

Subscribe to RSS
DOI: 10.1055/s-0043-1774374
Influence of Breed and Body Conformation on Vertebral Implant Insert Angles in Dogs
Authors
Funding None.

Abstract
Objective To evaluate the effect of breed and body conformation on the vertebral insertion corridor angles for stabilizing spinal surgery in dogs.
Study Design Computed tomography studies of the vertebral column of 100 dogs from 10 representatives of 10 FCI (Fédération Cynologique Internationale) breed groups were randomly and blindly evaluated for vertebral insertion corridor angles. Insertion angles were measured for the last six cervical vertebrae (C2–C7), the last four thoracic vertebrae (T10–T13), the seven lumbar vertebrae (L1–L7), and the sacrum (S1).
Results Insertion angle was significantly influenced by breed at C6 (p = 0.001), C7 (p = 0.008), T13 (p = 0.032), L6 (p = 0.011), and S1 (p = 0.009). At C6, Pugs had significantly larger mean insertion angles (MIAs) compared with Beagles (p = 0.016), Miniature Dachshunds (p = 0.024), Greyhounds (p = 0.004), and West Highland White Terriers (p = 0.001). English Springer Spaniels had significantly smaller MIA at C7 compared with Siberian Huskies (p = 0.037) and Pugs (p = 0.033). German Shepherds had significantly smaller MIA at L6 compared with Beagles (p = 0.044), Miniature Schnauzers (p = 0.029), and English Springer Spaniels (p = 0.047). Miniature Dachshunds had significantly larger MIA at S1 compared with Beagles (p = 0.009), Pugs (p = 0.015), Miniature Schnauzers (p = 0.010), and English Springer Spaniels (p = 0.006).
Conclusion Breed and body conformation are important factors when planning instrumented spinal surgery in dogs. Individualized planning for spinal instrumentation seems to be critical.
Introduction
Spinal stabilization is indicated in a variety of canine spinal instability disorders including spinal fractures, luxations, and vertebral malformations. Surgical treatment is aimed at realigning and stabilizing the affected vertebrae, discs, and zygapophyseal joints with or without spinal cord decompression.[1] [2] [3] [4] [5] [6]
Although multiple surgical techniques for vertebral stabilization have been described, most involve the placement of screws or pins in multiple vertebral bodies.[7] [8] [9] While these surgical techniques provide rigid intervertebral fixation, they are associated with a risk of complication. Good knowledge of three-dimensional (3D) anatomy, diagnostic imaging, and advanced surgical skills are required to reduce the risks of iatrogenic injury to the vasculature, nerve roots, and spinal cord.[4] [5] [6] [10] [11] [12] [13] Other potential surgical complications include screws pulling out or technical failures such as pins breaching the cortex of the pedicles.[13] [14]
Recent studies have evaluated safe implant insertion corridors describing entry points, exit points, and insertion corridor angles in detail.[10] [13] [14] [15] [16] [17] These studies have demonstrated differences between anatomical regions and species, for example, cat versus dog.[18] It is currently unknown if body conformation influences safe insertion corridors. Dogs come in a wide range of shapes and sizes. The large variability in dog breeds characterized by different body conformations might pose an additional technical challenge in vertebral fixation surgery.
The aim of this study was therefore to evaluate the angles of safe insertion corridors in dogs of different breeds and with different body conformations. It was hypothesized that ideal insertion corridors, with an emphasis on insertion angles, would be different in dogs with different body conformations.
Materials and Methods
Data Collection
This study used retrospectively collected data from previously performed computed tomography (CT) scans for a variety of clinical indications at the small animal referral hospital at the Royal Veterinary College between May 2018 and May 2022. The study was considered below the threshold for ethical approval.
For the aims of this study, the selection of cases was based on the characterization of dogs as claimed by the international world canine organization Fédération Cynologique Internationale (FCI; https://www.fci.be/en/). According to FCI, purebred dogs are arranged in 10 individual groups. In this study, we opted for one representative breed from each group and then 10 dogs from each chosen representative breed. One hundred adult dogs from 10 separate breeds were selected. Representative breeds were designated from each group. ([Table 1]).
Abbreviation: FCI, Fédération Cynologique Internationale.
Dogs were included if the CT study included the cervical, thoracolumbar, and sacral vertebral column. In dogs with pathology that interfered with normal vertebral anatomy, such as fracture, luxation, previous spinal surgery, vertebral malformation, or diffuse idiopathic skeletal hyperostosis, measurements were solely performed on the unaffected vertebrae.
A 320-slice helical CT scanner was used in all cases (Aquilion ONE Genesis Edition, Canon Medical Systems, Otawara, Japan). The CT settings for image acquisition were helical mode, 1 to 2 mm slice thickness, −1 interval between slices, 140 kV, 120 mA, 110 mm acquisition field of view, bone, and soft tissue reconstruction algorithms, 512 × 512 matrix. After the axial CT study was completed, sagittal and coronal reconstructions were made.
