

Subscribe to RSS
DOI: 10.1055/s-0042-1759785
Experience with Generic Pegylated L-asparaginase in Children with Acute Lymphoblastic Leukemia from a Tertiary Care Oncology Center in South India
Authors
Funding This project was funded by Emcure India Pvt. Ltd.

Abstract

Background Acute lymphoblastic leukemia (ALL) is a common type of leukemia in children. The innovator pegylated L-asparaginase has several advantages over native L-asparaginase; however, its use in India is limited due to availability and cost. Therefore, a generic pegylated L-asparaginase can be considered as an alternative to the innovator molecule.
Methods A retrospective study was conducted to assess the outcome (minimal residual disease [MRD]) and toxicity of a generic pegylated L-asparaginase (Hamsyl) at the end of induction therapy.
Results Eighty-eight (80.7%) and 21 (19.3%) patients had received generic pegylated L-asparaginase and conventional asparaginase, respectively, as a part of their treatment protocol. Nearly 82% of patients had B-type ALL. Eight-one percent of children had a white blood cell count of fewer than 50,000/mm3. At the end of induction, 80.7% (88) of children were minimal residual disease (MRD)-negative, and at the end of augmented consolidation therapy, 20.2% were MRD-negative. Ten percent of patients exhibited allergic reactions. Two children had pancreatitis, and one child had central venous thrombosis.
Conclusion The generic pegylated L-asparaginase (Hamsyl) was effective and safe for use in pediatric ALL.
Keywords
acute lymphoblastic leukemia - L-asparaginase - generic pegylated L-asparaginase - pegaspargase - Hamsyl - hypersensitivity - minimal residual disease - MRD - ALLIntroduction
In India, ∼40 to 50% of the burden of childhood cancer is leukemia, and acute lymphoblastic leukemia (ALL) is the most familiar type.[1] Nearly 25% of all cancers diagnosed under 15 years of age and 77% of childhood leukemia is ALL.[2] According to the data from 24 population-based cancer registries (2012–2014), the upper range in the incidence of age-adjusted childhood leukemia was 101.4 per million and 62.3 per million in boys and girls, respectively.[3] [4] Medical advances in the treatment have led to an overall 5-year survival rate of ∼90%.[1] [5] There is a lack of longitudinal data on the cancer survival rates in children in India. However, a recent review has pegged the overall survival at 45 to 81% and event-free survival at 41 to 70% in children with ALL.[1] [4] Besides a lower survival rate, developing countries such as India continue to face difficulties in achieving quality care.
L-Asparaginase is an essential component of remission induction therapy. Kidd, in 1953, discovered that guinea pig serum could regress lymphosarcoma xenografts implanted in mice.[6] Later, Broome found that asparaginase was responsible for anti-lymphoma activity.[7]
The survival of leukemia/lymphoma cells depends on the serum asparagine because the expression of L-asparagine synthetase is low in cancer cells.[8] Thus, the role of L-asparaginase in ALL is related to its ability to induce apoptosis of leukemic cells by depleting L-asparagine, which is critical for synthesizing cancer cell nuclear materials and proteins. Asparaginase aids in the hydrolysis of L-asparagine into aspartic acid and ammonia.[9]
Several L-asparaginase preparations available in the market are derived from either Escherichia coli (native and pegylated form) or Erwinia chrysanthemi.[10] [11] [12] Over the past decade, pegylated E. coli asparaginase has gained importance due to its longer half-life, better tolerability, sustained asparagine depletion, and better central nervous system protection.[13] [14] Pegylated L-asparaginase is formed by the covalent linking of polyethylene glycol to E. coli L-asparaginase.[15]
Oncaspar (pegaspargase), an innovator preparation available in the USA and Europe, is costly, and patients from middle-to-low–income group might not be able to afford it. Moreover, it is also difficult to import the drug, so its use in India is limited. Considering this unmet need in India for pegasparaginase, the Drug Controller General of India (DCGI), in 2014, approved a generic preparation of pegasparaginase under the brand name of Hamsyl (Emcure Pharmaceuticals).[16] Generic pegylated L-asparaginase(Hamsyl) could be used as a safe and cost-effective alternative to Oncaspar (pegaspargase) in India for children with ALL. The cost of the treatment could be further reduced by adopting an indigenous strategy of sharing the drug among three-fourth of children and maintaining the cold chain of the drug during long-term storage without compromising the efficacy of the drug.[14]
We report the clinical profile of generic pegylated L-asparaginase in terms of outcomes, side-effects, tolerance, and cost implications in children with ALL.
Materials and Methods
This study was a retrospective (descriptive) study in children with ALL who had received generic pegylated L-asparaginase (Hamsyl; Emcure Pharmaceuticals) or conventional asparaginase as induction/augmented consolidation/delayed intensification therapy at a Pediatric Hemato-Oncology center in South India. Oncaspar (pegaspargase), an innovator preparation available in the USA and Europe, is costly, and patients from middle-to-low–income group might not be able to afford it. Moreover, it is also difficult to import the drug, so its use in India is limited. Considering this unmet need in India for pegasparaginase, the Drug Controller General of India (DCGI), in 2014, approved a generic preparation of pegasparaginase under the brand name of Hamsyl (Emcure Pharmaceuticals). We assessed the outcome (minimal residual disease [MRD]) at the end of induction and toxicity of Hamsyl.
