

Subscribe to RSS
DOI: 10.1055/s-0043-1774301
Spontaneous Intracranial Hypotension: A Review of Neuroimaging and Current Concepts
Authors
Funding None.


Abstract
Spontaneous intracranial hypotension (SICH) is the emerging cause of orthostatic headache as it has been better recognized in recent years. SICH happens due to spinal cerebrospinal fluid (CSF) leak; however, the manifestations are predominantly cranial and hence imaging in SICH includes brain and spine. There are few characteristic brain imaging features to be concerned about to diagnose SICH in patients with vague symptoms or low clinical suspicion. Spine screening is recommended in these patients to assess spinal CSF leaks. While neuroradiologists play a significant role from the time of diagnosis to treatment of SICH, there is a need for all the general radiologists to be aware of the condition. Computed tomography myelogram and digital subtraction myelogram are performed for diagnostic and therapeutic management of SICH. There is a known risk for SICH recurrence in patients with sagittal longitudinal epidural collection and hence, targeted blood patch should be used instead of blind patch. Most importantly, slow mobilization is recommended following the patch to avoid recurrence.
Introduction
Spontaneous intracranial hypotension (SICH) is a clinical condition resulting from reduced intracranial pressure that causes imbalances between the blood, cerebrospinal fluid (CSF), and the brain parenchyma. This occurs more commonly secondary to spinal CSF leak into the epidural space or to adjacent venous channels. Even though the name suggests intracranial hypotension, hypotension is not always demonstrated on lumbar puncture and the CSF leak at the skull base rarely results in intracranial hypotension and hence it should be renamed as spontaneous spinal CSF leak syndrome. SICH can also be termed as CSF hypovolemia, CSF volume depletion, and low CSF volume headache. Spinal CSF leaks are increasingly recognized in recent times due to improved imaging techniques and detection with increasing awareness.
The pathophysiology is understood by Monro-Kellie doctrine where the volume of CSF, blood, and brain parenchyma remains constant in dynamic equilibrium. For instance, in patients with CSF leak, there is reduction in the CSF volume, which results in compensatory dilatation or engorgement of the intracranial and epidural venous structures to maintain the intracranial pressure causing clinical symptoms accordingly ([Chart 1]). Buoyancy of the brain is also reduced in leak patients.[1] Reduced CSF in the brain causes stretching of the pain sensitive meningeal structures and subsequent venous engorgement results in headache.
The knowledge of physiology of normal intracranial pressure is necessary to understand the mechanism of hypotension in SICH .
patients. There are two points of neuroaxis that play major roles in maintaining the equilibrium. These include hydrostatic indifference point (HIP) and zero CSF pressure in sitting (ZPS). HIP is a point located in the lower cervical or upper thoracic region spinal region, corresponding with the venous pressure at atmospheric level. At this level, the pressure recorded in sitting and lying down position is same. ZPS is located between occipital protuberance and spinous process of seventh cervical vertebra. CSF pressure is negative above ZPS level and positive below this level.
The physiology of orthostatic headache in SICH is that when the person is upright, the CSF pressure is more than the atmospheric pressure. In patients with spinal CSF leaks, pressure point moves downwards, resulting in negative intracranial pressure compared to the spine. However, on lying down, headache resolves on lying down as the pressure attains equilibrium with the point coming back to the normal position.[2] [3] This is the same reason why skull base leaks do not result in symptoms of SICH.
Clinical Features
SICH is the one of the most important and under diagnosed causes of daily disabling headache with an incidence of 1 in 50000. Underdiagnosis of SICH has led to chronic neurodisabilities despite being a treatable condition. Females are more commonly affected than men. Headache in SICH worsen over the second half of the day and may also worsen during Valsalva maneuver. Predisposing factors include connective tissue disorders causing meningeal disruption, discal spur, and marginal osteophyte.
SICH is an elusive disorder and can mimic many other conditions. The commonest clinical presentation is orthostatic headache, which aggravates against sitting or standing and relieved on lying down. In rare and severe cases, patient may present with dementia, symptoms of brain and/ or spinal cord herniation.[4] [5] [Table 1] summarizes the symptoms or presentations of SICH.
Abbreviations: CVT, cortical vein thrombosis; PRES, posterior reversible encephalopathy syndrome; SDH, subdural hematoma; SICH, spontaneous intracranial hypotension.
Differential diagnoses include orthostatic hypotension, cervicogenic headache, postural tachycardia syndrome, and migraine.[5] However, typical history and clinical examination would rule out other causes.
There are few imaging and clinical findings that form the diagnostic criteria for SICH, and these include [Table 2].[6] [7] [8] [9]
Abbreviations: CSF, cerebrospinal fluid; SICH, spontaneous intracranial hypotension.
