

Subscribe to RSS
DOI: 10.1055/s-0043-1770078
Hyaluronic Acid Filler Injection Guided by Doppler Ultrasound
Authors
Abstract
Doppler ultrasound can be used to detect almost all arteries of the face before injecting the hyaluronic acid (HA) filler. The relatively more dangerous sites of filler injection are the glabellar wrinkle, forehead, temple, nose, and nasolabial fold area, and it is recommended to map the vasculature of these areas by Doppler ultrasound before performing filler injection. The Doppler ultrasound detection method is included as a video. Internal carotid arterial branches, the supratrochlear, supraorbital, and dorsal nasal arteries, and external carotid arterial branches, the superficial temporal and facial arteries, are very important arteries when injecting HA filler; thus, Doppler ultrasound detection is recommended.
Introduction
The use of soft tissue fillers is one of the most commonly used aesthetic procedures for facial rejuvenation.[1] Although filler injections are easy to perform, they have complications.[2] Vascular complications, such as skin necrosis and ocular complications, are the most serious complications of filler injections.[3] To avoid these, knowledge of facial anatomy is key. However, the vasculature varies between individuals, and injectors cannot locate all the vasculature during filler injection. Doppler ultrasound can detect vessels of the face by detecting the interaction of sound waves with tissue. Ultrasonography is a well-known and safe procedure that can be applied to minimally invasive procedures of the face.[4] Ultrasound examination can be used to map vasculature and detect the locations of previous fillers or fillers when vascular complications occur.[5] Recently, real-time ultrasound-guided filler techniques have been developed.[6] However, it is very difficult to perform real-time detection and filler injection concomitantly because of the number of hands needed, delicate filler injection procedures, and the possibility of infection. In this review article, we summarize previous studies on Doppler ultrasound detection of arteries of the face and hyaluronic acid (HA) filler injection to promote the implementation of safer procedures. All patients provided written informed consent for publication of photograph.
Ultrasound Wave Frequency
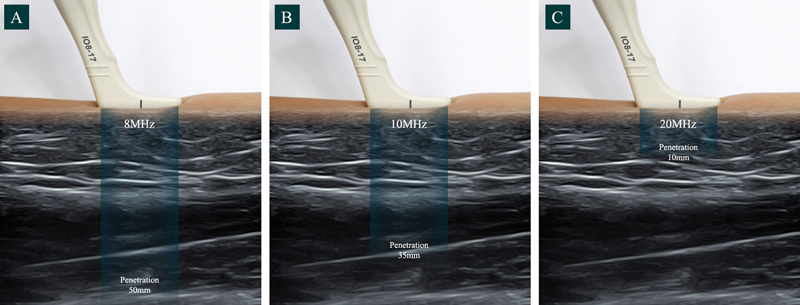
In our study, an 8 to 17 MHz hockey stick probe (E-cube, Alpinion Medical Systems Co., South Korea) was used. The use of 8 MHz provided a depth of visualization of approximately 50 mm, while 20 MHz, gives a depth of 10 mm ([Fig. 1]). Thus, 8 to 17 MHz probe can cover all the facial layer detection. Doppler ultrasound can detect both arteries and veins and distinguishes between them by the way blood circulation changes when the probe presses on the vessel. If blood circulation completely stops, the vessel is identified as a vein. If blood flow persists, it indicates an artery. Thus, artery and vein cannot be distinguished by color but distinguished by probe pressing.
Glabellar Wrinkle Correction
One of the dangerous areas for filler injection is the glabellar area where the supratrochlear artery is located, one of the most common sites for ocular complications.[7] In our previous study, 74 glabellar wrinkle lines were evaluated using Doppler ultrasound.[8] The supratrochlear artery was located lateral to the glabellar wrinkle lines in 44/74 (59%) cases. However, six supratrochlear arteries were located at the glabellar wrinkle line and in the subdermal layer ([Fig. 2]). In the case of this variation, it is extremely dangerous to inject HA filler at the glabellar wrinkle line.

