
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1757571
Conservative Treatment of Ulnar Nerve Compression at the Elbow: A Systematic Review and Meta-Analysis
Abstract
Background The clinical results of conservative treatment options for ulnar compression at the elbow have not been clearly determined. The aim of this review was to evaluate available conservative treatment options and their effectiveness for ulnar nerve compression at the elbow.
Methods In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations, a systematic review and meta-analysis of studies was performed. Literature search was performed using Ovid MEDLINE, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL).
Results Of the 1,079 retrieved studies, 20 were eligible for analysis and included 687 cases of ulnar neuropathy at the elbow. Improvement of symptoms was reported in 54% of the cases receiving a steroid/lidocaine injection (95% confidence interval [CI], 41–67) and in 89% of the cases using a splint device (95% CI, 69–99).
Conclusions Conservative management seems to be effective. Both lidocaine/steroid injections and splint devices gave a statistically significant improvement of symptoms and are suitable options for patients who refuse an operative procedure or need a bridge to their surgery. Splinting is preferred over injections, as it shows a higher rate of improvement.
#
Introduction
Ulnar nerve compression at the elbow is the second most prevalent entrapment neuropathy of the upper limb. The ulnar nerve travels down the medial side of the elbow, through the cubital tunnel, which is the most common location for entrapment of the ulnar nerve.[1] Repeated flexion of the elbow, muscle malformation, or direct compression can be the source of ulnar nerve compression at the elbow.[2] If remained untreated, the ulnar nerve compression at the elbow can lead to chronic loss of sensibility and muscle weakness.[3]
Most patients with ulnar nerve compression at the elbow undergo an operative procedure. However, conservative treatments, including splint devices, corticosteroid injections, physical therapy, and nerve gliding movements, have been described.[1] In cases where the risk of operation is high due to patient comorbidities or when patients have to wait a long time before undergoing a procedure, conservative treatment may be a good treatment option or bridge to surgery. The purpose of this article is to evaluate available conservative treatment options for ulnar nerve compression at the elbow and to review their outcomes.
#
Methods
This review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations.[4]
Search Methods for the Identification of Studies
The search strategy was conducted in collaboration with an independent librarian in the databases MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL). The final search was performed in May 2020. In [Table 1], the detailed search methods are displayed. The columns visualize databases that have been used (MEDLINE, Embase, CENTRAL) and the rows are searches with number of hits, stated as results, and the combination of searches. There was no restriction in publication years. Two authors reviewed titles and abstracts of the identified studies, and after selection of relevant studies, the full-text articles were analyzed. Disagreements were resolved by a third reviewer. Cross-referencing took place to identify any additional studies missed in the search.
#
Selection Criteria
All randomized controlled trials, prospective or retrospective cohort study, case–control studies, or case series were eligible for inclusion. Studies were selected if they matched the following inclusion criteria: study groups consisted of a minimum of 5 patients, with a minimal age of 18 years, and patients had received a conservative (nonsurgical) treatment for symptoms of ulnar nerve compression at the elbow. All types of conservative treatment were included. Only studies with clearly described outcomes were selected, with at least a distinction between improvement and no improvement.
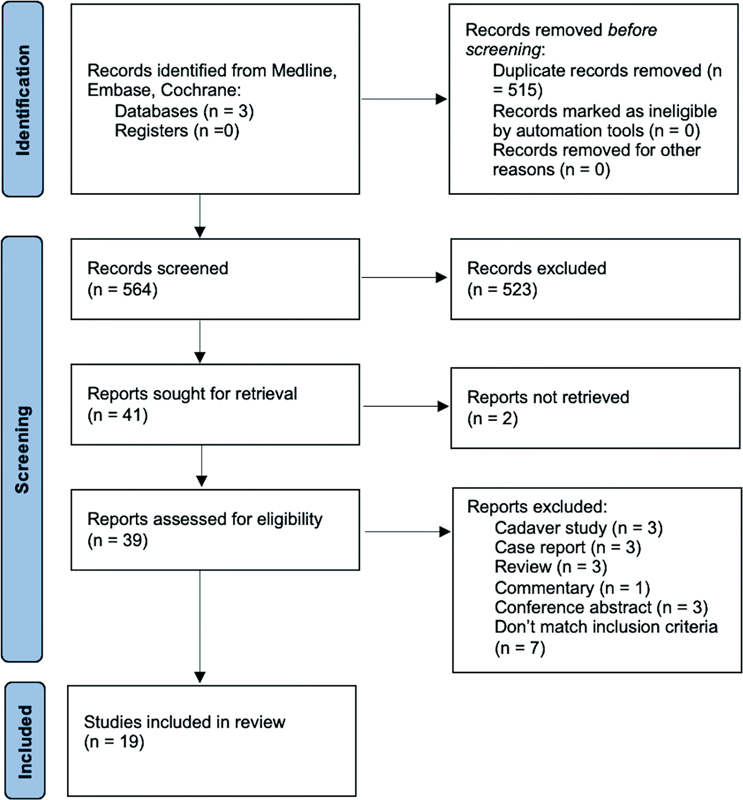
Exclusion criteria were studies performing animal experiments, cadaver studies, single case reports, or reviews. In [Fig. 1], the selection process is shown. [Table 2] provides a summary of the characteristics of the included studies.