As SICH is caused by CSF leaks in the spine, three types of leaks are described accordingly depending on the site of leak and whether epidural collection is present or not ([Table 3]).[8] [10] [11]
|
Type 1 |
Dural tear: SLEC positive 1A—Ventral tear 1B—Lateral tear |
|
Type 2A |
SLEC positive—proximal nerve root sleeve tear/ meningeal diverticular/ dural ectasia |
|
Type 2B |
SLEC negative—distal nerve root sleeve tear |
|
Type 3 |
CSF venous fistula (CVF) |
Abbreviations: CSF, cerebrospinal fluid; CVF, CSF venous fistula; SLEC, spinal longitudinal epidural collection.
Leaks can be categorized as fast or slow leaks. Fast leaks are seen following ventral dural tear. Slow leaks occur in nerve root sleeve tear and CSF venous fistula (CVF). Tears in the dura can occur ventrally or laterally. An osteophyte or degenerative disc microspur causes anterior longitudinal tears in the spinal dura and is more commonly seen at upper thoracic levels due to minimal flexibility of the spine along this region, although lower cervical and lumbar dural tears have also been reported. In type 1 spinal leak, there will be epidural collection due to the ventral dural defect that is associated with a discal spur or an osteophyte at the site of leak. It occurs frequently in middle aged females with lesser or normal resting metabolic rate, although the incidence in men is not very uncommon in recent times.[10] [12] Type 2 leaks are classified further as spinal longitudinal epidural collection positive (SLEC-P) which means there is definite spinal longitudinal epidural collection and SLEC negative (SLEC-N) where there is no epidural collection. SLEC-P type 2A leaks occur due to lateral dural tear wherein nerve root sleeve tear occurs proximally with positive SLEC. Other examples are the ruptured meningeal diverticulum and absent nerve root sleeve. These occur between the epidural space and neural foraminal compartment, resulting in definite epidural CSF collection. Meningeal diverticula are frequently seen in patients with connective tissue disorders like Marfan syndrome, neurofibromatosis, and Ehlers–Danlos syndrome. In type 2B SLEC-N leak, far lateral dural tear or nerve root sleeve tear occurs distally and CSF leaks into the adjacent fascia or connective tissue without any epidural collection. In type 3 leak, the CSF enters directly into the venous channels and hence no epidural collection (SLEC-N).[9] CVFs are more commonly seen along the lower thoracic spine and in elderly.[12] They may be associated with meningeal diverticulum that is seen as perineural cyst. Such cysts may give rise to CVFs acting as a nidus. CVFs lack dural defect and are seen near nerve root sleeve diverticula close to paraspinal veins.[13]
Other or secondary causes of spinal CSF leaks include injuries to the dura mater following lumbar puncture, spinal anesthesia or surgeries, trauma, and post-ventriculoperitoneal shunt of which post-lumbar puncture intracranial hypotension is more common than other causes.[14] The dural defect is posterior and lumbar in location in these causes as compared to anterior or lateral in SICH, but the pathophysiology is the same regardless of the cause. Post-dural puncture headache may appear as new daily onset headache after many years of prior dural puncture. There can be an arachnoid bleb formation at the puncture site. Use of atraumatic or pencil point needles over cutting edge needles during lumbar puncture would reduce many complications including post-dural puncture headaches.[15] [16]
Imaging Features
There are few characteristic brain and spine imaging features that suggest intracranial hypotension. Magnetic resonance imaging (MRI) including brain and spine with contrast is the imaging investigation of choice where SICH is suspected clinically due to the clinical symptoms. Computed tomography (CT) brain is not recommended as the temporal resolution is lesser than MRI. However, in few cases, where there is no clinical suspicion of SICH, CT may be the initial imaging modality by the clinicians to look for any cause of headache. CT of the whole spine is important to detect the osteophyte or the discal spur that may be the cause of SLEC-P SICH as CT is sensitive for any bone pathology and serves as complimentary imaging to MRI study. Brain findings remain the same for all cases of intracranial hypotension regardless the cause.
A description of the MRI protocol is given in [Table 4], which includes brain and spine sequences.[9]
Abbreviations: 3D, three-dimensional; CISS, constructive interference in steady state; CVST, cerebral venous sinus thrombosis; FIESTA, fast imaging employing steady state acquisition; MRI, magnetic resonance imaging; SICH, spontaneous intracranial hypotension; SWI, sagittal-weighted imaging; T1W, T1-weighted.
Below are the distinctive intracranial and spine imaging characteristics.
