can have variable origins: the deep radial artery, the arteries of the first commissure, and/or the main artery of the thumb.
Materials and methods
Six cryopreserved arms, amputated proximally to the elbow joint, were arterially injected with latex. The injection principles proposed by Rees and Taylor[7] were followed.
Thus, the brachial artery was cannulated with a catheter and transverse incisions were made on the distal phalanges of all the fingers. Latex was then injected through the brachial artery by pulsatile manual pressure with a 60-mL syringe. The exit of the latex through the transverse incisions of the fingers enabled the verification that the injection was correctly performed.
Amputations were performed at the level of the metacarpophalangeal or wrist joints. In one of the specimens, several axial sections were made in each of the fingers of the hand.
Subsequently, the pieces were prepared using the tissue-clearing technique by Spalteholz,[8] as well as a modified version of the above-mentioned technique with glycerin, with the aim of showing the vascularization of the fingers without the artifacts pertaining to dissection.
In the case of the conventional Spalteholz[8] tissue-clearing technique, some of the pieces injected with black latex were progressively dehydrated by immersing them in 60% ethanol for a week and then changing them every week to concentrations 10% higher until reaching a concentration of 100%. Subsequently, the pieces were immersed twice for a week in a concentration of 100% ethanol and finally in toluene for 2 successive periods of 1 week. Finally, the pieces were placed in a mixture of three parts of methyl salicylate and two parts of benzyl benzoate. The specimens were photographed while immersed in the liquid, fully transparent.
In the case of the Spalteholz[8] technique modified with glycerin, the pieces injected with black or red latex were immersed in a mixture of 50% water and 50% glycerin for 1 day. Subsequently, at successive 24-hour intervals, the liquids were replaced by glycerin concentrations of 75%, 85%, and, finally, by pure glycerin. The transparent pieces were photographed submerged in pure glycerin.
Results
The results of the present study, which are summarized in [Table 1], show that, in most cases, the diameter of both palmar digital arteries of each finger is different. This gauge difference follows a definite pattern in the index, middle finger, and little finger.
|
Case 1 |
Case 2 |
Case 3 |
Case 4 |
Case 5 |
Case 6 |
||
|---|---|---|---|---|---|---|---|
|
Proper palmar digital arteries (predominance) |
Thumb |
Radial |
Ulnar |
Ulnar |
Radial |
No differences |
(Thumb amputation) |
|
Index finger |
Ulnar |
Ulnar |
Ulnar |
Ulnar |
Ulnar |
Ulnar |
|
|
Middle finger |
Ulnar |
Ulnar |
Ulnar |
Ulnar |
No differences |
Ulnar |
|
|
Ring finger |
Ulnar |
Radial |
Radial |
No differences |
No differences |
Radial |
|
|
Little finger |
Radial |
Radial |
Ulnar |
Radial |
Radial |
Radial |
|
|
Proper dorsal digital arteries (predominance) |
Ulnar of the thumb (or ulnar side of the thumb) |
Both arteries of the thumb and the radial artery of the index |
Ulnar of the thumb (or ulnar side of the thumb) |
Ulnar of the thumb (or ulnar side of the thumb) |
Both arteries of the thumb |
Ulnar of the thumb (or ulnar side of the thumb) |
|
|
Hand laterality/technique used |
Right hand/glycerin |
Right hand/glycerin |
Right hand/glycerin (4th-5th fingers) and conventional Spalteholz (1st-3rd fingers) |
Left hand/Spalteholz |
Right hand/Spalteholz |
Right hand/glycerin |
|
In all the specimens, the predominant artery of the index finger is located on the ulnar side ([fig. 2]). Similarly, in five of the six cases, the palmar digital artery of the middle finger is larger on the ulnar side; in the remaining case, there is no difference between both arteries. Regarding the little finger, the artery on the radial side has a larger diameter in five of the six specimens; only in one case the predominant digital artery is located on the ulnar side ([fig. 3]).


In the thumb, one third of the specimens present a predominant palmar digital artery on the ulnar side, one third, on the radial side, and, in the remaining third, no significant differences between the two arteries are observed ([fig. 4]). When the palmar digital arteries of the ring finger show a different caliber, they do not follow a certain pattern.

As for the dorsal digital arteries, the only ones visible are the two of the thumb and the one located on the radial side of the index finger. In the thumb, the dorsal digital artery on the ulnar side has a larger diameter than that of the artery on the radial side in all specimens. Comparatively, the diameter of the dorsal digital artery on the ulnar side of the thumb is greater than that of the dorsal digital artery on the radial side of the index finger.
