

Subscribe to RSS
DOI: 10.1055/s-0043-1768155
When May Cochlear Implant Not Work Even at a Very Young Age?
Authors


Multichannel cochlear implant is the first neural prosthesis to bring electronic technology effectively and safely into a direct physiological relation with the central nervous system and human consciousness.[1]
Among children, classical candidates to cochlear implantation are those presenting bilateral severe to profound hearing loss when amplification benefits are limited to the optimal auditory and language development.[2] [3]
Despite the remarkable contribution to the access of speech sounds, cochlear implant outcomes vary considerably depending on several factors.[4] Sharma et al.[5] (2002) suggested that a critical period of plasticity existed for developing brain connections, and early surgical intervention has been indicated ever since. Nevertheless, just 'opening' the doorway of the brain (the ears) to receive sounds may not be enough to allow their interpretation.[6]
Once the hearing loss is diagnosed, an early intervention program should begin to promote receptive and expressive language development. This program will require the child to be educated to maximally use hearing with the cochlear implant.[1] [7] [8]
Listening presupposes an intentional activity. In listening, one is actively trying to focus on some sounds. In contrast, hearing may happen without necessarily paying attention or intention. It is possible to hear something even when you don't want to hear it and try not to hear it. The brain pathways used in 'listening' and simply hearing are different. When listening, in addition to paying attention to what we hear, it implies finding the pathways that lead to attributing representation to that sound, that could be a meaning or a feeling stored in memory. To hear, it is enough to detect, sound can pass through the ear and reach the temporal lobe, without connecting to symbolic or meaningful associations. When one really 'want' to listen, must pay attention, intention, and trigger association pathways to the 'end point' where there must have stored information, so that the input message can be compared to previous listening experiences, be understood and ́make sensé. At the extreme, one may put all the attention and intention into listening to someone talking in Russian, while nothing that was heard was understood, if one does not have meaningful stored information. Thus, to understand, it is necessary that the brain has a stored arsenal to be able to interpret the sound.
In the first years of life, everyone who is born with normal hearing thresholds, may be able to hear 'everything' and will store auditory experiences associated with sensations, emotions, and daily experiences that, through repetition and routine, will allow the creation of a significant arsenal (Flexer, 2011).[6] The 'meaningful arsenal' is achieved with emotional bonding among the family members (that will give the motivation to the intention to hear, or listening) and is the basis of language. Language will be transmitted as speech (oral language) when a connection among the ascending auditory pathways, meaningful association pathways and the descending motor efferent pathways are linked. The language is accumulated with the experiences that generate the processing of several stations, regardless of the way it will be expressed.
ASHA[9] summarizes some expected landmarks in the auditory and speech development ([Table 1]) in children with typical hearing. Although they may have thresholds within normal ranges, they only respond reflexively to loud sounds during the first three months of life. They begin to imitate speech sounds only after more than 7 months of repeated auditory experiences and motor maturity in the tongue and mouth, revealing the connection between the afferent auditory and the efferent speech motor pathways. They will point out body parts around 12 months old, after taking at least 365 baths or showers, listening in a pleasant and playful environment with their parents and caregivers.