To correct the glabellar wrinkle line, the Doppler ultrasound probe was positioned at the wrinkle line ([Fig. 3A]). The supratrochlear artery is identified and marked in red to show its position relative to the glabellar wrinkle lines ([Fig. 3B]). Considering the rheology in a previous article, Lorient No.2 (HA filler, G' 203 Pa, tan δ 0.2, Joonghun Pharmaceutical, Seoul, Korea) can be injected into the subdermal layer.[9]

Forehead Augmentation
The forehead is a wide area requiring an even injection of HA filler for better outcomes. The forehead area has an extensive network of blood vessels (the supratrochlear artery, supraorbital artery, and frontal branch of the superficial temporal artery; [Fig. 4]).[10]

Doppler ultrasound can be used to detect and mark the pathways of these arteries. However, as described in a previous article, the supraorbital artery can exhibit significant variations in its superficial branches and deep branches (18 and 64% of cases, respectively) when detected by Doppler ultrasound.[11] In our study also, the supraorbital artery was relatively difficult to detect. The frontal branch of the superficial temporal artery could be detected more easily in the temple area. After detection of the forehead arterial pathways, HA filler Lorient No.4 (G' 338, tan δ 0.28) was injected based on rheology[9] ([Fig. 5]).

Temple Augmentation
The temple area is composed of complex layers, including the skin, subcutaneous layer, superficial temporal fascia (STF), deep temporal fascia (DTF), and temporalis muscle and bone.[12] The authors recommend injecting HA filler between the STF and DTF. Our previous study showed good results when implementing these guidelines using Lorient No.4 (G' 338, tan δ 0.28, average 1.08 mL on each side).[13] All the procedures were performed after Doppler ultrasound detection ([Fig. 6]). The frontal branch of the superficial temporal artery is one of the main arteries located in the temple area and can be detected medially, inside, or at the hairline.[14]

Another recommendation for temple augmentation involves injecting HA filler into the deep layer, the pre-periosteal layer, by needle.[15] However, our previous study showed that there is a possibility of perforation of the superficial and deep temporal arteries.[16] Our sonographic findings showed that the anterior branch of the deep temporal artery could be interrupted when deeply injected into the temple area ([Fig. 7]). Therefore, ultrasound scanning prior to injection into the temple area is recommended.

Nose Augmentation
Nose augmentation by HA filler is one of the most commonly performed procedures, but it also carries its dangers. It is the most common area for ocular complications because the dorsal nasal artery is a branch of the internal carotid artery.[17] In a cadaveric study, arteries and veins were found to run above the fibromuscular layer, so injection at the supraperiosteal layer is determined to be a safe injection plane.[18] However, in our previous study, we showed that some arteries were detected by Doppler ultrasound at the supraperiosteal layer; thus, there was no completely safe layer for injection.[19] The dorsal nasal artery can be detected when the Doppler ultrasound probe is used at the midline of the nose ([Fig. 8]). The dorsal nasal artery tended to cross the midline of the nose.[20] Therefore, it is recommended to perform Doppler ultrasound before nose injection.

Nose augmentation using HA filler is usually performed using either a cannula or a needle. Our previous study showed that perpendicular injection at the radix area by needle could risk injection of filler into the dorsal nasal artery depending on the needle bevel location.[21] Therefore, cannula injection appears to be a relatively safe procedure. However, the use of a blunt-tip cannula still poses a potential risk. Previous studies have reported that ocular complications were induced by a 25G cannula and even a 23G cannula.[22] According to previous literature, it is relatively safe to perform Doppler ultrasound using a cannula, and gentle injection should be performed for nose augmentation with HA filler. In addition, it is recommended to inject the supraperiosteal layer with a high G' HA filler, such as Lorient No.6 (G' 413, tan δ 0.29).
Nasolabial Fold Correction
Nasolabial fold correction is one of the most common procedures to use filler injections. However, the facial artery runs near the nasolabial fold area and, due to the variation of arterial, can be located under or over muscles.[23] Our previous study showed that the facial artery pathway could be traversing the nasolabial fold area (69%) or lateral to the nasolabial fold area (31%).[24] Therefore, it is relatively safe to detect the facial artery location by Doppler ultrasound first, and then inject high G' HA fillers such as Lorient No.4 or 6 at the supraperiosteal layer ([Fig. 9]).