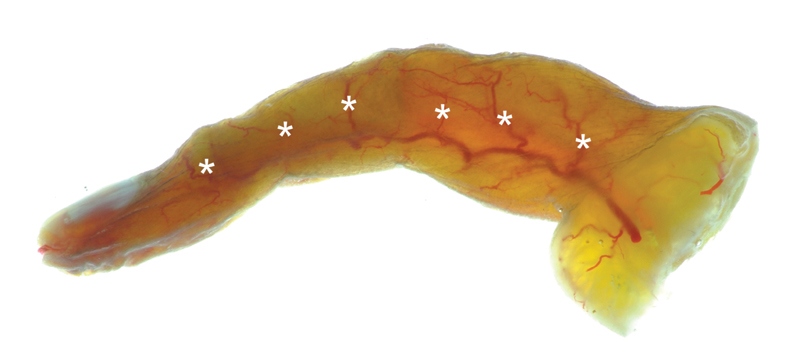
We have also consistently observed the presence of the transverse digital palmar arches and the dorsal branches of the palmar digital arteries ([fig. 5]).
Discussion
Anatomical study
Multiple studies[1] [2] [3] [5] have documented differences in the caliber of the proper palmar digital arteries of each finger. However, there are discrepancies about the specific pattern that each finger follows.
All the authors who have included triphalangeal finger vascularization in their studies[1] [2] [3] observed that the pattern followed by the index and little fingers coincide: the larger-caliber proper palmar digital artery is located on the ulnar side in the index finger and on the radial side in the little finger. The results of the present study are in accordance with these data since, in all the specimens examined, the proper palmar digital artery on the ulnar side in the index finger is greater than that of the radial side, and the proper palmar digital artery on the radial side in the little finger predominates over the artery on the ulnar side. We have observed a single exception to this described pattern, the case of a specimen that presented a predominant proper palmar digital artery on the ulnar side of the little finger. This result reinforces the importance of performing a modified Allen test prior to surgery, since the existence of a dominant arterial pattern does not exclude the possibility of an anatomical variant.
In the case of the thumb, the results of studies[1] [3] [5] in the literature show a predominance of the proper palmar digital artery on the ulnar side over the artery on the radial side. In the present study, however, we have not observed this predominance. Our results in the thumb have been heterogeneous in terms of the larger-caliber proper palmar digital artery: on the ulnar side in two cases, radial in two cases, and without differences in another case. It is possible that a study with a larger number of specimens points towards a predominance of the ulnar side.
Regarding the middle and ring fingers, there is more discrepancy in the literature. Edwards[1] concludes that there are differences between the proper palmar digital arteries on both sides of the middle and ring fingers. Similarly, Leslie et al.[2] consider that the difference in caliber of these arteries is not statistically significant, although they describe a predominance of the ulnar side in the middle finger, and of the radial side in the ring finger. On the other hand, Strauch and De Moura[3] and Coderech Carretero et al.[4] locate the vascular axis of the hand in the third commissure, with an ulnar predominance in the thumb, index finger, and middle finger, and a radial predominance in the ring and little fingers. The results of the present study are in accordance with those obtained by these authors[3] [4] in the middle finger, with a larger-caliber proper palmar digital artery on the ulnar side in all the specimens examined. On the other hand, the results in the ring finger are disparate, although a certain predominance of the radial side could be intuited: in three specimens, the artery on the radial side is larger; in one case, the predominance is located on the ulnar side; and, in the remaining two cases, no differences were observed between the two arteries. As in the case of the thumb, it is possible that by increasing the number of specimens studied, the results coincide with the pattern established by Strauch and De Moura[3] and Coderech Carretero et al.[4] to each finger.
Regarding the arterial vascularization of the dorsal aspect of the fingers, the results of the present study are similar to those obtained in previous studies.[1] [5] [6] The proper dorsal digital arteries themselves are branches that either have very small diameters or are absent, as Edwards concluded.[1] The exception to this rule would be the proper dorsal digital arteries of the thumb and on the radial side of the index finger. In the present study, these are the only visible proper dorsal digital arteries, especially those of the thumb. However, they present variability in caliber and origin, as pointed out by previous studies.[1] [5] [6]
We have also almost consistently observed the presence of arterial connections between both proper palmar digital arteries of each finger in the form of transverse digital arches, described by Edwards[1] and later studied by Strauch and De Moura,[3] as well as the regular distribution of the dorsal branches of the proper palmar digital arteries presented by these same authors.