|
# |
Authors and year |
Title |
Journal |
Country |
Type of study |
Number of patients receiving conservative treatment |
Level of evidence |
Funding or conflict of interest |
Methodological quality assessment |
|
Injections: |
|||||||||
|
1 |
Alblas et al, 2012[8] |
Injection with corticosteroids (ultrasound guided) in patients with an ulnar neuropathy at the elbow, feasibility study |
European Journal of Neurology |
The Netherlands |
Case series, prospective |
8 |
IV |
NM |
High |
|
2 |
Chen et al, 2020[20] |
Perineural dextrose and corticosteroid injections for ulnar neuropathy at the elbow: a randomized double-blind trial |
Archives of Physical Medicine & Rehabilitation |
China |
Case–control, prospective |
33 |
III |
No |
High |
|
3 |
Choi et al, 2015[9] |
Clinical implications of real-time visualized ultrasound-guided injection for the treatment of ulnar neuropathy at the elbow: a pilot study |
Annals of Rehabilitation Medicine |
Korea |
Caser series, prospective |
10 |
IV |
No |
High |
|
4 |
Gronbeck et al, 2021[10] |
Ultrasound-guided cubital tunnel injection: a review and exploration of utility as a diagnostic aid in mild or nonclassic cubital tunnel patients |
Techniques in Orthopaedics |
United States |
Case series, retrospective |
63 |
IV |
NM |
High |
|
5 |
Pechan and Kredba, 1980[11] |
Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. II. Long-term follow-up |
Acta Universitatis Carolinae, Medical |
Czech Republic |
Case series, prospective |
14 |
IV |
NM |
Moderate |
|
6 |
Rampen et al, 2011[12] |
Ultrasound-guided steroid injection to treat mild ulnar neuropathy at the elbow |
Muscle & Nerve |
The Netherlands |
Case series, prospective |
7 |
IV |
NM |
High |
|
7 |
vanVeen et al, 2015[21] |
Corticosteroid injection in patients with ulnar neuropathy at the elbow: a randomized, double-blind, placebo-controlled trial |
Muscle & Nerve |
The Netherlands |
Case–control, prospective |
30 |
III |
NM |
High |
|
Physical therapy: |
|||||||||
|
8 |
Oskay et al, 2010[13] |
Neurodynamic mobilization in the conservative treatment of cubital tunnel syndrome: long-term follow-up of 7 cases |
Journal of Manipulative & Physiological Therapeutics |
Turkey |
Case series, prospective |
7 |
IV |
No |
Moderate |
|
9 |
Ozkan et al, 2015[22] |
New treatment alternatives in the ulnar neuropathy at the elbow: ultrasound and low-level laser therapy |
Acta Neurologica Belgica |
Turkey |
Case–control, prospective |
32 |
III |
No |
High |
|
Splint devices: |
|||||||||
|
10 |
Dellon et al, 1993[14] |
Nonoperative management of cubital tunnel syndrome: an 8-year prospective study |
Neurology |
United States |
Case series, prospective |
121 |
IV |
NM |
High |
|
11 |
Hong et al, 1996[23] |
Splinting and local steroid injection for the treatment of ulnar neuropathy at the elbow: clinical and electrophysiological evaluation |
Archives of Physical Medicine & Rehabilitation |
United States |
Case–control, prospective |
10 |
III |
No |
High |
|
12 |
Michell and Sesath, 2020[15] |
Feasibility trial of treatment of ulnar neuropathy at the elbow using a specifically designed splint |
JCR: Journal of Clinical Rheumatology |
United Kingdom |
Case series, prospective |
15 |
IV |
NM |
Moderate |
|
13 |
Seror, 1993[16] |
Treatment of ulnar nerve palsy at the elbow with a night splint |
Journal of Bone & Joint Surgery |
France |
Case series, prospective |
22 |
IV |
NM |
High |
|
14 |
Shah et al, 2013[17] |
Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome |
Journal of Hand Surgery |
United States |
Case series, prospective |
19 |
IV |
NM |
High |
|
15 |
Svernlöv et al, 2009[24] |
Conservative treatment of the cubital tunnel syndrome |
Journal of Hand Surgery |
Sweden |
Case–control, prospective |
51 |
III |
NM |
High |
|
Other: |
|||||||||
|
16 |
Beekman et al, 2004[25] |
Ulnar neuropathy at the elbow: follow-up and prognostic factors determining outcome |
Neurology |
Netherlands |
Case– control, prospective |
NA |
III |
NM |
High |
|
17 |
Nakamichi et al, 2009[18] |
Patient education for the treatment of ulnar neuropathy at the elbow |
Archives of Physical Medicine & Rehabilitation |
Japan |
Case series, prospective |
77 |
IV |
No |
High |
|
18 |
Omejec and Podnar, 2018[26] |
Long-term outcomes in patients with ulnar neuropathy at the elbow treated according to the presumed etiology |
Clinical Neurophysiology |
Slovenia |
Case– control, prospective |
67 |
III |
Yes |
High |
|
19 |
Padua et al, 2002[19] |
Natural history of ulnar entrapment at elbow |
Clinical Neurophysiology |
Italy |
Case series, retrospective |
30 |
IV |
NM |
High |
Abbreviations: NA, no information available; NM, not mentioned.