We reviewed medical records from January 2015 to December 2020 of children aged 18 years and below, with a diagnosis and treatment for ALL and B/T lymphoblastic lymphoma.
We retrieved data of children treated with L-asparaginase (conventional and generic pegylated-L-asparaginase [Hamsyl]) from medical records after obtaining due permission. We included all children treated with generic pegylated-L-asparaginase for ALL (upfront/relapsed) and T-or B-lymphoblastic lymphoma at our center.
Children were treated with uniform Indian Childhood Collaborative Leukemia Protocol (ICiCle) as per risk stratification based on age at presentation, total leucocyte count at diagnosis, immunophenotype (B cell or T cell), cytogenetic analysis, karyotyping, steroid response, cerebrospinal fluid (CSF) analysis for CNS disease, and MRD assessment by flow cytometry.
Remission status was assessed by morphology and MRD, and details of relapses/death during the study period were documented. An absolute blast count of fewer than 1,000 cells defined a good response to steroids. The toxicity of pegylated L-asparaginase in terms of hypersensitivity reactions, pancreatitis, thrombosis, hypoalbuminemia, liver dysfunction, hypofibrinogenemia, need for fresh frozen plasma (FFP) transfusion, and coagulopathy were noted. Severity of complications was classified according to the standard National Cancer Institute (NCI) criteria. Minimal residual disease level of 0.01% after evaluating minimum 50,000 flow cytometry events was defined as negative MRD.
A dose of pegylated L-asparaginase (Hamsyl) 1000 units/m2 was used throughout the protocol. One vial of Hamsyl (3750 IU/5 mL) was shared among two or three children (if feasible). An opened vial was used within 4 hours, and the rest discarded as per the manufacturer's recommendations. The parents of patients shared the expenses proportionately. The cold chain was maintained throughout as per the recommendations until clinical use.
Data were recorded on a pre-designed proforma, tabulated, and the results were analyzed statistically using the SPSS statistical software. Data were checked for normality of distribution, and continuous variables were compared by student's t-test if normally distributed or Mann–Whitney U test if the distribution is skewed. In addition, categorical variables were compared by Pearson's Chi-square test and Fisher's exact test. The level of significance was considered at a p-value less than 0.05.
Results
Demographic Profile
The study included 109 patients, aged 18 years and below, with ALL. Eighty-eight patients (80.7%) and 21(19.3%) had received generic pegylated-L-asparaginase and conventional asparaginase, respectively. Seventeen and 72 patients with B-type lymphoblastic leukemia at diagnosis received conventional and generic pegylated-L-asparaginase, respectively. Four and 16 patients with T-type lymphoblastic leukemia received conventional and generic pegylated-L-asparaginase, respectively. At the time of diagnosis, 15 children and 66 children with WBC count above 50,000/mm3 had received conventional L-asparaginase and generic pegylated-L-asparaginase, respectively. The demographic profile of children at the time of diagnosis is depicted in [Table 1].
Disease Characteristics
The disease characteristics of patients included in the study are presented in [Table 2]. Our cohort comprised 95.4% of newly diagnosed and 4.6% of relapsed leukemia. Based on immunophenotyping/immunohistochemistry, 79.8% had B-ALL, 1.8% had B-lymphoblastic lymphoma, 13.7% had T-ALL, and 4.6% had T-lymphoblastic lymphoma. Total white blood cell [WBC] count above 50,000/mm3 was noted in 25.7% of cases, and hyperleukocytosis (WBC > 100,000/mm3) was observed in 18.3% of children.
Abbreviations: ALL, acute lymphoblastic leukemia; MRD, minimal residual disease.
In our study, 39.4% of children were stratified as standard risk, 15.6% in intermediate-risk, and 45% of children had high risk as per the ICiCLe protocol. None of them had upfront CNS involvement at diagnosis; however, 3/109 had early CNS relapse. In addition, upfront testicular involvement was seen in 2/68 boys, and 2 had isolated testicular disease at relapse.
In our cohort, 93.6% had good early response to steroids. End of induction MRD was positive in 19.3%, of whom only one had positive MRD status at the end of augmented consolidation qualifying for refractory disease.
Side Effects of Generic Pegylated L-asparaginase
Allergic reactions were noted in 10.1% of children (11/109 children; 3/21 in conventional and 8/88 in pegylated L-asparaginase group), of whom nine had grade−1 reactions; one patient each had grade−2 and grade−4 reactions. In one child who received pegylated-L-asparaginase (0.9%), further doses had to be deferred due to anaphylaxis. Another complication, pancreatitis, was seen in 1.8% (2/109; 1 with conventional asparaginase and 1 with pegylated L-asparaginase) and central venous thrombosis in 0.9% (1/109 in pegylated L-asparaginase group) of children. In addition, altered liver enzymes were reported in 1.8%, hyperglycemia in 1.8%, and hypofibrinogenemia in 5.5% of cases. None of them had altered coagulation profiles or hyperbilirubinemia.