Intracranial Findings (SEEPS)
-
Subdural collection (bilateral)
-
Enhancement of the pachymeninges
-
Engorgement of dural venous sinuses
-
Paucity of bilateral perioptic CSF
-
Pituitary hyperemia
-
Sagging of the brain
-
Superficial siderosis
The initial imaging finding is the venous sinus engorgement or distension that is easily detected in the transverse and straight sinuses. These sinuses have flattened or concave borders normally. The concave border of the transverse sinus is seen on sagittal images. In patients with intracranial hypotension, the venous sinus borders appear bulged and convex.[17] Pachymeningeal thickening with enhancement is the next imaging feature to appear. The thickening is smooth/non-nodular and requires contrast imaging to be appreciated. This is due to the noninflammatory fibrocollagenous proliferation of the meninges because of persistent vascular engorgement and transudation of intravascular fluid into the adjacent subdural space. On further progression/persistence of the CSF leak, to maintain the volume within the intracranial space, subdural collection occurs secondary to passive transudation from the intravascular space into the subdural space. The collection may be hemorrhagic in nature but always bilateral and more commonly seen along the frontoparietal convexities.[14] Among these signs, venous distension is very specific to diagnose low intracranial pressure. Pituitary engorgement is another important imaging sign where it enlarges up to 8 to 11 mm in height. However, while recovering, it reverses sooner than pachymeningeal enhancement. Another important finding is sagging of the brain secondary to loss of buoyancy of the brain. This is seen on imaging as down sloping of the floor of third ventricle, mamillary body descent, and effaced basal cisternal spaces. Reduced perioptic CSF fluid is another imaging finding that supports the diagnosis of intracranial hypotension. All these findings reverse back to normal following treatment ([Fig. 2A–H]). [Fig. 3] illustrates other miscellaneous imaging features. All the findings are detected on MRI. CT is not very sensitive to detect these findings other than subdural collection. CT may also show pseudosubarachnoid hemorrhage when there is brain sagging and effaced cisternal spaces.



The probability of CSF leak is assessed using Bern scoring system as low, intermediate, and high with scores of 2 or less, 3 to 4, 5 and more, respectively. This system includes only intracranial findings and does not consider SLEC. Bern scoring system is as follows[9] ([Table 5]).
Abbreviation: SICH, spontaneous intracranial hypotension.
Spine Findings
-
Epidural collection (anterior / posterior)
-
Dural defect
-
Meningeal diverticulum/ Perineural cyst
-
Engorged vertebral venous plexus/epidural veins
-
Spinal cord signal intensity changes
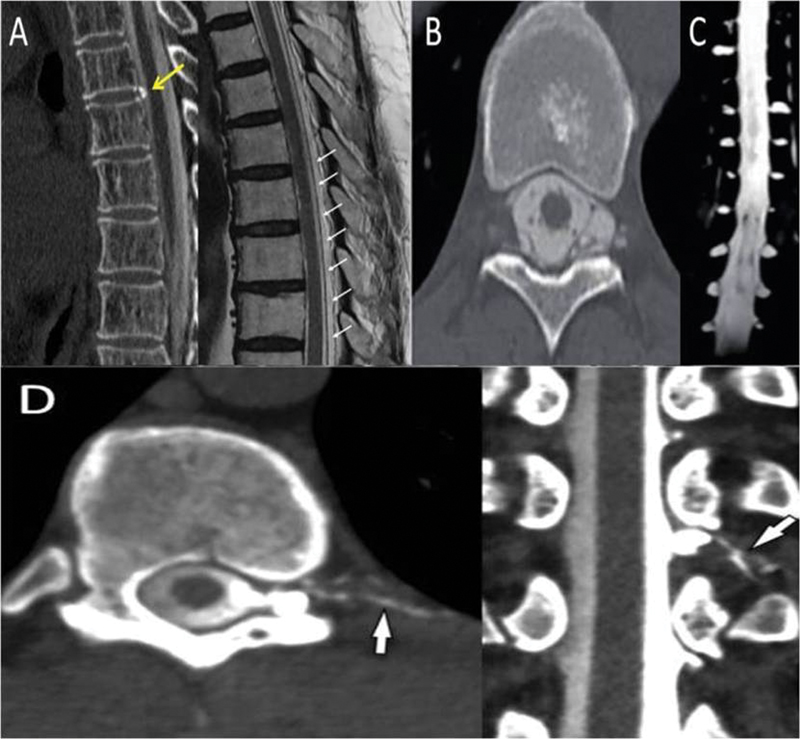
Out of all the sequences, T2 is the most useful sequence to rule out SLEC and if present is termed as SLEC-P SICH. SICH can also present without SLEC and is termed as SLEC-N SICH. These SLEC-P SICH are fast leakers that are seen in type 1 and type 2 leaks. Type 3 that includes CVF is a slow leaker without SLEC. The resolution of three-dimensional heavily T2-weighted imaging may help in detecting the site of the dural tear in fast leakers. However, MRI spine has limited outcome in patients with CVF as the fistula is not seen in this modality. In a patient with high clinical suspicion of intracranial hypotension without any brain or spine imaging features, CVF needs to be ruled out. Further investigation of choice is digital subtraction myelography (DSM). Plain CT scan of the whole spine is to be very useful in detecting the discal spur or osteophyte responsible for the spinal leak ([Figs. 4] and [5]).