#
Quality Assessment
The quality of the included case–control studies was assessed using the “JBI Critical Appraisal Checklist for case-control studies” and the “JBI Critical Appraisal checklist for case series.”[5] These checklists pay attention to selection of the study groups, evaluation of the exposure, and statistical analysis. In the checklist for case–control studies, the comparability of the groups and confounding factors are evaluated. Quality assessment is performed using a score ranging from 0 to 10 points. Studies with a score of 7 to 10 points were considered as high quality, 4 to 6 points as moderate quality, and 0 to 3 as low quality. Two reviewers conducted the quality appraisal. Any disagreements during the process were discussed and resolved by adjudication by a third reviewer.
#
Data Extraction
Data were independently extracted by two reviewers. The following data were extracted from the studies: total number of patients, gender, affected arm (dominant/nondominant), duration of symptoms until the start of treatment, type of conservative treatment, total duration of treatment, subjective and objective outcome measurements for pain, sensory or motor function improvement after the conservative treatment, advantages and disadvantages described by the authors, complications, and other features. In cases of different interpretations, the results were discussed again by the two reviewers and resolved by involvement of a third reviewer.
#
Statistical Analysis
The I2 statistic was determined to measure study heterogeneity. The cutoff value for low, moderate, and high heterogeneity is set at 25, 50, and 75%, respectively.[6] When possible and appropriate, a random-effects model was used to pool proportions of individual studies in the subgroups. This was done for the subgroup injections and splint devices, with the exception of studies reporting no individual response rates. Because I2 was moderate to high in both subgroups, random-effects models were used for further analyses. Results are presented as mean values or 95% confidence intervals. A p-value of ≤0.05 was considered statistically significant. Forest and funnel plots for both subgroup analyses were created for optimal visualization of the results. No additional analyses were done. Statistical analyses were performed using MedCalc for Windows, version 19.3.1 (MedCalc Software, Ostend, Belgium).[7]
#
#
Results
Initially, 1,079 studies were identified. A total of 515 duplicates were removed, and the remaining 564 titles and abstracts were screened for suitability. Forty-one studies were selected and the full texts were read. Nineteen papers were included in the final analysis. Screening the reference lists did not provide inclusion of additional studies. The selection process flow diagram with reasons for exclusion is shown in [Fig. 1]. Of the included studies, 12 were level IV evidence,[8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] whereas 7 were level III[20] [21] [22] [23] [24] [25] [26] ([Table 2]). Methodological quality varied among the studies: 16 studies were considered as high quality and 3 studies as moderate quality. Also, 63% (n = 12) of the studies did not mention if they were funded, while 32% (n = 6) of the studies explicitly stated no funding. One study reported funding, but declared this had no role in collection, analysis, and interpretation of data and in writing of the manuscript.[26] A total of 682 patients, including 684 arms, were followed-up after receiving a treatment for ulnar nerve compression at the elbow. One study included a patient group receiving surgical management, without stating the exact number of patients involved.[25] In studies describing the following parameters, patients had a mean age of 48.7 years, the dominant side was involved in 64% of patients (198 of 313), and the minimal follow-up period was an average of 6.2 months (range: 1–124 months). Six studies included patients with mild-to-moderate symptoms,[10] [12] [15] [17] [20] [24] while 13 studies included patients with any severity of symptoms.[8] [9] [11] [13] [14] [16] [18] [19] [21] [22] [23] [25] [26] The most common interventions, from most to least common, included education and activity modification, steroid/lidocaine injection, splinting, physical therapy, pulsed ultrasound (US), or laser therapy. The most commonly reported outcomes included subjective clinical and patient-reported outcomes, such as patient-reported VAS scores, symptoms, questionnaires, and clinical signs, followed by nerve conduction studies and US examination. Two studies only reported subjective outcomes,[10] [15] while 17 studies reported on a combination of subjective and objective outcome measurements.[8] [9] [11] [12] [13] [14] [16] [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] Subgroup meta-analyses were performed on the injection and the splint devices studies. Oskay et al reported that 100% of patients (n = 7) had improvement of symptoms after physical therapy with an average follow-up period of 12 months, specifically after neurodynamic mobilization therapy in combination with US therapy.[13] Ozkan et al stated that 69% of the patients (n = 32) had improvement of symptoms 3 months after starting US or low-level laser therapy (LLLT).[22] The duration of symptoms was between 5 weeks and 6 months at the start of these physical therapies. Nakamichi et al stated that 59% of arms (n = 80) had improvement of symptoms 3 months after education about the pathophysiology and activity modification.[18] Beekman et al and Omejec et al reported that, respectively, 35 and 82% of the arms (n = 46 and 67) had improvement of symptoms after an average period of 22,8 months after starting to avoid risky positioning of the affected limb, and Padua et al described that 40% of the arms (n = 30) had improvement of their symptoms after 6 to 19 months of only giving information about what ulnar nerve entrapment at the elbow is and how to avoid risky positioning.[19] [25] [26] Beekman et al reported an average duration of symptoms of 3.5 months before the start of activity modification.[25] Omejec et al and Padua et al did not mention the duration of symptoms.[19] [26] Study data are presented in [Table 3].