Other Locations for Doppler Ultrasound Detection
Doppler ultrasound can be applied when tear trough correction is performed using an HA filler. The angular artery runs on the medial side of the angular vein. However, the angular artery can vary when approaching the infraorbital artery.[25] The angular vein can be detected by Doppler ultrasound and is useful when injecting HA filler into the tear trough area, and deep injection is recommended.[26] The infraorbital artery can also be detected using Doppler ultrasound and is useful when performing midface augmentation. However, when augmentation of the lateral cheek area, it is relatively difficult to find the transverse facial artery by Doppler ultrasound. HA fillers can also be applied to lower face areas, such as for chin augmentation, lip augmentations, and marionette line correction. The superior and inferior labial arteries can be detected near the lower face area; however, since it is well known that the labial artery tends to run near the mucosal area, filler injection is relatively safe when injected into the vermilion borders of the lips.
Conclusion
Doppler ultrasound can be used to detect almost all arteries of the face before injecting the HA filler. The relatively more dangerous sites of filler injection are the glabellar wrinkle, forehead, temple, nose, and nasolabial fold area, and it is recommended to map the vasculature of these areas by Doppler ultrasound before performing filler injection. The Doppler ultrasound detection method is included as a video ([Video 1], available in the online version). Internal carotid arterial branches, the supratrochlear, supraorbital, and dorsal nasal arteries, and external carotid arterial branches, the superficial temporal and facial arteries, are very important arteries when injecting HA filler; thus, Doppler ultrasound detection is recommended.
Video 1
Conflict of Interest
None declared.
Acknowledgment
Authors would like to thank Won Lee was an investigator, speaker, and consultant for Joonghun Pharmaceutical, Seoul, South Korea.
Authors' Contributions
W.L. has made contribution to conceptualization, writing, and drafting. the author is in change of every section of the manuscript.
Ethical Approval
Since it is a Review, Ethical Approval was not required for this article.
Patient Consent
All photograph model provided written consent for publication.
-
References
- 1 The aesthetic society's cosmetic surgery national data bank: Statistics 2019. Aesthet Surg J 2020; 40 (1, suppl 1): 1-26
- 2 DeLorenzi C. Complications of injectable fillers, part I. Aesthet Surg J 2013; 33 (04) 561-575
- 3 DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J 2014; 34 (04) 584-600
- 4 Kim HJ, Youn KH, Kim JS, Kim YS, Hong SO, Na J. Ultrasonographic Anatomy of the Face and Neck for Minimally Invasive Procedures: An Anatomic Guideline for Ultrasonographic-Guided Procedures. Singapore: Springer Nature; 2020
- 5 Schelke LW, Decates TS, Velthuis PJ. Ultrasound to improve the safety of hyaluronic acid filler treatments. J Cosmet Dermatol 2018; 17 (06) 1019-1024
- 6 Rocha PS, Guerra TA, Teixeira DA. Description of a safe Doppler ultrasound-guided technique for hyaluronic acid filler in the face-a method to avoid adverse vascular events. J Cosmet Dermatol 2022; 21 (07) 2783-2787
- 7 Beleznay K, Carruthers JD, Humphrey S, Jones D. Avoiding and treating blindness from fillers: a review of the world literature. Dermatol Surg 2015; 41 (10) 1097-1117
- 8 Lee W, Moon HJ, Kim JS, Yang EJ. Safe glabellar wrinkle correction with soft tissue filler using Doppler ultrasound. Aesthet Surg J 2021; 41 (09) 1081-1089
- 9 Lee W. Five factors to consider before treatment of a hyaluronic acid filler-induced vascular complications. Arch Plast Surg 2022; 49 (04) 479-481
- 10 Cong LY, Phothong W, Lee SH. et al. Topographic analysis of the supratrochlear artery and the supraorbital artery: implication for improving the safety of forehead augmentation. Plast Reconstr Surg 2017; 139 (03) 620e-627e