Patients with secondary causes of hypotension have similar intracranial imaging findings and spine imaging findings include spinal epidural collection at the site of defect depending on the respective causes.
Chronic SICH
Chronic complications/ findings in untreated patients of SICH include ([Fig. 6]):

-
Superficial siderosis is commonly seen in posterior fossa involving superior cerebellar foliae and occurs due to bleeding from the friable epidural veins at the site of dural tear.[9]
-
Bibrachial amyotrophy. This feature is seen in chronic SLEC-P patients as the collection compresses the anterior horn cells of the spinal cord and stretches the cervical nerve roots resulting in atrophy.[18] [19]
-
The longitudinal spinal collection appears more loculated with rounded margins and with or without thin septations like pseudomeningocele.
-
Calvarial thickening with/without prominent transosseous venous collaterals. Thickening of the calvarium in SICH is a compensatory mechanism for the depleted CSF volume. Typically, the thickening occurs along the inner table, more so involving the frontal bone, giving rise to an appearance of layer cake skull.[20]
Uncommon Findings in SICH[21]
-
Ischemia is secondary to brain herniation.
-
Venous sinus thrombosis due to venous engorgement and stasis.
-
Spinal subarachnoid hemorrhage and hemosiderosis.
-
Dural calcifications may occur sequelae to chronic blood product deposition secondary to repeated hemorrhage from the epidural venous plexus.
Mimics of SICH[22]
-
Arnold Chiari 1 malformation
-
Other causes of subdural collection
-
Other causes of pachymeningeal thickening
-
Postural orthostatic tachycardia syndrome (POTS)
-
Migraine
Arnold Chiari 1 is a very close mimicker of SICH. Few characteristic imaging findings distinguish between the two and the differences are summarized in [Table 6].
Abbreviations: SDH, subdural hematoma; SICH, spontaneous intracranial hypotension.
Other causes of subdural collection may include trauma, bridging vein rupture in elderly following minor trauma. However, these are frequently on one side and rarely bilateral unlike SICH that is always bilateral. Pachymeningeal thickening can also be seen in other conditions like IgG4-related disease, neurosarcoidosis, histiocytosis, other autoimmune conditions, and infections including tuberculosis. In these conditions, other sites, which include brain parenchyma, cranial nerves, and bone may also be affected. In intracranial hypotension, the pachymeningeal thickening is smooth and non-nodular.[24]
Clinically, few conditions mimic SICH and these are POTS, vestibular migraine, orthostatic hypotension, and cervicogenic headache. POTS patients also develop headache worsening in standing or upright position. Heart rate and blood pressure while sitting and standing would help in diagnosing POTS as these patients typically have rapid increase in heart rate on standing with relatively stable blood pressure. Cervicogenic headache is due to osteoarthritic changes of the cervical spine. Vestibular migraine is diagnosed by the presence of associated vertigo.[22]
Further Managing SICH
Dynamic CT myelogram (CTM) or DSM performed to confirm spinal leak. Both the techniques involve expertise and radiation exposure. Myelogram confirms the site of dural tear, detection of meningeal diverticulum and CVF. Both the techniques are invasive in nature.
Ultrafast CT Myelography Technique
Patient is positioned in prone Trendelenburg position. By using the lumbar puncture technique, 10 mL of 300mg I/mL iodinated contrast is injected into the thecal sac and real time serial images are taken while injecting the contrast. Back and forth table movement in the CT gantry is accompanied by image acquisition every 10 to 20 seconds. In case of SLEC-N leaks, lateral decubitus position is suitable, although CTM may be negative in CVF and hence DSM is used.[23] In the event of contrast extravasation into the epidural space, the procedure must be stopped.[14] In fast leakers, the contrast enters the epidural space. If the imaging is quickly performed, the site of leak can be readily detected. In case of CVFs, CTM may show prominent paraspinal vein with adjacent small foraminal radicular veins.
Digital Subtraction Myelogram
It has greater temporal resolution than convention techniques, but limited coverage as DSM makes use of planar images.[25] Lateral decubitus position is preferred to demonstrate CVFs. A newer technique has been recently described for better appreciation of CVF. It is a two-day procedure carried out with right lateral decubitus on day 1 and repeating the same in left lateral decubitus on the day 2. To increase the sensitivity of detection of CVF in DSM, few modifications are suggested including respiratory modulation. It is based on the principle of changes in venous pressure secondary to changes in the intrathoracic pressure during different phases of respiration. This technique involves breathing continuously into a 5 mL syringe between the lips and image acquisition during breathing into the syringe and finally during Valsalva maneuver. There is disappearance of the prominent paraspinal vein and appearance of a prominent external epidural vein during Valsalva.