|
# |
Authors and year |
No. of patients in conservative group/no. of cases |
Males (no. [%])/females (no. [%]) |
Mean age in years (range) |
Severity of the included cases[a] |
Mean FU in years (range) |
No. of cases improved (%)/no. of patients not improved (%) |
|---|---|---|---|---|---|---|---|
|
Injections |
|||||||
|
1 |
Alblas et al, 2012[8] |
8/9 |
4 (50)/4 (50) |
53 (43–67) |
U |
0.25 (NA) |
5 (56)/4 (44) |
|
2 |
Chen et al, 2020[20] |
33/33 |
11 (33)/22 (67) |
56 (32–77) |
Mild-to-moderate |
0.5 (NA) |
17 (52)/16 (48) |
|
3 |
Choi et al, 2015[9] |
10/10 |
7 (70)/3 (30) |
63 (57–58) |
U |
0.1 (NA) |
NA (significant drop in VAS) |
|
4 |
Gronbeck et al, 2021[10] |
NA/56 |
NA |
47 (NA) |
Mild |
NA (0.1–0.25) |
38 (68)/18 (32) |
|
5 |
Pechan and Kredba, 1980[11] |
14/22 |
6 (43)/8 (57) |
41 (25–65) |
Mild |
1.2 (0.5–NA) |
14 (64)/8 (36) |
|
6 |
Rampen et al, 2011[12] |
7/7 |
6 (86)/1 (14) |
43 (32–54) |
Mild |
0.13 (NA) |
4 (57)/3 (43) |
|
7 |
vanVeen et al, 2015[21] |
30/30 |
18 (60)/12 (40) |
56 (29–91) |
U |
0.25 (NA) |
9 (30)/21 (70) |
|
Physical therapy: |
|||||||
|
8 |
Oskay et al, 2010[13] |
7/7 |
NA |
NA (35–70) |
U |
1.0 (NA) |
7 (100)/0 (0) |
|
9 |
Ozkan et al, 2015[22] |
32/32 |
16 (50)/16 (50) |
44 (NA) |
U |
0.25 (NA) |
22 (69)/10 (31) |
|
Splint devices: |
|||||||
|
10 |
Dellon et al, 1993[14] |
121/121 |
23 (19)/98 (81) |
44 (15–72) |
U |
4.9 (1.0–10.3) |
85 (70)/36 (30) |
|
11 |
Hong et al, 1996[23] |
10/12 |
10 (100)/0 (0) |
59 (37–70) |
U |
0.5 (NA) |
NA (significant improvement in symptoms) |
|
12 |
Michell and Sesath, 2020[15] |
15/15 |
4 (27)/11 (73) |
41 (21–84) |
Mild-to-moderate |
0.15 (0.13–0.4) |
11 (73)/4 (27) |
|
13 |
Seror, 1993[16] |
22/22 |
12 (55)/10 (45) |
52 (39–81) |
U |
0.9 (0.3–2.5) |
22 (100)/0 (0) |
|
14 |
Shah et al, 2013[17] |
19/24 |
8 (42)/11 (58) |
43 (21–72) |
Mild-to-moderate |
2.0 (1.3–2.7) |
21 (88)/3 (12) |
|
15 |
Svernlöv et al, 2009[24] |
51/51 |
24 (47)/27 (53) |
43 (17–72) |
Mild-to-moderate |
0.5 (NA) |
51 (100)/0 (0) |
|
Other: |
|||||||
|
16 |
Beekman et al, 2004[25] |
NA/46 |
NA |
51 (39–60) |
U |
1.2 (6–NA) |
16 (35)/30 (65) |
|
17 |
Nakamichi et al, 2009[18] |
77/80 |
56 (73)/21 (27) |
52 (19–77) |
U |
NA (3–NA) |
59 (74)/21 (26) |
|
18 |
Omejec and Podnar, 2018[26] |
67/67 |
33 (49)/34 (51) |
47 (19–75) |
U |
2.4 (2.2–3.4) |
55 (82)/12 (18) |
|
19 |
Padua et al, 2002[19] |
27/30 |
11 (41)/16 (59) |
57 (32–76) |
U |
NA (0.5–1.6) |
12 (40)/18 (60) |
Abbreviations: FU, follow-up; NA, no information available; U, unspecified; VAS, visual analog scale.