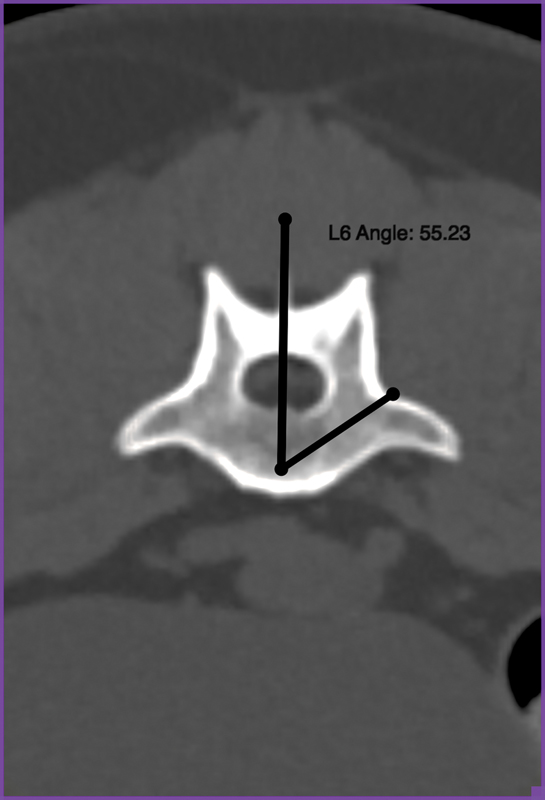
All studies were anonymized and randomized with a random number generator (www.random.org). All measurements were performed by one author who was unaware of the signalment of each individual dog (L.N.). The DICOM (Digital Imaging and Communications in Medicine) files were transferred from a picture archiving system to a computer workstation (MacBook Air, 2022, Apple, United States) and imported into an imaging software program (Horos, v3.3.6, www.horosproject.org). The CT images were viewed in a bone window using multiplanar reconstructions. The angle was defined by using the angle measurement tool in the Horos toolbar. Insertion corridor angles were measured, according to Watine et al, for the last six cervical vertebrae (C2–C7), the last four thoracic vertebrae (T10–T13), the seven lumbar vertebrae (L1–L7), and the sacrum (S1).[16] Technical aspects of the measurements were based on the same study. A ventral surgical approach was chosen for cervical vertebrae and a dorsal approach was chosen for thoracic, lumbar, and sacral vertebrae.
The characteristic of the insertion angle, α, was the angle between the insertion corridor and the sagittal plane of the vertebra ([Figs. 1] [2] [3]).


Statistical Analysis
The results were statistically analyzed using SPSS statistics 28 version 28.0.0.0 (IBM). Histograms were plotted of continuous variables (angle recorded for each vertebral body) to assess for normality of distribution. Normally distributed continuous data were analyzed with one-way analysis of variance (ANOVA) and pairwise post-hoc Tukey testing. Nonnormally distributed data were analyzed with a Kruskal–Wallis test. Normally distributed data are presented with mean and standard deviation, while nonnormal continuous data are presented with median and range. A p-value of 0.05 was considered significant.
Results
Of the 100 dogs included in this study, 52 were males (36 neutered) and 48 were females (38 neutered), aged between 11 months and 14.6 years (median: 9.9 years). CT was performed for a variety of clinical indications, including metastatic screening (n = 48), brachycephalic obstructive airway syndrome (n = 6), immune-mediated hemolytic anemia (n = 6), pyrexia of unknown origin (n = 6), cerebrovascular accident (n = 5), trauma (n = 4), lymphadenopathy (n = 4), immune-mediated polyarthritis (n = 4), cardiac disease (n = 4), gastrointestinal disease (n = 4), hepatic disease (n = 3), diffuse neuromuscular disease (n = 2), pleural effusion (n = 2), pyothorax (n = 1), and Horner's syndrome (n = 1).
A summary of the obtained insertion angles for each breed can be found in [Tables 2] [3] [4]. There was a significant influence of breed on the insertion angle for C6 (p = 0.001), C7 (p = 0.008), T13 (p = 0.032), L6 (p = 0.011), and S1 (p = 0.009) vertebrae. Pairwise comparisons for C6 revealed that Pugs had significantly larger mean insertion angle (MIA) compared with Beagles (p = 0.016), Miniature Dachshunds (p = 0.024), Greyhounds (p = 0.004), and West Highland White Terriers (WHWTs; p = 0.001). At C7, English Springer Spaniels (ESS) had significantly smaller MIA compared with Siberian Huskies (p = 0.037) and Pugs (p = 0.033). Pairwise comparisons for T13 did not reveal any significant differences between individual breeds. At L6, German Shepherd dogs had significantly smaller MIA compared with Beagles (p = 0.044), Miniature Schnauzers (p = 0.029), and ESS (p = 0.047). At S1, Miniature Dachshunds had a significantly larger MIA compared with Beagles (p = 0.009), Pugs (p = 0.015), Miniature Schnauzers (p = 0.010), and ESS (p = 0.006). No significant difference was identified in the insertion angles at the remaining vertebral levels ([Table 5] and [6]).