- 11 Phumyoo T, Jiirasutat N, Jitaree B, Rungsawang C, Pratoomthai B, Tansatit T. Localization and topography of the arteries on the middle forehead region for eluding complications following forehead augmentation: conventional cadaveric dissection and ultrasonography investigation. J Craniofac Surg 2020; 31 (07) 2029-2035
- 12 Davidge KM, van Furth WR, Agur A, Cusimano M. Naming the soft tissue layers of the temporoparietal region: unifying anatomic terminology across surgical disciplines. Neurosurgery 2010; 67 (3, Suppl Operative): ons120-ons129 , discussion ons129–ons130
- 13 Lee W, Park JW, Yang EJ. Temple augmentation by injecting a hyaluronic acid filler between the superficial and deep temporal fasciae. J Cosmet Dermatol 2022; 21 (10) 4313-4318
- 14 Lee W, Moon HJ, Kim JS, Chan BL, Yang EJ. Doppler ultrasound-guided thread lifting. J Cosmet Dermatol 2020; 19 (08) 1921-1927
- 15 Swift A. One up, one over regional approach in upper face: anatomy and regional approaches to injectables” found in the November 2015 supplement issue soft tissue fillers and neuromodulators: international and multidisciplinary perspectives. Plast Reconstr Surg 2015; 136: S204-S218
- 16 Lee W, Moon HJ, Kim MS, Cheon GW, Yang EJ. Pre-injection ultrasound scanning for treating temporal hollowing. J Cosmet Dermatol 2022; 21 (06) 2420-2425
- 17 Beleznay K, Carruthers JDA, Humphrey S, Carruthers A, Jones D. Update on avoiding and treating blindness from fillers: a recent review of the world literature. Aesthet Surg J 2019; 39 (06) 662-674
- 18 Moon HJ. Injection rhinoplasty using filler. Facial Plast Surg Clin North Am 2018; 26 (03) 323-330
- 19 Lee W, Kim JS, Oh W, Koh IS, Yang EJ. Nasal dorsum augmentation using soft tissue filler injection. J Cosmet Dermatol 2019; 18 (05) 1254-1260
- 20 Choi DY, Bae JH, Youn KH. et al. Topography of the dorsal nasal artery and its clinical implications for augmentation of the dorsum of the nose. J Cosmet Dermatol 2018; 17 (04) 637-642
- 21 Moon HJ, Lee W, Do Kim H, Lee IH, Kim SW. Doppler ultrasonographic anatomy of the midline nasal dorsum. Aesthetic Plast Surg 2021; 45 (03) 1178-1183
- 22 Thanasarnaksorn W, Cotofana S, Rudolph C, Kraisak P, Chanasumon N, Suwanchinda A. Severe vision loss caused by cosmetic filler augmentation: case series with review of cause and therapy. J Cosmet Dermatol 2018; 17 (05) 712-718
- 23 Lee JG, Yang HM, Choi YJ. et al. Facial arterial depth and relationship with the facial musculature layer. Plast Reconstr Surg 2015; 135 (02) 437-444
- 24 Lee W, Kim JS, Moon HJ, Yang EJ. A safe Doppler ultrasound-guided method for nasolabial fold correction with hyaluronic acid filler. Aesthet Surg J 2021; 41 (06) NP486-NP492
- 25 Kim YS, Choi DY, Gil YC, Hu KS, Tansatit T, Kim HJ. The anatomical origin and course of the angular artery regarding its clinical implications. Dermatol Surg 2014; 40 (10) 1070-1076
- 26 Calomeni M, Alfertshofer MG, Frank K. et al. Real-time ultrasound imaging of the tear trough: lessons learned from functional anatomy. Aesthet Surg J 2022; 42 (05) 518-526
Address for correspondence
Publication History
Received: 03 September 2022
Accepted: 24 March 2023
Article published online:
02 August 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 The aesthetic society's cosmetic surgery national data bank: Statistics 2019. Aesthet Surg J 2020; 40 (1, suppl 1): 1-26
- 2 DeLorenzi C. Complications of injectable fillers, part I. Aesthet Surg J 2013; 33 (04) 561-575
- 3 DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J 2014; 34 (04) 584-600
- 4 Kim HJ, Youn KH, Kim JS, Kim YS, Hong SO, Na J. Ultrasonographic Anatomy of the Face and Neck for Minimally Invasive Procedures: An Anatomic Guideline for Ultrasonographic-Guided Procedures. Singapore: Springer Nature; 2020
- 5 Schelke LW, Decates TS, Velthuis PJ. Ultrasound to improve the safety of hyaluronic acid filler treatments. J Cosmet Dermatol 2018; 17 (06) 1019-1024