a The severity of the included cases was defined by the authors of the included studies.
Physical Therapy, Ultrasound, and Laser Therapy
Neurodynamic mobilization in combination with US therapy was reported to be a beneficial therapy for all patients. Oskay et al stated that these therapies are viable options for the treatment of ulnar neuropathy at the elbow.[13] Ozkan et al saw significant improvement in patients after treating them with either US or LLLT.[22] More severely affected patients were pooled in the US group, so they reason that this therapy might be superior to LLLT.
#
Meta-analysis
Injections
In our meta-analysis of the outcomes of conservative therapy for ulnar nerve compression at the elbow, a statistically significant proportion of patients improved after a steroid/lidocaine injection.
Pooled results of six studies in the injections subgroup showed that 54% of the patients (95% confidence interval [CI], 41–67) improved after an average period of 4.3 months after receiving a steroid/lidocaine injection for ulnar nerve compression at the elbow. The duration of symptoms before injection was 2 to 36 months. The I2 was 59% (95% CI, 0–83). Forest and funnel plot are shown in [Fig. 2], and detailed calculations are shown in [Table 4].

|
Author and year |
Sample size (no. of cases) |
Proportion (%) |
95% CI |
Weight (%) random effects |
|---|---|---|---|---|
|
[Fig. 2]: pooled results of overall symptomatic improvement in proportions of improved patients in the injections subgroup |
||||
|
Alblas et al, 2012[8] |
9 |
55,556 |
21,201–86,300 |
11.02 |
|
Chen et al, 2020[20] |
33 |
51,515 |
33,544–69,204 |
19.93 |
|
Gronbeck et al, 2021[10] |
56 |
67,857 |
54,036–79,715 |
23.07 |
|
Pechan and Kredba, 1980[11] |
22 |
63,636 |
40,658–82,802 |
17.17 |
|
Rampen et al, 2011[12] |
7 |
57,143 |
18,405–90,101 |
9.51 |
|
vanVeen et al, 2015[21] |
30 |
30,000 |
14,735–49,396 |
19.30 |
|
Total (random effects) |
157 |
54,009 |
41,135–66,617 |
100.00 |
|
[Fig. 3]: pooled results of overall symptomatic improvement in proportions of improved patients in the splint devices subgroup |
||||
|
Dellon et al, 1993[14] |
121 |
70,248 |
61,262–78,215 |
21.77 |
|
Michell and Sesath, 2020[15] |
15 |
73,333 |
44,900–92,213 |
18.30 |
|
Seror, 1993[16] |
22 |
100,000 |
84,563–100,000 |
19.38 |
|
Shah et al, 2013[17] |
24 |
87,500 |
67,639–97,344 |
19.59 |
|
Svernlöv et al, 2009[24] |
51 |
100,000 |
93,022–100,000 |
20.96 |
|
Total (random effects) |
235 |
89,000 |
69,729–99,128 |
100 |

#
Splinting
Pooled results of five studies in the splint devices subgroup showed that 89% of the patients (95% CI, 69–99) improved using a splint device for ulnar nerve compression at the elbow for an average period of 18.7 months.[14] I2 was 92% (95% CI, 84–96). Forest and funnel plot are shown in [Fig. 3], and detailed calculations are shown in [Table 4]. The duration of symptoms before starting the usage of a splint was 0.5 to 72 months. All studies used an elbow brace that prevented elbow flexion. Dellon et al, Seror, Shah et al, and Svernlöv et al used a nighttime splint,[14] [16] [17] [24] while Hong et al and Michell and Sesath recommended to wear the splints as much as possible.[15] [23] The splints consisted of a variety of materials, including neoprene, polyform, and thermoplastic.[14] [23] [24] Michell and Sesath designed the Cambridge Ulnar Splint, with a plastic exoskeleton, for their study.[15]
#
#
#
Discussion
In this systematic review, we evaluated available conservative treatment options for ulnar nerve compression at the elbow and reviewed the effectiveness and complications of the options. Of the 1,079 retrieved studies, 19 were eligible for analysis and included a total of 682 patients and 684 cases of ulnar neuropathy at the elbow. Improvement of symptoms was reported in 54% of the cases receiving a steroid/lidocaine injection (95% CI, 41–67). Improvement of symptoms was reported in 89% of the cases using a splint device (95% CI, 69–99).