|
Hearing and comprehension |
Speech |
|---|---|
|
Birth to 3 months |
|
|
Startles with loud sounds Be quiet or smile when spoken to |
Makes pleasant sounds Smile when sees mom/dad |
|
4 to 7 months |
|
|
Moves eyes in the direction of sounds Notices toys that make noise |
Babbles different speech sounds Vocalizes while playing |
|
7 to 12 months |
|
|
Turn and look in the direction of the sound source Starts responding to requests ('come here') |
Babbling has both long and short sounds. Imitates different speech sounds |
|
1 to 2 years |
|
|
Points to some body parts Follows simple orders (where's the shoe) |
Says a new word every month Uses 1-2 word phrases and questions |
Hence, the construction of language is the result of countless experiences and situations stored and associated by synaptic connections, that are potentiated by emotions and hormones.[10]
As mentioned earlier, when the child is born with severe to profound hearing loss and conventional amplification hearing aids are not able to stimulate all the tonotopic regions of the cochlea and cochlear nerve with speech sounds, the cochlear implant will be indicated to allow access to the necessary acoustic cues. This may allow the development of auditory skills, the experience of representative situations, culminating in oral language.[11]
Diagnosis at birth or in the first month is very important so that the necessary actions for intervention are taken in time, that is, before 3 to 6 months, to allow this children have the meaningful experiences almost at the same time as their hearing peers.[7] The more adequate the auditory and linguistic development before the CI, the better the evolution after the surgery. As important as the diagnosis is the supporting and counseling of families. Families that are “paralyzed” in the diagnosis, not knowing how to deal with deaf children, without the adequate guidance might unconsciously becoming “mute families”. One of the possible reactions or tendencies when dealing with someone that may not be hearing us, may be 'not talking'. “What is the point of talking”, one may ask themselves, “if he/she won't listen to me'”. The importance of supporting families involved in the child's rehabilitation process has been reinforced and proven in numerous studies.[4] [10] [11] [12] [13] [14] [15] [16] Lind-Combs & Holt[15] (2022) conducted a study with 62 dyads of children with typical hearing and with hearing loss using conventional hearing aids or cochlear implants, between 3 and 8 years of age. They found that the vocabulary used by the family associated with a mental state (such as: I think that, I feel that) positively affected the inhibitory control of children using hearing devices. Hence, not only language development is impacted by family communication style, but the whole cognitive development.
The great contribution of rehabilitation is precisely to establish a partnership, strengthening guidance and advice to families of children with hearing loss to transform the home into a stimulating environment.
Thus, in addition to the the age at diagnosis and intervention with conventional hearing aids before 3 to 6 months of age, adequate and desired oral language development after early cochlear implantation will only happen when:
-
There is adequate family involvement and communication,
-
Residual hearing is effectively harnessed with hearing aids before the CI, while the greater the degree of hearing loss, the shorter the deprivation time should be,
-
Etiology allows proper insertion of electrodes and sufficient and adequate neural density of ganglion cells for electrical stimulation
-
The Map (programming) in the speech processor is adequate to allow optimized access to speech sounds and features
-
There are no other associated handicaps
-
Appropriate school and rehabilitation quality
-
Adequate nonverbal intelligence
-
And CI usage during all the waking hours, that is to say an average of 10 hours a day.
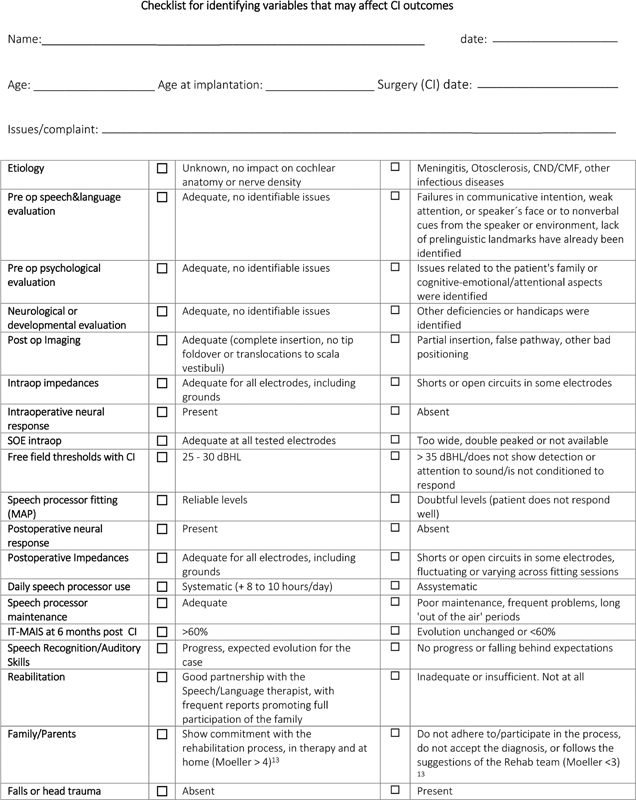
Pianesi et al.[17] (2016) warned that the risk of lack of oral language development can be identified in the first 6 months after CI, due to slow development of auditory skills identified by IT-MAIS. Silva-Comerlatto[18] has also studied 230 Brazilian kids with severe to profound hearing loss, and stablished the landmarks for auditory and oral language after cochlear implants. Therefore, children who do not demonstrate development in the first 6 months after CI should be considered as 'red flags' and actions such as the verification of the intervention (rehabilitation and family communication), speech processor programming and hours of use should be investigated.