- 6 Rocha PS, Guerra TA, Teixeira DA. Description of a safe Doppler ultrasound-guided technique for hyaluronic acid filler in the face-a method to avoid adverse vascular events. J Cosmet Dermatol 2022; 21 (07) 2783-2787
- 7 Beleznay K, Carruthers JD, Humphrey S, Jones D. Avoiding and treating blindness from fillers: a review of the world literature. Dermatol Surg 2015; 41 (10) 1097-1117
- 8 Lee W, Moon HJ, Kim JS, Yang EJ. Safe glabellar wrinkle correction with soft tissue filler using Doppler ultrasound. Aesthet Surg J 2021; 41 (09) 1081-1089
- 9 Lee W. Five factors to consider before treatment of a hyaluronic acid filler-induced vascular complications. Arch Plast Surg 2022; 49 (04) 479-481
- 10 Cong LY, Phothong W, Lee SH. et al. Topographic analysis of the supratrochlear artery and the supraorbital artery: implication for improving the safety of forehead augmentation. Plast Reconstr Surg 2017; 139 (03) 620e-627e
- 11 Phumyoo T, Jiirasutat N, Jitaree B, Rungsawang C, Pratoomthai B, Tansatit T. Localization and topography of the arteries on the middle forehead region for eluding complications following forehead augmentation: conventional cadaveric dissection and ultrasonography investigation. J Craniofac Surg 2020; 31 (07) 2029-2035
- 12 Davidge KM, van Furth WR, Agur A, Cusimano M. Naming the soft tissue layers of the temporoparietal region: unifying anatomic terminology across surgical disciplines. Neurosurgery 2010; 67 (3, Suppl Operative): ons120-ons129 , discussion ons129–ons130
- 13 Lee W, Park JW, Yang EJ. Temple augmentation by injecting a hyaluronic acid filler between the superficial and deep temporal fasciae. J Cosmet Dermatol 2022; 21 (10) 4313-4318
- 14 Lee W, Moon HJ, Kim JS, Chan BL, Yang EJ. Doppler ultrasound-guided thread lifting. J Cosmet Dermatol 2020; 19 (08) 1921-1927
- 15 Swift A. One up, one over regional approach in upper face: anatomy and regional approaches to injectables” found in the November 2015 supplement issue soft tissue fillers and neuromodulators: international and multidisciplinary perspectives. Plast Reconstr Surg 2015; 136: S204-S218
- 16 Lee W, Moon HJ, Kim MS, Cheon GW, Yang EJ. Pre-injection ultrasound scanning for treating temporal hollowing. J Cosmet Dermatol 2022; 21 (06) 2420-2425
- 17 Beleznay K, Carruthers JDA, Humphrey S, Carruthers A, Jones D. Update on avoiding and treating blindness from fillers: a recent review of the world literature. Aesthet Surg J 2019; 39 (06) 662-674
- 18 Moon HJ. Injection rhinoplasty using filler. Facial Plast Surg Clin North Am 2018; 26 (03) 323-330
- 19 Lee W, Kim JS, Oh W, Koh IS, Yang EJ. Nasal dorsum augmentation using soft tissue filler injection. J Cosmet Dermatol 2019; 18 (05) 1254-1260
- 20 Choi DY, Bae JH, Youn KH. et al. Topography of the dorsal nasal artery and its clinical implications for augmentation of the dorsum of the nose. J Cosmet Dermatol 2018; 17 (04) 637-642
- 21 Moon HJ, Lee W, Do Kim H, Lee IH, Kim SW. Doppler ultrasonographic anatomy of the midline nasal dorsum. Aesthetic Plast Surg 2021; 45 (03) 1178-1183
- 22 Thanasarnaksorn W, Cotofana S, Rudolph C, Kraisak P, Chanasumon N, Suwanchinda A. Severe vision loss caused by cosmetic filler augmentation: case series with review of cause and therapy. J Cosmet Dermatol 2018; 17 (05) 712-718
- 23 Lee JG, Yang HM, Choi YJ. et al. Facial arterial depth and relationship with the facial musculature layer. Plast Reconstr Surg 2015; 135 (02) 437-444
- 24 Lee W, Kim JS, Moon HJ, Yang EJ. A safe Doppler ultrasound-guided method for nasolabial fold correction with hyaluronic acid filler. Aesthet Surg J 2021; 41 (06) NP486-NP492
- 25 Kim YS, Choi DY, Gil YC, Hu KS, Tansatit T, Kim HJ. The anatomical origin and course of the angular artery regarding its clinical implications. Dermatol Surg 2014; 40 (10) 1070-1076
- 26 Calomeni M, Alfertshofer MG, Frank K. et al. Real-time ultrasound imaging of the tear trough: lessons learned from functional anatomy. Aesthet Surg J 2022; 42 (05) 518-526