The results of the subgroup meta-analyses show the proportions of patients with improvement of symptoms, but not how much they improved. The inability to determine the amount of the improvement is due to the wide variety of outcome measures used in the included studies (e.g., subjective clinical and patient-reported outcomes, nerve conduction studies, and US examination).
All the studies included in this systematic review described improvement in symptoms after education, information about avoiding risky positioning of the elbow, or both. Nakamichi et al described this treatment to be effective, inexpensive, and simple, with no contraindications. It can be started immediately after diagnosis.[18] Since there were no control groups in any of these studies, where patients received no information at all, improvement due to the natural course of ulnar neuropathy at the elbow cannot be ruled out.
In our meta-analysis, a statistically significant proportion of patients using a splint device for ulnar nerve compression at the elbow improved. Michell and Sesath presented it to be a comfortable, effective, and cost-effective treatment option.[15] Seror and Svernlöv et al report that even patients with severe and long-lasting symptoms benefited from wearing a splint.[16] [24] Hong et al compared wearing a splint with an additional steroid injection and detected no supplementary effect of the injection.[23] This brings us to a curious point where it is the question if the placebo effect or natural course of ulnar nerve compression at the elbow might not be inadequate.
A major flaw of the study is the lack of preoperative clinical data. The severity of the clinical situation is not exactly known. Six studies only included patients with mild-to-moderate symptoms, while 13 studies included patients with any severity of symptoms. However, it is possible that patients with more severe symptoms were offered or opted for surgery earlier. Different patient populations are compared, and different treatment durations, follow-up periods, compliances, and outcome measures are reported in the included studies. Duration of symptoms in the included studies is not clearly stated, so no conclusion could be drawn on the natural course of ulnar neuropathy at the elbow.
It cannot be denied that bias might be introduced especially due to the lack of a proper control group and small samples. Dropouts in the included studies are likely to be patients who are experiencing no effect from conservative treatment options, so effectiveness of the investigated treatment could be overrated in some of the included studies. This might be overcome by developing a proper randomized clinical trial comparing some kind of conservative treatment with no treatment.
Conservative management for ulnar neuropathy at the elbow seems to improve symptoms in up to 9 out of 10 patients. Both lidocaine/steroid injections and splint devices gave a significant improvement in symptoms and are suitable options for patients who refuse an operative procedure or need a bridge to this treatment. Physical therapy also seems to be a promising option but needs to be investigated further in larger samples to draw any conclusions on the overall effectiveness. Also, the education and activity modification gave a positive effect on the symptoms and form a simple way to start any treatment for ulnar neuropathy at the elbow. In cases where surgical treatment is not applicable to patients due to comorbidities, it is tempting to advise education in combination with activity modification. This might be followed or combined with further splinting. However, the limitations of this study should be taken into consideration.
#
#
Conflict of Interest
None declared.
Acknowledgments
We thank Alice Tillema for her assistance with database searches.
Note
The authors received no financial support for the research, authorship, and/or publication of this article.
Authors' Contributions
T.N.: conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft, writing – review and editing.
M.S.v.d.W.: Conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft, writing – review and editing.
E.P.H.: Conceptualization, methodology, writing – original draft, writing – review and editing.
N.J.S.: Data curation, formal analysis, investigation, methodology, writing – original draft.
E.T.W.: Conceptualization, project administration, supervision, writing – review and editing.
R.H.M.A.B.: Conceptualization, investigation, methodology, project administration, resources, supervision, writing – review and editing.