Robbins[19] (2005) proposed a list of Red flags for both groups of children implanted early and late in life, up to 12 months after CI, that may also serve as markers for taking actions after cochlear implantation. Our proposal is that, if there is no expected evolution, a list of reasons may be reviewed to allow the identification of the aspects that may be driven ([figure 1]).
In summary
Cochlear implant is a remarkable solution to open the doorway to the brain,[6] but the factors that influence the development of oral language, that is, auditory and communicative skills in severe to profound deaf children, transcend the age of the cochlear implant surgery.
Furthermore, we must have in mind that in very early cochlear implantation, many other additional handicap diagnoses may appear later, after the surgery, including Autism Spectral Disorders.[20] [21]
Considering the individuality and characteristics of each child, it is the responsibility as the multidisciplinary team, including pediatricians, otorhinolaryngologists, speech therapists, social workers, psychologists, to offer support and the best possible guidance to the children and their families.
No conflict of interest has been declared by the author(s).
-
References
- 1 Clark GM. Personal reflections on the multichannel cochlear implant and a view of the future. J Rehabil Res Dev 2008; 45 (05) 651-693
- 2 Bento RF, Brito RV, Castilho AM, Goffi Gomez MVS, Giorgi SB, Guedes MC. Auditory results with multicanal cochlear implant in patients submitted to cochlear implant surgery at University of São Paulo Medical School - Hospital das Clínicas. Rev Bras Otorrinolaringol 2004; 70 (05) 632-637
- 3 Goffi-Gomez MVS, Guedes MC, Sant'Anna SBG, Peralta CGO, Tsuji RK, Castilho AM, Brito Neto RV, Bento RF. Critérios de Seleção e Avaliação Médica e Audiológica dos Candidatos ao Implante Coclear: Protocolo HCFMUSP [Medical and Audiological Selection Criteria and Evaluation for Cochlear Implants Candidates: HC-FMUSP Protocol.]. Arq Otorrinolaringol 2004; 8 (04) 303-323
- 4 Ching TYC, Dillon H, Leigh G, Cupples L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: summary of 5-year findings and implications. Int J Audiol 2018; 57 (sup2): S105-S111
- 5 Sharma A, Dorman MF, Spahr AJ. A sensitive period for the development of the central auditory system in children with cochlear implants: implications for age of implantation. Ear Hear 2002; 23 (06) 532-539
- 6 Flexer C. Cochlear implants and neuroplasticity: linking auditory exposure and practice. Cochlear Implants Int 2011; 12 (Suppl. 01) S19-S21
- 7 Bevilacqua MC, Alvarenga KdeF, Costa OA, Moret AL. The universal newborn hearing screening in Brazil: from identification to intervention. Int J Pediatr Otorhinolaryngol 2010; 74 (05) 510-515
- 8 Ching TY, Dillon H, Marnane V. et al. Outcomes of early- and late-identified children at 3 years of age: findings from a prospective population-based study. Ear Hear 2013; 34 (05) 535-552
- 9 ASHA. https://www.asha.org/public/speech/development/01/
- 10 Yoshinaga-Itano C, Sedey AL, Mason CA, Wiggin M, Chung W. Early Intervention, Parent Talk, and Pragmatic Language in Children With Hearing Loss. Pediatrics 2020; 146 (Suppl. 03) S270-S277