On CTM, false localizing sign has been described. This sign depicts retrospinal fluid collections at C1-C2 level in patients with intracranial hypotension that occurs as the epidural fluid escapes into the retrospinal soft tissues.[27] [28]
Treatment

Conservative Approach
Hydration and absolute bed rest may be tried but do not respond in many cases. Oral caffeine and abdominal binders may be tried but not at the expense of other definitive management ([Fig. 7]).
Epidural blood patch (EBP) can be given empirically or targeted. This is done following no more than 2 weeks of conservative management by performing CTM. Conventional CTM is not useful in fast leakers especially those with type 1 SICH and requires ultrafast dynamic CTM (UFCTM). As part of the radiological intervention for SLEC-P cases, UFCTM is performed to localize the rent followed by 8 to 10 mL of autologous EBP mixed with approximately 1 mL of iodinated contrast into the epidural space. EBP is targeted at either the localized site or empirically if unsuccessful to locate the exact site of leak. However, for all blind patches, lumbar region is used. Image-guided targeted EBP is recommended over blind EBP. Fibrin glue maybe used instead of blood, only in failed EBP cases or as the initial treatment if the treating doctor has experience or expertise in using fibrin glue. Post-EBP instructions are to be followed to prevent recurrence. Strict bed rest for at least 8 hours after blood patch. Immediate sitting upright post EBP, long hours of travelling or lifting heavy weights and performing maneuvers which tend to increase the intra-abdominal pressure are to be avoided for few days following the patch as these activities may increase the chance of recurrence. Recommended follow-up after blood patch is between 10 and 14 days and late follow-up is between 3 and 6 months. In case of recurrence in clinical symptoms, multidisciplinary meet is performed, and repeat imaging or intervention may be considered.[3]
-
Repeat EBPs recommended for recurrent cases. Image-guided targeted EBP is recommended over empirical patches. CT-guided epidural fibrin glue patches may also be tried for failed EBP cases.
-
CT-guided fibrin glue injection to meningeal diverticula and CVF.
-
CT-guided epidural fibrin glue injection or transvenous endovascular embolization of foraminal veins using liquid embolic agents for CVF.
-
Neurosurgical role
-
- Subdural collections evacuation for causing significant mass effect or midline shift.
-
- Dural repair and excision of the bony spurs or microspecies.
-
- Microsurgical repair of the dura and ligation of foraminal vein in cases of CVF and ligation repair of meningeal diverticulum.
-
Intrathecal Gadolinium MR Myelogram Remains Obsolete
Nuclear medicine cisternography used in patients with image-negative SICH. Lumbar puncture radionuclide tracer is injected. After 24 hours, complete coverage of cerebral convexity is obtained. In case of incomplete coverage after 24 hours, CSF flow dynamics are affected, and these are considered as SICH-positive cases and are subjected to DSM/CTM to assess possible SLEC-N leak.[29]
Anticoagulation in Case of Cerebral Venous Thrombosis
At places where there is no expertise to perform the UFCTM or DSM, two level nontargeted autologous blood patch is preferred, one at the cervicothoracic junction and the other at dorsolumbar junction, respectively.
Rebound Intracranial Hypertension
SICH may result in rebound intracranial hypertension following EBP or surgical repair, where the patient presents with headache worsening on lying down and improves in upright position. This is more commonly seen in patients with chronic SICH and is believed to be caused by increased CSF production and disrupted CSF reabsorption during the CSF leak period. It is treated by head end elevation and analgesics in mild cases, acetazolamide orally or intravenously in moderate cases, and lumbar puncture to remove the fluid in severely affected cases.[30]
Post-Treatment Imaging
Imaging findings are temporary and revert to normal. Intracranial features of venous distension, pituitary engorgement, herniation, and pachymeningeal enhancement disappear within a month following treatment. However, bilateral subdural collection may take a few more weeks to resolve.
Conclusion
SICH is an emerging elusive neurological condition, with an increase in incidence in recent years due to improved detection techniques and increasing awareness. The flowchart ([Fig. 8]) summarizes the steps need to be undertaken from the time of suspicion of diagnosis followed by the management. The knowledge of imaging findings of SICH is to be made aware among all the general radiologists that can further improve in detecting and treating this condition. MRI brain with contrast and screening the whole spine would give the radiologist a clue regarding spinal CSF leak. Utilizing appropriate diagnostic techniques is the key to confirming the diagnosis. Targeted EBP is the preferred first line of the treatment at present and use of CT guidance for injecting blood and fibrin glue is on the rise. In case of failure, repeat patches can be given and may consider alternative treatment strategies especially surgical repairs. However, the key success in SICH treatment is targeted image-guided blood patch and following strict post-procedure instructions.