Discussion
This study evaluated the influence of breed and body conformation on the angle of an optimal anatomical trajectory in the transverse plane for spinal stabilizing surgery in 10 selected dog breeds of different body conformations. Although the obtained measurements agreed with previous studies, our results suggest that breed significantly influences the insertion angles of the C6, C7, T13, L6, and S1 vertebrae. In this study, the major differences were in Pugs at C6, ESS at C7, German Shepherds at L6, and Miniature Dachshunds at S1.
Although insertion angles have previously been determined for individual vertebral levels,[16] the results of this study suggest that body conformation can affect these angles. This limits the application of generalized insertion angles between breeds. It might therefore be ideal and even necessary to determine the ideal insertion corridor angle for each individual patient that requires instrumented spinal surgery. Presurgical planning of stabilizing spinal surgery requires diagnostic imaging to establish the optimal safe trajectory corridor. Imaging can be undertaken via survey radiographs, CT, or magnetic resonance imaging (MRI). Previous studies proved CT superior over radiographs and MRI in detecting vertebral osseous traumatic pathologies.[11] [14] [19] [20]
The sensitivity of conventional radiography is generally considered moderate for fractures and subluxations and low for evaluating exact implant placement.[11] [20] CT is more sensitive in identifying vertebral osseous pathologies and in assessing measurements considering surgery.[11] The possibility of 3D imaging allows measurements from all possible angles, valuable in surgical planning.[11] [14]
A combination of CT and MRI is recommended in a complete assessment of vertebral trauma in dogs. MRI may be able to detect the presence of soft tissue injuries and fractured vertebrae but cannot replace CT for identifying precise fracture morphology and possible measurements for implant placement.[19] [21]
All surgical techniques for spinal stabilization require accurate positioning of the stabilizing implants.[4] [5] [12] [16] Although CT is the ideal technique to determine optimal trajectories, it can be challenging to reproduce these ideal trajectories in vivo during spinal surgery.[14] Correct vertebral implant placement requires correct assessment of vertebral conformation and anatomy, emerging nerve roots and surrounding vasculature, and soft tissue structures. The difficulty of replicating ideal intraoperative insertion angles is demonstrated by several studies, where considerable differences between theoretical measurements and free-hand implant placement were shown.[7] [10] [13] [15] [17]
More recent developments in veterinary medicine advocate the use of individualized and custom-made 3D drill guides.[3] [10] [22] [23] This new technology facilitates more accurate and hence safer implant placement; however, it comes with an expense. In addition, 3D drill guides are not widely available and can be considered cost-prohibited for a subset of clients. And even if they reduce the risk of complications, most fractures/luxations are time critical and cannot be delayed for the printing of guides. For most veterinary surgeons, there will be situations where in vivo free-hand positioning inevitably is required. Apart from detailed knowledge about the specific type of vertebra and the mean angle of insertion for a safe trajectory, this study suggests adding breed and body conformation into individualized surgical planning. Although this study identified that especially Pugs at C6, ESS at C7, German Shepherds at L6, and Miniature Dachshunds at S1 had different insertion angles, more extensive studies are necessary to evaluate for potential differences between additional breeds.
The current study has several limitations. First, all measurements were performed by a single person. It can however be hypothesized that this could have contributed to the consistency of the measurements. However, using multiple reviewers could allow for testing measurement sensitivity. Second, only one representative breed was selected for each group of dogs. Although this approach was sufficient to demonstrate the influence of body conformation on insertion angles, it remains unclear if the obtained measurements of one breed can be extrapolated to other breeds within the same group. The FCI groups are large and heterogeneous with several breeds of different sizes and conformation within the same group. Identifying the ideal representative breed for one group is challenging. For example, in FCI group 8, retrievers, flushing dogs, and water dogs, where an ESS was chosen as a representative breed in this study, there are substantial differences from larger dogs such as Golden Retrievers or Labrador Retrievers. Even within the same breed, there can be considerably different phenotypes. In addition, some of the selected breeds, WHWTs, Pugs, and Beagles, carry several chondrodystrophic characteristics that might influence the vertebral conformation. These are all factors favoring an individualized approach. Considering the heterogenicity of the breeds within the FCI groups, the identified insertion angles of specific vertebrae should probably not be used as generalized corridor angles.