- 11 McConkey Robbins A, Koch DB, Osberger MJ, Zimmerman-Phillips S, Kishon-Rabin L. Effect of age at cochlear implantation on auditory skill development in infants and toddlers. Arch Otolaryngol Head Neck Surg 2004; 130 (05) 570-574
- 12 de Brito R, Bittencourt AG, Goffi-Gomez MV. et al. Cochlear implants and bacterial meningitis: A speech recognition study in paired samples. Int Arch Otorhinolaryngol 2013; 17 (01) 57-61
- 13 Moeller MP. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000; 106 (03) E43
- 14 Hoshino AC, Echegoyen A, Goffi-Gomez MV, Tsuji RK, Bento RF. Outcomes of Late Implantation in Usher Syndrome Patients. Int Arch Otorhinolaryngol 2017; 21 (02) 140-143
- 15 Lind-Combs HC, Holt RF. Associations Between Parent Mental State Language and Child Inhibitory Control in Children Who Are Deaf or Hard of Hearing. J Speech Lang Hear Res 2022; 65 (08) 3129-3145
- 16 Selleck AM, Park LR, Brown KD. Factors Influencing Pediatric Cochlear Implant Outcomes: Carolina Sibling Study. Otol Neurotol 2019; 40 (09) 1148-1152
- 17 Pianesi F, Scorpecci A, Giannantonio S, Micardi M, Resca A, Marsella P. Prelingual auditory-perceptual skills as indicators of initial oral language development in deaf children with cochlear implants. Int J Pediatr Otorhinolaryngol 2016; 82: 58-63
- 18 Silva-Comerlatto MP. Habilidades auditivas e de linguagem de crianças usuárias de implante coclear: análise dos marcadores clínicos de desenvolvimento. Tese (Doutorado). Available at https://teses.usp.br/teses/disponiveis/5/5143/tde-20052016-142644/pt-br.php
- 19 McConkey Robbins A. Monitoring Communication Progress in Early Intervention. IN: A Sound Foundation Through Early Amplification. Available at https://www.amymcconkeyrobbins.com/PDF/com_18_p61899_pho_kapitel_8.pdf
- 20 Eshraghi AA, Nazarian R, Telischi FF. et al. Cochlear Implantation in Children With Autism Spectrum Disorder. Otol Neurotol 2015; 36 (08) e121-e128
- 21 Nasralla HR, Montefusco AM, Hoshino ACH. et al. Benefit of Cochlear Implantation in Children with Multiple-handicaps: Parent's Perspective. Int Arch Otorhinolaryngol 2018; 22 (04) 415-427
Address for correspondence
Publication History
Article published online:
28 April 2023
© 2023. Fundação Otorrinolaringologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Clark GM. Personal reflections on the multichannel cochlear implant and a view of the future. J Rehabil Res Dev 2008; 45 (05) 651-693
- 2 Bento RF, Brito RV, Castilho AM, Goffi Gomez MVS, Giorgi SB, Guedes MC. Auditory results with multicanal cochlear implant in patients submitted to cochlear implant surgery at University of São Paulo Medical School - Hospital das Clínicas. Rev Bras Otorrinolaringol 2004; 70 (05) 632-637
- 3 Goffi-Gomez MVS, Guedes MC, Sant'Anna SBG, Peralta CGO, Tsuji RK, Castilho AM, Brito Neto RV, Bento RF. Critérios de Seleção e Avaliação Médica e Audiológica dos Candidatos ao Implante Coclear: Protocolo HCFMUSP [Medical and Audiological Selection Criteria and Evaluation for Cochlear Implants Candidates: HC-FMUSP Protocol.]. Arq Otorrinolaringol 2004; 8 (04) 303-323
- 4 Ching TYC, Dillon H, Leigh G, Cupples L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: summary of 5-year findings and implications. Int J Audiol 2018; 57 (sup2): S105-S111