Conflict of Interest
None declared.
Acknowledgment
We would like to thank Dr. Harshith Kramadhari, Assistant professor in Department of Radiodiagnosis at Kasturba Medical College, Manipal for his contribution to the artistic medical images of types of SICH
Learning Points
1. Headache with postural nature is an important symptom.
2. Imaging in SICH should include both brain and spine.
3. Negative imaging does not rule out SICH. High index of suspicion is necessary as it can mimic many conditions, ranging from Arnold Chiari I to amyotrophic lateral sclerosis.
4. Dynamic myelogram is preferred over conventional myelogram.
5. Multimodality treatment is available at present.
-
References
- 1 Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology 2001; 56 (12) 1746-1748
- 2 Robblee J, Secora KA, Alhilali LM, Knievel KL. Spontaneous Intracranial Hypotension Requires a High Index of Suspicion Because of Potentially Normal Diagnostic Test Results and Refractory Symptoms. Practical Neurology 2020
- 3 Sun-Edelstein C, Lay CL. Spontaneous intracranial hypotension: pathophysiology, clinical features, and diagnosis. UpToDate 2022
- 4 Headache classification committee of the international headache society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia 2018; 38 (01) 1-211
- 5 Cheema S, Anderson J, Angus-Leppan H. et al. Multidisciplinary consensus guideline for the diagnosis and management of spontaneous intracranial hypotension. J Neurol Neurosurg Psychiatry 2023
- 6 Urbach H, Fung C, Dovi-Akue P, Lützen N, Beck J. Spontaneous intracranial hypotension. Dtsch Arztebl Int 2020; 117 (27-28): 480-487
- 7 Kim D, Small JE. Intracranial Hypotension. In Small JE, Noujaim DL, Ginat DT, Kelly HR, Schaefer PW. (Ed), Neuroradiology. Elsevier; 2019: 158-162 . Doi: https://doi.org/10.1016/B978-0-323-44549-8.00017-1
- 8 Kranz PG, Gray L, Malinzak MD, Amrhein TJ. Spontaneous intracranial hypotension: pathogenesis, diagnosis, and treatment. Neuroimaging Clin N Am 2019; 29 (04) 581-594
- 9 Carlton Jones L, Butteriss D, Scoffings D. Spontaneous intracranial hypotension: the role of radiology in diagnosis and management. Clin Radiol 2022; 77 (03) e181-e194
- 10 Farb RI, Nicholson PJ, Peng PW. et al. Spontaneous intracranial hypotension: a systematic imaging approach for CSF leak localization and management based on MRI and digital subtraction myelography. Am J Neuroradiol 2019; 40 (04) 745-753
- 11 Luetzen N, Dovi-Akue P, Fung C, Beck J, Urbach H. Spontaneous intracranial hypotension: diagnostic and therapeutic workup. Neuroradiology 2021; 63 (11) 1765-1772
- 12 Mamlouk MD, Shen PY, Jun P, Sedrak MF. Spontaneous spinal CSF leaks stratified by age, body mass index, and spinal level. Am J Neuroradiol 2022; 43 (07) 1068-1072
- 13 Callen AL, Timpone VM, Schwertner A. et al. Algorithmic multimodality approach to diagnosis and treatment of spinal CSF leak and venous fistula in patients with spontaneous intracranial hypotension. Am J Roentgenol 2022; 219 (02) 292-301
- 14 Michali-Stolarska M, Bladowska J, Stolarski M, Sąsiadek MJ. Diagnostic imaging and clinical features of intracranial hypotension – review of literature. Pol J Radiol 2017; 82: 842-849
- 15 Callen AL, Lennarson P, Carroll IR. A causative role for remote dural puncture and resultant arachnoid bleb in new daily persistent headache: a case report. Headache 2023; 63 (07) 981-983
- 16 Nath S, Koziarz A, Badhiwala JH. et al. Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. Lancet 2018; 391 (10126): 1197-1204
- 17 Kim SC, Ryoo I, Sun HY, Park SW. MRI findings of spontaneous intracranial hypotension: usefulness of straight sinus distention. Am J Roentgenol 2019; 212 (05) 1129-1135
- 18 Lützen N, Zeitlberger A, Beck J, Urbach H. Teaching neuroimages: dynamic digital subtraction myelography discloses a ventral CSF leak in a patient with upper limb amyotrophy. Clin Neuroradiol 2023; 33 (01) 245-246