Disease Status at Follow-Up
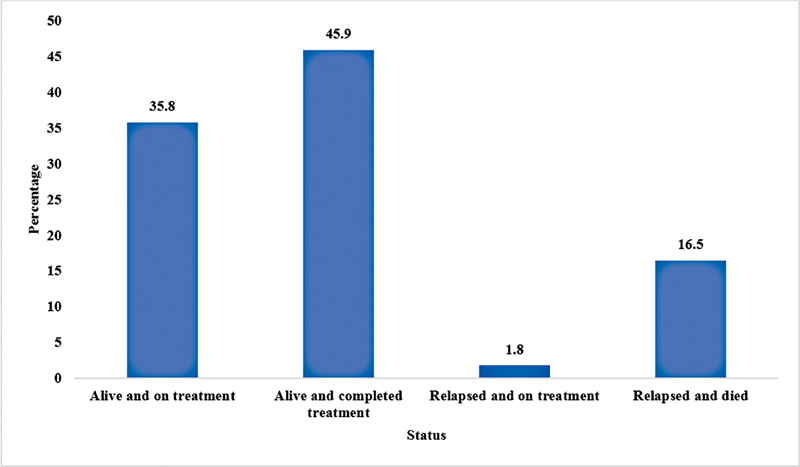
At the time of study, 35.8% of children were alive and receiving maintenance treatment, and 45.9% of children were alive after treatment ([Fig. 1]). Among 11% of children with relapsed disease (12/109), three continued chemotherapies, two were successfully salvaged with chemotherapy alone, three underwent hematopoietic stem cell transplant, one was lost to follow-up, and six had refractory/progressive disease and died.
Discussion
In our cohort, generic pegylated-L-asparaginase (Hamsyl) was effective and safe for use in children with ALL. Although pegylated-L-asparaginase has largely replaced the conventional asparaginase regimen in developed countries, its use in developing countries is limited by financial constraints.[14] However, given its potential safety, efficacy, and ease of administration, pegylated L-asparaginase is an important therapeutic option.[17] A generic formulation bioequivalent to innovator pegaspargase (Oncaspar) would be a cost-effective option in treating ALL.[15] Generic pegylated-L-asparaginase (Hamsyl) available in India, manufactured by Emcure Pharmaceuticals, is the DCGI-approved generic version of pegaspargase.[16]
Asparaginase activity level of 0.1 IU/mL is necessary for adequate depletion of asparagine. Krishnamurthy et al established the bioequivalence of generic pegylated-L-asparaginase (Hamsyl) and innovator pegasparagase (Oncaspar). Patients treated with generic pegylated-L-asparaginase (Hamsyl) or innovator pegasparagase achieved more than the recommended asparaginase levels at day 14.[15]
Following a single intramuscular injection of pegaspargase, the peak asparaginase activity (≈1 IU/mL) was reached by day 5, and the half-life was 1.7 days. Similarly, following a single intravenous injection, the peak asparaginase activity of 1.6 IU/mL was reached within 1.25 hours.[8] No dose adjustments are required for patients with renal and liver impairment.[11] [12] In the bioequivalent study, maximum plasma concentration, trough concentrations, half-life volume of distribution, drug clearance, and changes in the asparagine and glutamine levels were not significantly different between the generic and innovator pegaspargase.[15]
Studies comparing the efficacy of native asparaginase and pegylated-L-asparaginase have shown that both treatments are effective.[16] [17] However, the advantages of pegylated-L-asparaginase include rapid clearance of blast, prolonged asparaginase activity, better CNS penetration, and low titer of antibodies compared with native asparaginase.[17]
A few studies have evaluated the effect of generic pegylated-L-asparaginase in children with ALL. Indian experience with generic pegylated L-asparaginase (Hamsyl) has been promising. Vyas et al compared the clinical utility of native L-asparaginase (n = 52) and generic pegylated L-asparaginase (Hamsyl; n = 54) in children with ALL. The mean trough levels were higher in the pegylated-L-asparaginase (Hamsyl) arm. There was no difference in the toxicity profile between the two treatment arms in the induction phase. However, clinical and subclinical hypersensitivity were lower in the pegylated-L-asparaginase (Hamsyl) arm in the re-induction phase. Two-year event-free survival in the generic pegylated-L-asparaginase (Hamsyl) and native asparaginase treatment arms was 84% and 80.7%, respectively (p = 0.85). Generic pegylated-L-asparaginase (Hamsyl) was efficacious, well-tolerated, and adequate therapeutic levels were maintained for 2 weeks.[16]
In the review by Arora et al, 23 to 37% of children with ALL had a baseline WBC count of > 50,000/mm3, and T cell lymphoblastic leukemia was reported in 21 to 50% of children with ALL.[4] Among 3761 children with ALL, 2 to 6% had CNS involvement. In our study, none of the patients had CNS disease.[4] In all, 25.7% of children in our cohort had WBC count was > 50,000/mm3, and 18.3% had T cell lymphoblastic leukemia.