- 5 Sharma A, Dorman MF, Spahr AJ. A sensitive period for the development of the central auditory system in children with cochlear implants: implications for age of implantation. Ear Hear 2002; 23 (06) 532-539
- 6 Flexer C. Cochlear implants and neuroplasticity: linking auditory exposure and practice. Cochlear Implants Int 2011; 12 (Suppl. 01) S19-S21
- 7 Bevilacqua MC, Alvarenga KdeF, Costa OA, Moret AL. The universal newborn hearing screening in Brazil: from identification to intervention. Int J Pediatr Otorhinolaryngol 2010; 74 (05) 510-515
- 8 Ching TY, Dillon H, Marnane V. et al. Outcomes of early- and late-identified children at 3 years of age: findings from a prospective population-based study. Ear Hear 2013; 34 (05) 535-552
- 9 ASHA. https://www.asha.org/public/speech/development/01/
- 10 Yoshinaga-Itano C, Sedey AL, Mason CA, Wiggin M, Chung W. Early Intervention, Parent Talk, and Pragmatic Language in Children With Hearing Loss. Pediatrics 2020; 146 (Suppl. 03) S270-S277
- 11 McConkey Robbins A, Koch DB, Osberger MJ, Zimmerman-Phillips S, Kishon-Rabin L. Effect of age at cochlear implantation on auditory skill development in infants and toddlers. Arch Otolaryngol Head Neck Surg 2004; 130 (05) 570-574
- 12 de Brito R, Bittencourt AG, Goffi-Gomez MV. et al. Cochlear implants and bacterial meningitis: A speech recognition study in paired samples. Int Arch Otorhinolaryngol 2013; 17 (01) 57-61
- 13 Moeller MP. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000; 106 (03) E43
- 14 Hoshino AC, Echegoyen A, Goffi-Gomez MV, Tsuji RK, Bento RF. Outcomes of Late Implantation in Usher Syndrome Patients. Int Arch Otorhinolaryngol 2017; 21 (02) 140-143
- 15 Lind-Combs HC, Holt RF. Associations Between Parent Mental State Language and Child Inhibitory Control in Children Who Are Deaf or Hard of Hearing. J Speech Lang Hear Res 2022; 65 (08) 3129-3145
- 16 Selleck AM, Park LR, Brown KD. Factors Influencing Pediatric Cochlear Implant Outcomes: Carolina Sibling Study. Otol Neurotol 2019; 40 (09) 1148-1152
- 17 Pianesi F, Scorpecci A, Giannantonio S, Micardi M, Resca A, Marsella P. Prelingual auditory-perceptual skills as indicators of initial oral language development in deaf children with cochlear implants. Int J Pediatr Otorhinolaryngol 2016; 82: 58-63
- 18 Silva-Comerlatto MP. Habilidades auditivas e de linguagem de crianças usuárias de implante coclear: análise dos marcadores clínicos de desenvolvimento. Tese (Doutorado). Available at https://teses.usp.br/teses/disponiveis/5/5143/tde-20052016-142644/pt-br.php
- 19 McConkey Robbins A. Monitoring Communication Progress in Early Intervention. IN: A Sound Foundation Through Early Amplification. Available at https://www.amymcconkeyrobbins.com/PDF/com_18_p61899_pho_kapitel_8.pdf
- 20 Eshraghi AA, Nazarian R, Telischi FF. et al. Cochlear Implantation in Children With Autism Spectrum Disorder. Otol Neurotol 2015; 36 (08) e121-e128
- 21 Nasralla HR, Montefusco AM, Hoshino ACH. et al. Benefit of Cochlear Implantation in Children with Multiple-handicaps: Parent's Perspective. Int Arch Otorhinolaryngol 2018; 22 (04) 415-427