- 19 Girão MMV, Sousa RMP, Ribeiro MC, Cardoso TAMO, França Júnior MC, Reis F. Spontaneous intracranial hypotension and its complications. Arq Neuropsiquiatr 2018; 76 (08) 507-511
- 20 Benson JC, Madhavan AA, Cutsforth-Gregory JK, Johnson DR, Carr CM. The Monro-Kellie doctrine: a review and call for revision. Am J Neuroradiol 2023; 44 (01) 2-6
- 21 Callen AL, Dillon WP, Shah VN. Correction to: Unusual neuroimaging findings in spontaneous intracranial hypotension. Neuroradiology 2023; 65 (05) 883
- 22 Bond KM, Benson JC, Cutsforth-Gregory JK, Kim DK, Diehn FE, Carr CM. Spontaneous intracranial hypotension: atypical radiologic appearances, imaging mimickers, and clinical look-alikes. Am J Neuroradiol 2020; 41 (08) 1339-1347
- 23 Houk JL, Amrhein TJ, Gray L, Malinzak MD, Kranz PG. Differentiation of Chiari malformation type 1 and spontaneous intracranial hypotension using objective measurements of midbrain sagging. J Neurosurg 2021; 136 (06) 1796-1803
- 24 Dobrocky T, Mosimann PJ, Zibold F. et al. Cryptogenic cerebrospinal fluid leaks in spontaneous intracranial hypotension: Role of dynamic CT myelography. Radiology 2018; 289 (03) 766-772
- 25 Kranz PG, Luetmer PH, Diehn FE, Amrhein TJ, Tanpitukpongse TP, Gray L. Myelographic techniques for the detection of spinal CSF leaks in spontaneous intracranial hypotension. Am J Roentgenol 2016; 206 (01) 8-19
- 26 Kranz PG, Malinzak MD, Gray L, Willhite J, Amrhein TJ. Resisted inspiration improves visualization of CSF-venous fistulas in spontaneous intracranial hypotension. Am J Neuroradiol 2023; 44 (08) 994-998
- 27 Schievink WI, Maya MM, Chu RM, Moser FG. False localizing sign of cervico-thoracic CSF leak in spontaneous intracranial hypotension. Neurology 2015; 84 (24) 2445-2448
- 28 Medina JH, Abrams K, Falcone S, Bhatia RG. Spinal imaging findings in spontaneous intracranial hypotension. Am J Roentgenol 2010; 195 (02) 459-464
- 29 Farnsworth PJ, Madhavan AA, Verdoorn JT. et al. Spontaneous intracranial hypotension: updates from diagnosis to treatment. Neuroradiology 2023; 65 (02) 233-243
- 30 Schievink WI, Maya MM, Jean-Pierre S, Moser FG, Nuño M, Pressman BD. Rebound high-pressure headache after treatment of spontaneous intracranial hypotension: MRV study. Neurol Clin Pract 2019; 9 (02) 93-100
Address for correspondence
Publication History
Article published online:
16 September 2023
© 2023. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology 2001; 56 (12) 1746-1748
- 2 Robblee J, Secora KA, Alhilali LM, Knievel KL. Spontaneous Intracranial Hypotension Requires a High Index of Suspicion Because of Potentially Normal Diagnostic Test Results and Refractory Symptoms. Practical Neurology 2020
- 3 Sun-Edelstein C, Lay CL. Spontaneous intracranial hypotension: pathophysiology, clinical features, and diagnosis. UpToDate 2022
- 4 Headache classification committee of the international headache society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia 2018; 38 (01) 1-211
- 5 Cheema S, Anderson J, Angus-Leppan H. et al. Multidisciplinary consensus guideline for the diagnosis and management of spontaneous intracranial hypotension. J Neurol Neurosurg Psychiatry 2023
- 6 Urbach H, Fung C, Dovi-Akue P, Lützen N, Beck J. Spontaneous intracranial hypotension. Dtsch Arztebl Int 2020; 117 (27-28): 480-487
- 7 Kim D, Small JE. Intracranial Hypotension. In Small JE, Noujaim DL, Ginat DT, Kelly HR, Schaefer PW. (Ed), Neuroradiology. Elsevier; 2019: 158-162 . Doi: https://doi.org/10.1016/B978-0-323-44549-8.00017-1
- 8 Kranz PG, Gray L, Malinzak MD, Amrhein TJ. Spontaneous intracranial hypotension: pathogenesis, diagnosis, and treatment. Neuroimaging Clin N Am 2019; 29 (04) 581-594
- 9 Carlton Jones L, Butteriss D, Scoffings D. Spontaneous intracranial hypotension: the role of radiology in diagnosis and management. Clin Radiol 2022; 77 (03) e181-e194