Minimal residual disease serves as a measure of early response to treatment.[18] In our study, at the end of induction, 19.8% and 80.7% of patients were MRD-positive and -negative, respectively. One patient remained MRD-positive at the end of augmented consolidation therapy. At the end of induction with pegasparagase, Jayaraman et al reported that 25% of children (53/211) were MRD-positive requiring augmented therapy.[14]
Native and pegylated-L-asparaginase largely differ in immunogenicity and pharmacokinetic properties.[19] [20] [21] Half-life of pegylated-L-asparaginase is five times longer than native asparaginase, which clinically transforms to a less frequent administration and fewer hospital visits.[17] Absorption of pegylated-L-asparaginase from the intramuscular site was slower (5 days) than native asparaginase.[17]
L-Asparaginase is of bacterial origin and can elicit either a clinical or subclinical immune response in children.[22] The clinical hypersensitivity accounted for up to 75% of children treated with native asparaginase and is the reason for its discontinuation.[22] [23] Hypersensitivity to asparaginase could affect the treatment efficacy as it leads to increased antibody levels and low asparaginase activity. Pegaspargase is associated with lesser clinical hypersensitivity than native asparaginase. Hypersensitivity to pegylated-L-asparaginase is frequently reported in children who are previously exposed to native asparaginase.[22] Occurrence of immune reactions also depends on L-asparaginase formulation, concomitant medications, and treatment intensity. Recurrent exposures, consolidation/re-induction treatment, and treatment interruption increase the levels of antibody formation.[17] [22] [24] Corticosteroids used in the treatment protocol can mask clinical hypersensitivity symptoms and lead to suboptimal asparaginase activity.[17] [22]
Sub-clinical hypersensitivity also leads to the development of antibodies and reduced asparaginase activity, but patients may lack clinical symptoms. Subclinical hypersensitivity is challenging to identify and, if not addressed, can lead to treatment failure.[25] Subclinical hypersensitivity has been reported in 8 to 29% of patients receiving native asparaginase.[25] Non-antibody mediated infusion reactions can also occur.[26] Hence, therapeutic drug level monitoring should be done to identify patients with suboptimal drug activity and adjust the treatment accordingly.[8] However, access to sophisticated tests is not possible in routine practical use. Glutamine depletion was used to monitor the L-asparaginase activity and was slower for pegaspargase, leading to fewer side effects.[27]
L-asparaginase treatment is associated with hyperglycemia, pancreatitis, thrombosis, encephalopathy, myelosuppression, and liver toxicity. In addition, asparaginase can reduce insulin production and insulin receptor resistance, primarily when used concomitantly with steroids. Asparaginase-associated hyperglycemia is seen in 4 to 20% of children.[28] Asparaginase can lead to an elevation in bilirubin, alkaline phosphatase, and hepatic transaminases. In children receiving multiagent chemotherapy, an abnormal liver function has been found in 30 to 60% of cases.[29] The incidence of liver toxicity is lesser with pegylated L-asparaginase compared with native asparaginase.[30] Pancreatitis has been attributed to the depletion of asparagine and occurs in 2 to 18% of children undergoing chemotherapy with multiagent drugs.[31] Recurrence of pancreatitis has been reported in up to 63% of patients.[32] Kamat et al also reported pancreatitis (n = 4) and venous thrombosis (n = 4) as significant adverse events.[33] Hepatic, lipid abnormalities, and coagulopathy warranting intervention were the other side-effects.[33] Like other reports, our cohort also showed low incidence (<5%) of pancreatitis, hyperglycemia, altered liver enzymes, and low fibrinogen.
Asparaginase leads to a decrease in the number of proteins involved in coagulation, mainly anti-thrombin-III leading to thrombosis in up to 2 to 7% cases. Fibrinogen is a surrogate marker for coagulation protein depletion. Fresh frozen plasma is initiated to improve the levels of anti-thrombin III and prevent thrombosis.[14] [34] Only one child with cerebral venous thrombosis in our cohort required FFP and enoxaparin. The patient could be safely re-challenged with pegylated-L-asparaginase after clinical recovery and thrombosis resolution as documented on imaging. In our center, we did not routinely monitor fibrinogen or transfused FFP. There was no incidence of hyperbilirubinemia /altered coagulation profile in our study.
Encephalopathy can occur due to elevated ammonia levels following treatment with asparaginase.[35] Asparaginase has been found to cause myelosuppression directly or alter the myelosuppressive property of other agents.[36] [37] There was no incidence of encephalopathy or significant myelosuppression in our study.
Verma et al. reported that 10 patients with prior hypersensitivity reactions to pegaspargase could be treated with a safe, cost-effective standard desensitization protocol (diluted medication [1:100] administered over 6 hours). Sustained asparaginase level > 0.05 IU/mL > 0.1 IU/mL could be maintained for 4 to 7 days and 10 to 14 days, respectively.[38]
The difference in efficacy between different asparaginase is related to suboptimal dosing, which leads to low asparaginase activity. Dose adjustments to yield therapeutic levels of asparaginase activity are needed indicating the importance of drug monitoring. Subclinical hypersensitivity, interpersonal variation, and differences in pharmacokinetics among different asparaginase preparations have underscored the need for therapeutic drug monitoring. Individual dosing as per drug monitoring can lead to a better outcome in terms of relapses and event-free survival rates.[39]
Generic asparaginase can be used as a safe and cost-effective alternative for children with ALL.[15] The cost of pegylated asparaginase treatment is comparable to native asparaginase, taking into account the reduced number of doses and clinical visits using pegylated asparaginase.[17] Moreover, a UK-based cost-utility analysis confirmed the cost-effectiveness of pegaspargase versus native asparaginase in terms of lower hypersensitivity rates and the need for fewer injections.[40] The National Institute for Health and Care Excellence (NICE) guidelines suggest pegylated-L-asparaginase as a cost-effective drug in treating children with ALL.[41] To contain the cost of generic pegylated asparaginase (Hamsyl), we used indigenous methods such as pooling the patients without majorly altering the protocol.