-
References
- 1 Caliandro P, La Torre G, Padua R, Giannini F, Padua L. Treatment for ulnar neuropathy at the elbow. Cochrane Database Syst Rev 2016; 11: CD006839
- 2 Jacobson L, Dengler J, Moore AM. Nerve entrapments. Clin Plast Surg 2020; 47 (02) 267-278
- 3 Boone S, Gelberman RH, Calfee RP. The management of cubital tunnel syndrome. J Hand Surg Am 2015; 40 (09) 1897-1904 , quiz 1904
- 4 Page MJ, McKenzie JE, Bossuyt PM. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372 (71) n71
- 5 Moola S, Munn Z, Tufanaru C. , et al. , Systematic reviews of etiology and risk. In: Aromataris E, Munn Z. eds. Joanna Briggs Institute Reviewer's Manual. The Joanna Briggs Institute; 2017
- 6 Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327 (7414): 557-560
- 7 Ostend, Belgium: MedCalc Software Ltd; 2020
- 8 Alblas CL, van Kasteel V, Jellema K. Injection with corticosteroids (ultrasound guided) in patients with an ulnar neuropathy at the elbow, feasibility study. Eur J Neurol 2012; 19 (12) 1582-1584
- 9 Choi CK, Lee HS, Kwon JY, Lee WJ. Clinical implications of real-time visualized ultrasound-guided injection for the treatment of ulnar neuropathy at the elbow: a pilot study. Ann Rehabil Med 2015; 39 (02) 176-182
- 10 Gronbeck C, Wolf J, Rodner CM. Ultrasound-guided cubital tunnel injection: a review and exploration of utility as a diagnostic aid in mild or nonclassic cubital tunnel patients. Tech Orthop 2021; 36 (03) 301-306
- 11 Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. II. Long-term follow-up. Acta Univ Carol [Med] (Praha) 1980; 26 (3–4): 135-140
- 12 Rampen AJ, Wirtz PW, Tavy DL. Ultrasound-guided steroid injection to treat mild ulnar neuropathy at the elbow. Muscle Nerve 2011; 44 (01) 128-130
- 13 Oskay D, Meriç A, Kirdi N, Firat T, Ayhan C, Leblebicioğlu G. Neurodynamic mobilization in the conservative treatment of cubital tunnel syndrome: long-term follow-up of 7 cases. J Manipulative Physiol Ther 2010; 33 (02) 156-163
- 14 Dellon AL, Hament W, Gittelshon A. Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology 1993; 43 (09) 1673-1677
- 15 Michell AW, Sesath HGR. Feasibility trial of treatment of ulnar neuropathy at the elbow using a specifically designed splint. J Clin Rheumatol 2020; 26 (01) 37-39
- 16 Seror P. Treatment of ulnar nerve palsy at the elbow with a night splint. J Bone Joint Surg Br 1993; 75 (02) 322-327
- 17 Shah CM, Calfee RP, Gelberman RH, Goldfarb CA. Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome. J Hand Surg Am 2013; 38 (06) 1125-1130.e1
- 18 Nakamichi K, Tachibana S, Ida M, Yamamoto S. Patient education for the treatment of ulnar neuropathy at the elbow. Arch Phys Med Rehabil 2009; 90 (11) 1839-1845
- 19 Padua L, Aprile I, Caliandro P, Foschini M, Mazza S, Tonali P. Natural history of ulnar entrapment at elbow. Clin Neurophysiol 2002; 113 (12) 1980-1984
- 20 Chen LC, Ho TY, Shen YP. et al. Perineural dextrose and corticosteroid injections for ulnar neuropathy at the elbow: a randomized double-blind trial. Arch Phys Med Rehabil 2020; 101 (08) 1296-1303
- 21 vanVeen KE, Alblas KC, Alons IM. et al. Corticosteroid injection in patients with ulnar neuropathy at the elbow: a randomized, double-blind, placebo-controlled trial. Muscle Nerve 2015; 52 (03) 380-385
- 22 Ozkan FU, Saygı EK, Senol S. et al. New treatment alternatives in the ulnar neuropathy at the elbow: ultrasound and low-level laser therapy. Acta Neurol Belg 2015; 115 (03) 355-360
- 23 Hong CZ, Long HA, Kanakamedala RV, Chang YM, Yates L. Splinting and local steroid injection for the treatment of ulnar neuropathy at the elbow: clinical and electrophysiological evaluation. Arch Phys Med Rehabil 1996; 77 (06) 573-577
- 24 Svernlöv B, Larsson M, Rehn K, Adolfsson L. Conservative treatment of the cubital tunnel syndrome. J Hand Surg Eur Vol 2009; 34 (02) 201-207
- 25 Beekman R, Wokke JH, Schoemaker MC, Lee ML, Visser LH. Ulnar neuropathy at the elbow: follow-up and prognostic factors determining outcome. Neurology 2004; 63 (09) 1675-1680
- 26 Omejec G, Podnar S. Long-term outcomes in patients with ulnar neuropathy at the elbow treated according to the presumed aetiology. Clin Neurophysiol 2018; 129 (08) 1763-1769
Address for correspondence
Publikationsverlauf
Eingereicht: 27. Januar 2022
Angenommen: 26. Mai 2022
Artikel online veröffentlicht:
06. Februar 2023
© 2023. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Caliandro P, La Torre G, Padua R, Giannini F, Padua L. Treatment for ulnar neuropathy at the elbow. Cochrane Database Syst Rev 2016; 11: CD006839
- 2 Jacobson L, Dengler J, Moore AM. Nerve entrapments. Clin Plast Surg 2020; 47 (02) 267-278
- 3 Boone S, Gelberman RH, Calfee RP. The management of cubital tunnel syndrome. J Hand Surg Am 2015; 40 (09) 1897-1904 , quiz 1904
- 4 Page MJ, McKenzie JE, Bossuyt PM. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372 (71) n71
- 5 Moola S, Munn Z, Tufanaru C. , et al. , Systematic reviews of etiology and risk. In: Aromataris E, Munn Z. eds. Joanna Briggs Institute Reviewer's Manual. The Joanna Briggs Institute; 2017
- 6 Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327 (7414): 557-560
- 7 Ostend, Belgium: MedCalc Software Ltd; 2020
- 8 Alblas CL, van Kasteel V, Jellema K. Injection with corticosteroids (ultrasound guided) in patients with an ulnar neuropathy at the elbow, feasibility study. Eur J Neurol 2012; 19 (12) 1582-1584
- 9 Choi CK, Lee HS, Kwon JY, Lee WJ. Clinical implications of real-time visualized ultrasound-guided injection for the treatment of ulnar neuropathy at the elbow: a pilot study. Ann Rehabil Med 2015; 39 (02) 176-182
- 10 Gronbeck C, Wolf J, Rodner CM. Ultrasound-guided cubital tunnel injection: a review and exploration of utility as a diagnostic aid in mild or nonclassic cubital tunnel patients. Tech Orthop 2021; 36 (03) 301-306
- 11 Pechan J, Kredba J. Treatment of cubital tunnel syndrome by means of local administration of cortisonoids. II. Long-term follow-up. Acta Univ Carol [Med] (Praha) 1980; 26 (3–4): 135-140
- 12 Rampen AJ, Wirtz PW, Tavy DL. Ultrasound-guided steroid injection to treat mild ulnar neuropathy at the elbow. Muscle Nerve 2011; 44 (01) 128-130
- 13 Oskay D, Meriç A, Kirdi N, Firat T, Ayhan C, Leblebicioğlu G. Neurodynamic mobilization in the conservative treatment of cubital tunnel syndrome: long-term follow-up of 7 cases. J Manipulative Physiol Ther 2010; 33 (02) 156-163
- 14 Dellon AL, Hament W, Gittelshon A. Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology 1993; 43 (09) 1673-1677
- 15 Michell AW, Sesath HGR. Feasibility trial of treatment of ulnar neuropathy at the elbow using a specifically designed splint. J Clin Rheumatol 2020; 26 (01) 37-39
- 16 Seror P. Treatment of ulnar nerve palsy at the elbow with a night splint. J Bone Joint Surg Br 1993; 75 (02) 322-327
- 17 Shah CM, Calfee RP, Gelberman RH, Goldfarb CA. Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome. J Hand Surg Am 2013; 38 (06) 1125-1130.e1
- 18 Nakamichi K, Tachibana S, Ida M, Yamamoto S. Patient education for the treatment of ulnar neuropathy at the elbow. Arch Phys Med Rehabil 2009; 90 (11) 1839-1845
- 19 Padua L, Aprile I, Caliandro P, Foschini M, Mazza S, Tonali P. Natural history of ulnar entrapment at elbow. Clin Neurophysiol 2002; 113 (12) 1980-1984
- 20 Chen LC, Ho TY, Shen YP. et al. Perineural dextrose and corticosteroid injections for ulnar neuropathy at the elbow: a randomized double-blind trial. Arch Phys Med Rehabil 2020; 101 (08) 1296-1303
- 21 vanVeen KE, Alblas KC, Alons IM. et al. Corticosteroid injection in patients with ulnar neuropathy at the elbow: a randomized, double-blind, placebo-controlled trial. Muscle Nerve 2015; 52 (03) 380-385
- 22 Ozkan FU, Saygı EK, Senol S. et al. New treatment alternatives in the ulnar neuropathy at the elbow: ultrasound and low-level laser therapy. Acta Neurol Belg 2015; 115 (03) 355-360
- 23 Hong CZ, Long HA, Kanakamedala RV, Chang YM, Yates L. Splinting and local steroid injection for the treatment of ulnar neuropathy at the elbow: clinical and electrophysiological evaluation. Arch Phys Med Rehabil 1996; 77 (06) 573-577
- 24 Svernlöv B, Larsson M, Rehn K, Adolfsson L. Conservative treatment of the cubital tunnel syndrome. J Hand Surg Eur Vol 2009; 34 (02) 201-207
- 25 Beekman R, Wokke JH, Schoemaker MC, Lee ML, Visser LH. Ulnar neuropathy at the elbow: follow-up and prognostic factors determining outcome. Neurology 2004; 63 (09) 1675-1680
- 26 Omejec G, Podnar S. Long-term outcomes in patients with ulnar neuropathy at the elbow treated according to the presumed aetiology. Clin Neurophysiol 2018; 129 (08) 1763-1769