- 10 Farb RI, Nicholson PJ, Peng PW. et al. Spontaneous intracranial hypotension: a systematic imaging approach for CSF leak localization and management based on MRI and digital subtraction myelography. Am J Neuroradiol 2019; 40 (04) 745-753
- 11 Luetzen N, Dovi-Akue P, Fung C, Beck J, Urbach H. Spontaneous intracranial hypotension: diagnostic and therapeutic workup. Neuroradiology 2021; 63 (11) 1765-1772
- 12 Mamlouk MD, Shen PY, Jun P, Sedrak MF. Spontaneous spinal CSF leaks stratified by age, body mass index, and spinal level. Am J Neuroradiol 2022; 43 (07) 1068-1072
- 13 Callen AL, Timpone VM, Schwertner A. et al. Algorithmic multimodality approach to diagnosis and treatment of spinal CSF leak and venous fistula in patients with spontaneous intracranial hypotension. Am J Roentgenol 2022; 219 (02) 292-301
- 14 Michali-Stolarska M, Bladowska J, Stolarski M, Sąsiadek MJ. Diagnostic imaging and clinical features of intracranial hypotension – review of literature. Pol J Radiol 2017; 82: 842-849
- 15 Callen AL, Lennarson P, Carroll IR. A causative role for remote dural puncture and resultant arachnoid bleb in new daily persistent headache: a case report. Headache 2023; 63 (07) 981-983
- 16 Nath S, Koziarz A, Badhiwala JH. et al. Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. Lancet 2018; 391 (10126): 1197-1204
- 17 Kim SC, Ryoo I, Sun HY, Park SW. MRI findings of spontaneous intracranial hypotension: usefulness of straight sinus distention. Am J Roentgenol 2019; 212 (05) 1129-1135
- 18 Lützen N, Zeitlberger A, Beck J, Urbach H. Teaching neuroimages: dynamic digital subtraction myelography discloses a ventral CSF leak in a patient with upper limb amyotrophy. Clin Neuroradiol 2023; 33 (01) 245-246
- 19 Girão MMV, Sousa RMP, Ribeiro MC, Cardoso TAMO, França Júnior MC, Reis F. Spontaneous intracranial hypotension and its complications. Arq Neuropsiquiatr 2018; 76 (08) 507-511
- 20 Benson JC, Madhavan AA, Cutsforth-Gregory JK, Johnson DR, Carr CM. The Monro-Kellie doctrine: a review and call for revision. Am J Neuroradiol 2023; 44 (01) 2-6
- 21 Callen AL, Dillon WP, Shah VN. Correction to: Unusual neuroimaging findings in spontaneous intracranial hypotension. Neuroradiology 2023; 65 (05) 883
- 22 Bond KM, Benson JC, Cutsforth-Gregory JK, Kim DK, Diehn FE, Carr CM. Spontaneous intracranial hypotension: atypical radiologic appearances, imaging mimickers, and clinical look-alikes. Am J Neuroradiol 2020; 41 (08) 1339-1347
- 23 Houk JL, Amrhein TJ, Gray L, Malinzak MD, Kranz PG. Differentiation of Chiari malformation type 1 and spontaneous intracranial hypotension using objective measurements of midbrain sagging. J Neurosurg 2021; 136 (06) 1796-1803
- 24 Dobrocky T, Mosimann PJ, Zibold F. et al. Cryptogenic cerebrospinal fluid leaks in spontaneous intracranial hypotension: Role of dynamic CT myelography. Radiology 2018; 289 (03) 766-772
- 25 Kranz PG, Luetmer PH, Diehn FE, Amrhein TJ, Tanpitukpongse TP, Gray L. Myelographic techniques for the detection of spinal CSF leaks in spontaneous intracranial hypotension. Am J Roentgenol 2016; 206 (01) 8-19
- 26 Kranz PG, Malinzak MD, Gray L, Willhite J, Amrhein TJ. Resisted inspiration improves visualization of CSF-venous fistulas in spontaneous intracranial hypotension. Am J Neuroradiol 2023; 44 (08) 994-998
- 27 Schievink WI, Maya MM, Chu RM, Moser FG. False localizing sign of cervico-thoracic CSF leak in spontaneous intracranial hypotension. Neurology 2015; 84 (24) 2445-2448
- 28 Medina JH, Abrams K, Falcone S, Bhatia RG. Spinal imaging findings in spontaneous intracranial hypotension. Am J Roentgenol 2010; 195 (02) 459-464
- 29 Farnsworth PJ, Madhavan AA, Verdoorn JT. et al. Spontaneous intracranial hypotension: updates from diagnosis to treatment. Neuroradiology 2023; 65 (02) 233-243
- 30 Schievink WI, Maya MM, Jean-Pierre S, Moser FG, Nuño M, Pressman BD. Rebound high-pressure headache after treatment of spontaneous intracranial hypotension: MRV study. Neurol Clin Pract 2019; 9 (02) 93-100