Conclusion
The generic pegylated-L-asparaginase (Hamsyl) was effective and safe to use in pediatric ALL management. The safety profile of generic pegylated-L-asparaginase was similar to those reported with innovator pegaspargase and other studies involving generic formulation of pegylated-L-asparaginase. Although cost is a significant limitation, historical study reviews suggest that pegylated-L-asparaginase would be cost-effective considering the reduced number of drug administrations and low hypersensitivity reactions. Practically, an upfront reduction in cost could be realized by adopting the indigenous method of sharing the drug. However, further studies on a larger population are warranted to validate these results.
All named authors for this manuscript meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. All authors take full responsibility for the integrity of the work and have given final approval for the published version.
Conflict of Interest
None declared.
Acknowledgments
The authors acknowledge Dr. Punit Srivastava from Mediception Science Pvt. Ltd., Gurugram, India, for providing writing and editing assistance for this project.
-
References
- 1 Ganguly S, Kinsey S, Bakhshi S. Childhood cancer in India. Cancer Epidemiol 2021; 71 (Pt B): 101679
- 2 Childhood Acute Lymphoblastic Leukemia Treatment. (PDQ®)–Health Professional Version - National Cancer Institute [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.cancer.gov/types/leukemia/hp/child-all-treatment-pdq
- 3 Asthana S, Labani S, Mehrana S, Bakhshi S. Incidence of childhood leukemia and lymphoma in India. Pediatr Hematol Oncol J 2018; 3 (04) 115-120
- 4 Arora RS, Arora B. Acute leukemia in children: a review of the current Indian data. South Asian J Cancer 2016; 5 (03) 155-160
- 5 Pui C-H, Yang JJ, Hunger SP. et al. Childhood acute lymphoblastic leukemia: progress through collaboration. J Clin Oncol 2015; 33 (27) 2938-2948
- 6 Kidd JG. Regression of transplanted lymphomas induced in vivo by means of normal guinea pig serum. I. Course of transplanted cancers of various kinds in mice and rats given guinea pig serum, horse serum, or rabbit serum. J Exp Med 1953; 98 (06) 565-582
- 7 Broome JD. Evidence that the L-asparaginase of guinea pig serum is responsible for its antilymphoma effects. I. Properties of the L-asparaginase of guinea pig serum in relation to those of the antilymphoma substance. J Exp Med 1963; 118 (01) 99-120
- 8 Heo YA, Syed YY, Keam SJ. Pegaspargase: A Review in Acute Lymphoblastic Leukaemia. Drugs 2019; 79 (07) 767-777
- 9 Egler RA, Ahuja SP, Matloub Y. L-asparaginase in the treatment of patients with acute lymphoblastic leukemia. J Pharmacol Pharmacother 2016; 7 (02) 62-71
- 10 Angiolillo AL, Schore RJ, Devidas M. et al. Pharmacokinetic and pharmacodynamic properties of calaspargase pegol Escherichia coli L-asparaginase in the treatment of patients with acute lymphoblastic leukemia: results from Children's Oncology Group Study AALL07P4. J Clin Oncol 2014; 32 (34) 3874-3882
- 11 Shire Pharmaceuticals. Oncaspar (pegaspargase): US prescribing information. 2020 [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/193411s5196lbl.pdf
- 12 European Medicines Agency. Oncaspar (pegaspargase): Summary of product characteristics. 2020 [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.ema.europa.eu/en/documents/product-information/oncaspar-epar-product-information_en.pdf
- 13 Nelson textbook of Pediatrics. Robert M. Kliegman, Joseph W. St Geme, Nathan J. Blum, Samir S. Shah, Robert C. Tasker, Karen M. Wilson; eds., emeritus Richard E. Behrman. Elsevier Inc., Philadelphia, PA,2019
- 14 Jayaraman D, Uppuluri R, Swaminathan VV, Sivasankaran M, Patel S, Raj R. Affordable and safe health care for all children: lessons learned from the use of peg-asparaginase in a developing country. Indian J Med Paediatr Oncol 2017; 38 (03) 398-400
- 15 Nookala Krishnamurthy M, Narula G, Gandhi K. et al. Randomized, parallel group, open-label bioequivalence trial of intramuscular pegaspargase in patients with relapsed acute lymphoblastic leukemia. JCO Glob Oncol 2020; 6 (06) 1009-1016
- 16 Vyas C, Jain S, Kapoor G, Mehta A, Takkar Chugh P. Experience with generic pegylated L-asparaginase in children with acute lymphoblastic leukemia and monitoring of serum asparaginase activity. Pediatr Hematol Oncol 2018; 35 (5-6): 331-340
- 17 Avramis VI, Sencer S, Periclou AP. et al. A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children's Cancer Group study. Blood 2002; 99 (06) 1986-1994
- 18 Kwok CS, Kham SK, Ariffin H, Lin HP, Quah TC, Yeoh AE. Minimal residual disease (MRD) measurement as a tool to compare the efficacy of chemotherapeutic drug regimens using Escherichia coli-asparaginase or Erwinia-asparaginase in childhood acute lymphoblastic leukemia (ALL). Pediatr Blood Cancer 2006; 47 (03) 299-304