Study limitations
It is not possible to carry out a quantitative comparative study of the diameter of the digital arteries due to the limitations inherent to the anatomical technique used to study it. Latex injection can distort, although minimally and homogeneously, the diameter of the injected vessels. In addition, there is also a variation each time the injection is performed, since there are several factors that are difficult to control objectively, such as the pressure applied by the person when injecting. In the Spalteholz[8] tissue-clearing technique, a certain degree of optical distortion can also occur when the pieces are immersed in the mixture. Finally, as these are donors whose clinical history is unknown, it is not possible to rule out the presence of factors that could alter the vascular structure of the patient in life, such as peripheral arterial disease.
Conclusions
The proper palmar digital arteries on both sides present differences in their diameter in the index, middle, and little fingers. Almost consistently, the ulnar-sided proper palmar digital artery is larger than the artery on the radial side in the index and middle fingers, and the artery on the radial side is larger than the artery on the ulnar side in the little finger. However, anatomical variations make it necessary to systematically perform a modified Allen test and Doppler ultrasound examination of the patient before reconstructive surgery of the hand, since the difference in caliber of both palmar digital arteries of each finger can condition the success of the intervention.
The proper dorsal digital arteries with the largest diameter are those of the thumb and the radial side of the index finger. The rest of the arterial vascularization of the dorsal aspect of the fingers depends on the dorsal branches of the proper palmar digital arteries, which are distributed regularly in each phalanx.
Conflicto de Intereses
Los autores no tienen conflicto de intereses que declarar.
-
Referencias
- 1 Edwards EA. Organization of the small arteries of the hand and digits. Am J Surg 1960; 99: 837-846
- 2 Leslie BM, Ruby LK, Madell SJ, Wittenstein F. Digital artery diameters: an anatomic and clinical study. J Hand Surg Am 1987; 12 (5 Pt 1): 740-743
- 3 Strauch B, de Moura W. Arterial system of the fingers. J Hand Surg Am 1990; 15 (01) 148-154
- 4 Coderech Carretero J, Corella Montoya F, Grande Barez M, Corella Montoya MÁ, Ocampos Hernández M, Larrainzar-Garijo R. Description and analysis of the dynamic and morphological flow pattern of the main arteries of the wrist and hand in a healthy spanish population. Rev Esp Cir Ortop Traumatol (Engl Ed) 2020; 64 (03) 167-176
- 5 Earley MJ. The arterial supply of the thumb, first web and index finger and its surgical application. J Hand Surg [Br] 1986; 11 (02) 163-174
- 6 Parks BJ, Arbelaez J, Horner RL. Medical and surgical importance of the arterial blood supply of the thumb. J Hand Surg Am 1978; 3 (04) 383-385
- 7 Rees MJW, Taylor GI. A simplified lead oxide cadaver injection technique. Plast Reconstr Surg 1986; 77 (01) 141-145
- 8 Spalteholz W. . Ueber das Durchsichtigmachen von Menschlichen und Tierischen Präparaten; nebst Anhang: Ueber Knochenfärburg. Leipzig: S. Hirzel; 1911
Address for correspondence
Publication History
Received: 05 April 2022
Accepted: 14 June 2022
Article published online:
16 December 2022
© 2022. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referencias
- 1 Edwards EA. Organization of the small arteries of the hand and digits. Am J Surg 1960; 99: 837-846
- 2 Leslie BM, Ruby LK, Madell SJ, Wittenstein F. Digital artery diameters: an anatomic and clinical study. J Hand Surg Am 1987; 12 (5 Pt 1): 740-743
- 3 Strauch B, de Moura W. Arterial system of the fingers. J Hand Surg Am 1990; 15 (01) 148-154
- 4 Coderech Carretero J, Corella Montoya F, Grande Barez M, Corella Montoya MÁ, Ocampos Hernández M, Larrainzar-Garijo R. Description and analysis of the dynamic and morphological flow pattern of the main arteries of the wrist and hand in a healthy spanish population. Rev Esp Cir Ortop Traumatol (Engl Ed) 2020; 64 (03) 167-176
- 5 Earley MJ. The arterial supply of the thumb, first web and index finger and its surgical application. J Hand Surg [Br] 1986; 11 (02) 163-174
- 6 Parks BJ, Arbelaez J, Horner RL. Medical and surgical importance of the arterial blood supply of the thumb. J Hand Surg Am 1978; 3 (04) 383-385
- 7 Rees MJW, Taylor GI. A simplified lead oxide cadaver injection technique. Plast Reconstr Surg 1986; 77 (01) 141-145
- 8 Spalteholz W. . Ueber das Durchsichtigmachen von Menschlichen und Tierischen Präparaten; nebst Anhang: Ueber Knochenfärburg. Leipzig: S. Hirzel; 1911