- 19 Abuchowski A, Kazo GM, Verhoest Jr CR. et al. Cancer therapy with chemically modified enzymes. I. Antitumor properties of polyethylene glycol-asparaginase conjugates. Cancer Biochem Biophys 1984; 7 (02) 175-186
- 20 Asselin BL, Whitin JC, Coppola DJ, Rupp IP, Sallan SE, Cohen HJ. Comparative pharmacokinetic studies of three asparaginase preparations. J Clin Oncol 1993; 11 (09) 1780-1786
- 21 Keating MJ, Holmes R, Lerner S, Ho DH. L-asparaginase and PEG asparaginase–past, present, and future. Leuk Lymphoma 1993; 10 (1, suppl) 153-157
- 22 Hijiya N, van der Sluis IM. Asparaginase-associated toxicity in children with acute lymphoblastic leukemia. Leuk Lymphoma 2016; 57 (04) 748-757
- 23 Wacker P, Land VJ, Camitta BM. et al; Children's Oncology Study Group. Allergic reactions to E. coli L-asparaginase do not affect outcome in childhood B-precursor acute lymphoblastic leukemia: a Children's Oncology Group Study. J Pediatr Hematol Oncol 2007; 29 (09) 627-632
- 24 Woo MH, Hak LJ, Storm MC. et al. Hypersensitivity or development of antibodies to asparaginase does not impact treatment outcome of childhood acute lymphoblastic leukemia. J Clin Oncol 2000; 18 (07) 1525-1532
- 25 Panosyan EH, Seibel NL, Martin-Aragon S. et al; Children's Cancer Group Study CCG-1961. Asparaginase antibody and asparaginase activity in children with higher-risk acute lymphoblastic leukemia: Children's Cancer Group Study CCG-1961. J Pediatr Hematol Oncol 2004; 26 (04) 217-226
- 26 Tong WH, Pieters R, Kaspers GJL. et al. A prospective study on drug monitoring of PEGasparaginase and Erwinia asparaginase and asparaginase antibodies in pediatric acute lymphoblastic leukemia. Blood 2014; 123 (13) 2026-2033
- 27 Boos J, Werber G, Ahlke E. et al. Monitoring of asparaginase activity and asparagine levels in children on different asparaginase preparations. Eur J Cancer 1996; 32A (09) 1544-1550
- 28 Pui CH, Burghen GA, Bowman WP, Aur RJA. Risk factors for hyperglycemia in children with leukemia receiving L-asparaginase and prednisone. J Pediatr 1981; 99 (01) 46-50
- 29 Stock W, Douer D, DeAngelo DJ. et al. Prevention and management of asparaginase/pegasparaginase-associated toxicities in adults and older adolescents: recommendations of an expert panel. Leuk Lymphoma 2011; 52 (12) 2237-2253
- 30 Dinndorf PA, Gootenberg J, Cohen MH, Keegan P, Pazdur R. FDA drug approval summary: pegaspargase (oncaspar) for the first-line treatment of children with acute lymphoblastic leukemia (ALL). Oncologist 2007; 12 (08) 991-998
- 31 Raja RA, Schmiegelow K, Frandsen TL. Asparaginase-associated pancreatitis in children. Br J Haematol 2012; 159 (01) 18-27
- 32 Kearney SL, Dahlberg SE, Levy DE, Voss SD, Sallan SE, Silverman LB. Clinical course and outcome in children with acute lymphoblastic leukemia and asparaginase-associated pancreatitis. Pediatr Blood Cancer 2009; 53 (02) 162-167
- 33 Kamat A. Retrospective post-marketing study on the use of bio-similar pegasparagase among acute lymphoblastic leukemia patients in India. Pediatr Hematol Oncol J 2018; 3 (01) 9-12
- 34 Payne JH, Vora AJ. Thrombosis and acute lymphoblastic leukaemia. Br J Haematol 2007; 138 (04) 430-445
- 35 Hourani R, Abboud M, Hourani M, Khalifeh H, Muwakkit S. L-asparaginase-induced posterior reversible encephalopathy syndrome during acute lymphoblastic leukemia treatment in children. Neuropediatrics 2008; 39 (01) 46-50
- 36 Merryman R, Stevenson KE, Gostic II WJ. et al. Asparaginase-associated myelosuppression and effects on dosing of other chemotherapeutic agents in childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 2012; 59 (05) 925-927
- 37 Parsons SK, Skapek SX, Neufeld EJ. et al. Asparaginase-associated lipid abnormalities in children with acute lymphoblastic leukemia. Blood 1997; 89 (06) 1886-1895
- 38 Verma A, Chen K, Bender C, Gorney N, Leonard W, Barnette P. PEGylated E. coli asparaginase desensitization: an effective and feasible option for pediatric patients with acute lymphoblastic leukemia who have developed hypersensitivity to pegaspargase in the absence of asparaginase Erwinia chrysanthemi availability. Pediatr Hematol Oncol 2019; 36 (05) 277-286
- 39 Vrooman LM, Stevenson KE, Supko JG. et al. Postinduction dexamethasone and individualized dosing of Escherichia Coli L-asparaginase each improve outcome of children and adolescents with newly diagnosed acute lymphoblastic leukemia: results from a randomized study–Dana-Farber Cancer Institute ALL Consortium Protocol 00-01. J Clin Oncol 2013; 31 (09) 1202-1210
- 40 Hu X, Wildman KP, Basu S, Lin PL, Rowntree C, Saha V. The cost-effectiveness of pegaspargase versus native asparaginase for first-line treatment of acute lymphoblastic leukaemia: a UK-based cost-utility analysis. Health Econ Rev 2019; 9 (01) 40
- 41 NICE. Pegaspargase-for-treating-acute-lymphoblastic-leukaemia-pdf-82604549478085.pdf [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.nice.org.uk/guidance/ta408/resources/pegaspargase-for-treating-acute-lymphoblastic-leukaemia-pdf-82604549478085
Address for correspondence
Publication History
Article published online:
10 April 2023
© 2023. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ganguly S, Kinsey S, Bakhshi S. Childhood cancer in India. Cancer Epidemiol 2021; 71 (Pt B): 101679
- 2 Childhood Acute Lymphoblastic Leukemia Treatment. (PDQ®)–Health Professional Version - National Cancer Institute [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.cancer.gov/types/leukemia/hp/child-all-treatment-pdq
- 3 Asthana S, Labani S, Mehrana S, Bakhshi S. Incidence of childhood leukemia and lymphoma in India. Pediatr Hematol Oncol J 2018; 3 (04) 115-120
- 4 Arora RS, Arora B. Acute leukemia in children: a review of the current Indian data. South Asian J Cancer 2016; 5 (03) 155-160
- 5 Pui C-H, Yang JJ, Hunger SP. et al. Childhood acute lymphoblastic leukemia: progress through collaboration. J Clin Oncol 2015; 33 (27) 2938-2948
- 6 Kidd JG. Regression of transplanted lymphomas induced in vivo by means of normal guinea pig serum. I. Course of transplanted cancers of various kinds in mice and rats given guinea pig serum, horse serum, or rabbit serum. J Exp Med 1953; 98 (06) 565-582
- 7 Broome JD. Evidence that the L-asparaginase of guinea pig serum is responsible for its antilymphoma effects. I. Properties of the L-asparaginase of guinea pig serum in relation to those of the antilymphoma substance. J Exp Med 1963; 118 (01) 99-120
- 8 Heo YA, Syed YY, Keam SJ. Pegaspargase: A Review in Acute Lymphoblastic Leukaemia. Drugs 2019; 79 (07) 767-777
- 9 Egler RA, Ahuja SP, Matloub Y. L-asparaginase in the treatment of patients with acute lymphoblastic leukemia. J Pharmacol Pharmacother 2016; 7 (02) 62-71
- 10 Angiolillo AL, Schore RJ, Devidas M. et al. Pharmacokinetic and pharmacodynamic properties of calaspargase pegol Escherichia coli L-asparaginase in the treatment of patients with acute lymphoblastic leukemia: results from Children's Oncology Group Study AALL07P4. J Clin Oncol 2014; 32 (34) 3874-3882
- 11 Shire Pharmaceuticals. Oncaspar (pegaspargase): US prescribing information. 2020 [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/193411s5196lbl.pdf
- 12 European Medicines Agency. Oncaspar (pegaspargase): Summary of product characteristics. 2020 [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.ema.europa.eu/en/documents/product-information/oncaspar-epar-product-information_en.pdf
- 13 Nelson textbook of Pediatrics. Robert M. Kliegman, Joseph W. St Geme, Nathan J. Blum, Samir S. Shah, Robert C. Tasker, Karen M. Wilson; eds., emeritus Richard E. Behrman. Elsevier Inc., Philadelphia, PA,2019
- 14 Jayaraman D, Uppuluri R, Swaminathan VV, Sivasankaran M, Patel S, Raj R. Affordable and safe health care for all children: lessons learned from the use of peg-asparaginase in a developing country. Indian J Med Paediatr Oncol 2017; 38 (03) 398-400
- 15 Nookala Krishnamurthy M, Narula G, Gandhi K. et al. Randomized, parallel group, open-label bioequivalence trial of intramuscular pegaspargase in patients with relapsed acute lymphoblastic leukemia. JCO Glob Oncol 2020; 6 (06) 1009-1016
- 16 Vyas C, Jain S, Kapoor G, Mehta A, Takkar Chugh P. Experience with generic pegylated L-asparaginase in children with acute lymphoblastic leukemia and monitoring of serum asparaginase activity. Pediatr Hematol Oncol 2018; 35 (5-6): 331-340
- 17 Avramis VI, Sencer S, Periclou AP. et al. A randomized comparison of native Escherichia coli asparaginase and polyethylene glycol conjugated asparaginase for treatment of children with newly diagnosed standard-risk acute lymphoblastic leukemia: a Children's Cancer Group study. Blood 2002; 99 (06) 1986-1994
- 18 Kwok CS, Kham SK, Ariffin H, Lin HP, Quah TC, Yeoh AE. Minimal residual disease (MRD) measurement as a tool to compare the efficacy of chemotherapeutic drug regimens using Escherichia coli-asparaginase or Erwinia-asparaginase in childhood acute lymphoblastic leukemia (ALL). Pediatr Blood Cancer 2006; 47 (03) 299-304
- 19 Abuchowski A, Kazo GM, Verhoest Jr CR. et al. Cancer therapy with chemically modified enzymes. I. Antitumor properties of polyethylene glycol-asparaginase conjugates. Cancer Biochem Biophys 1984; 7 (02) 175-186
- 20 Asselin BL, Whitin JC, Coppola DJ, Rupp IP, Sallan SE, Cohen HJ. Comparative pharmacokinetic studies of three asparaginase preparations. J Clin Oncol 1993; 11 (09) 1780-1786
- 21 Keating MJ, Holmes R, Lerner S, Ho DH. L-asparaginase and PEG asparaginase–past, present, and future. Leuk Lymphoma 1993; 10 (1, suppl) 153-157
- 22 Hijiya N, van der Sluis IM. Asparaginase-associated toxicity in children with acute lymphoblastic leukemia. Leuk Lymphoma 2016; 57 (04) 748-757
- 23 Wacker P, Land VJ, Camitta BM. et al; Children's Oncology Study Group. Allergic reactions to E. coli L-asparaginase do not affect outcome in childhood B-precursor acute lymphoblastic leukemia: a Children's Oncology Group Study. J Pediatr Hematol Oncol 2007; 29 (09) 627-632
- 24 Woo MH, Hak LJ, Storm MC. et al. Hypersensitivity or development of antibodies to asparaginase does not impact treatment outcome of childhood acute lymphoblastic leukemia. J Clin Oncol 2000; 18 (07) 1525-1532
- 25 Panosyan EH, Seibel NL, Martin-Aragon S. et al; Children's Cancer Group Study CCG-1961. Asparaginase antibody and asparaginase activity in children with higher-risk acute lymphoblastic leukemia: Children's Cancer Group Study CCG-1961. J Pediatr Hematol Oncol 2004; 26 (04) 217-226
- 26 Tong WH, Pieters R, Kaspers GJL. et al. A prospective study on drug monitoring of PEGasparaginase and Erwinia asparaginase and asparaginase antibodies in pediatric acute lymphoblastic leukemia. Blood 2014; 123 (13) 2026-2033
- 27 Boos J, Werber G, Ahlke E. et al. Monitoring of asparaginase activity and asparagine levels in children on different asparaginase preparations. Eur J Cancer 1996; 32A (09) 1544-1550
- 28 Pui CH, Burghen GA, Bowman WP, Aur RJA. Risk factors for hyperglycemia in children with leukemia receiving L-asparaginase and prednisone. J Pediatr 1981; 99 (01) 46-50
- 29 Stock W, Douer D, DeAngelo DJ. et al. Prevention and management of asparaginase/pegasparaginase-associated toxicities in adults and older adolescents: recommendations of an expert panel. Leuk Lymphoma 2011; 52 (12) 2237-2253
- 30 Dinndorf PA, Gootenberg J, Cohen MH, Keegan P, Pazdur R. FDA drug approval summary: pegaspargase (oncaspar) for the first-line treatment of children with acute lymphoblastic leukemia (ALL). Oncologist 2007; 12 (08) 991-998
- 31 Raja RA, Schmiegelow K, Frandsen TL. Asparaginase-associated pancreatitis in children. Br J Haematol 2012; 159 (01) 18-27
- 32 Kearney SL, Dahlberg SE, Levy DE, Voss SD, Sallan SE, Silverman LB. Clinical course and outcome in children with acute lymphoblastic leukemia and asparaginase-associated pancreatitis. Pediatr Blood Cancer 2009; 53 (02) 162-167
- 33 Kamat A. Retrospective post-marketing study on the use of bio-similar pegasparagase among acute lymphoblastic leukemia patients in India. Pediatr Hematol Oncol J 2018; 3 (01) 9-12
- 34 Payne JH, Vora AJ. Thrombosis and acute lymphoblastic leukaemia. Br J Haematol 2007; 138 (04) 430-445
- 35 Hourani R, Abboud M, Hourani M, Khalifeh H, Muwakkit S. L-asparaginase-induced posterior reversible encephalopathy syndrome during acute lymphoblastic leukemia treatment in children. Neuropediatrics 2008; 39 (01) 46-50
- 36 Merryman R, Stevenson KE, Gostic II WJ. et al. Asparaginase-associated myelosuppression and effects on dosing of other chemotherapeutic agents in childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 2012; 59 (05) 925-927
- 37 Parsons SK, Skapek SX, Neufeld EJ. et al. Asparaginase-associated lipid abnormalities in children with acute lymphoblastic leukemia. Blood 1997; 89 (06) 1886-1895
- 38 Verma A, Chen K, Bender C, Gorney N, Leonard W, Barnette P. PEGylated E. coli asparaginase desensitization: an effective and feasible option for pediatric patients with acute lymphoblastic leukemia who have developed hypersensitivity to pegaspargase in the absence of asparaginase Erwinia chrysanthemi availability. Pediatr Hematol Oncol 2019; 36 (05) 277-286
- 39 Vrooman LM, Stevenson KE, Supko JG. et al. Postinduction dexamethasone and individualized dosing of Escherichia Coli L-asparaginase each improve outcome of children and adolescents with newly diagnosed acute lymphoblastic leukemia: results from a randomized study–Dana-Farber Cancer Institute ALL Consortium Protocol 00-01. J Clin Oncol 2013; 31 (09) 1202-1210
- 40 Hu X, Wildman KP, Basu S, Lin PL, Rowntree C, Saha V. The cost-effectiveness of pegaspargase versus native asparaginase for first-line treatment of acute lymphoblastic leukaemia: a UK-based cost-utility analysis. Health Econ Rev 2019; 9 (01) 40
- 41 NICE. Pegaspargase-for-treating-acute-lymphoblastic-leukaemia-pdf-82604549478085.pdf [Internet]. [cited 2021 Jun 21]. Accessed Nov 23, 2022, at: https://www.nice.org.uk/guidance/ta408/resources/pegaspargase-for-treating-acute-lymphoblastic-leukaemia-pdf-82604549478085