In addition, insertion corridor angles are merely one part of the presurgical planning. Additional aspects such as entrance points, exit points, and evaluation of implant positioning in the sagittal and coronal plane will likewise have an impact on the outcome. Moreover, the clinical relevance of smaller differences in insertion angles can be debated as these might be challenging to achieve surgically.
In conclusion, the results of this study suggest adding breed into the individualized surgical planning and underline that breed by itself is an important factor when managing spinal stabilizing surgery in dogs. Individual planning is critical but safe corridor angles of specific vertebrae, as presented in this study, can support the assessment. To optimize a safe trajectory for implant positioning, performing transverse imaging to measure the precise insertion corridor angle in the specific vertebra might be considered worthwhile.
The limited number of selected breeds in this study opens the possibility that similar statistically significant differences might be present in additional breeds and vertebrae.
Conflict of Interest
None declared.
-
References
- 1 Aikawa T, Kanazono S, Yoshigae Y, Sharp NJH, Muñana KR. Vertebral stabilization using positively threaded profile pins and polymethylmethacrylate, with or without laminectomy, for spinal canal stenosis and vertebral instability caused by congenital thoracic vertebral anomalies. Vet Surg 2007; 36 (05) 432-441
- 2 Auger J, Dupuis J, Quesnel A, Beauregard G. Surgical treatment of lumbosacral instability caused by discospondylitis in four dogs. Vet Surg 2000; 29 (01) 70-80
- 3 Fujioka T, Nakata K, Nishida H. et al. A novel patient-specific drill guide template for stabilization of thoracolumbar vertebrae of dogs: cadaveric study and clinical cases. Vet Surg 2019; 48 (03) 336-342
- 4 Jeffery ND. Vertebral fracture and luxation in small animals. Vet Clin North Am Small Anim Pract 2010; 40 (05) 809-828
- 5 Sharp NJH, Wheeler SJ. Small Animal Spinal Cord Disorders. 2nd ed. Philadelphia, PA: Elsevier Mosby; 2005: 60-61 , 299, 321–322
- 6 Steffen F, Voss K, Morgan JP. Distraction-fusion for caudal cervical spondylomyelopathy using an intervertebral cage and locking plates in 14 dogs. Vet Surg 2011; 40 (06) 743-752
- 7 Blass CE, Seim III HB. Spinal fixation in dogs using Steinmann pins and methyl methacrylate. Vet Surg 1984; 13 (04) 203-210
- 8 Gougeon E, Meheust P. Pedicle screws implantation in polymethylmethacrylate construct to stabilise sixth lumbar vertebral body fracture in dogs: 5 cases (2015-2018). J Small Anim Pract 2021; 62 (11) 1007-1015
- 9 Trotter EJ. Cervical spine locking plate fixation for treatment of cervical spondylotic myelopathy in large breed dogs. Vet Surg 2009; 38 (06) 705-718
- 10 Guevar J, Bleedorn J, Cullum T, Hetzel S, Zlotnick J, Mariani CL. Accuracy and safety of three-dimensionally printed animal-specific drill guides for thoracolumbar vertebral column instrumentation in dogs: bilateral and unilateral designs. Vet Surg 2021; 50 (02) 336-344
- 11 Hettlich BF, Fosgate GT, Levine JM. et al. Accuracy of conventional radiography and computed tomography in predicting implant position in relation to the vertebral canal in dogs. Vet Surg 2010; 39 (06) 680-687
- 12 Tran JH, Hall DA, Morton JM, Deruddere KJ, Snelling SR. Accuracy and safety of pin placement during lateral versus dorsal stabilization of lumbar spinal fracture-luxation in dogs. Vet Surg 2017; 46 (08) 1166-1174
- 13 Samer ES, Forterre F, Rathmann JMK, Stein VM, Precht CM, Guevar J. Accuracy and safety of image-guided freehand pin placement in canine cadaveric vertebrae. Vet Comp Orthop Traumatol 2021; 34 (05) 338-345
- 14 Schmitt EM, Early P, Bergman R. et al. Computed tomography evaluation of proposed implant corridors in canine thoracic vertebrae. Vet Surg 2021; 50 (07) 1427-1433
- 15 Smolders LA, Voorhout G, van de Ven R. et al. Pedicle screw-rod fixation of the canine lumbosacral junction. Vet Surg 2012; 41 (06) 720-732
- 16 Watine S, Cabassu JP, Catheland S, Brochier L, Ivanoff S. Computed tomography study of implantation corridors in canine vertebrae. J Small Anim Pract 2006; 47 (11) 651-657
- 17 Wheeler JL, Cross AR, Rapoff AJ. A comparison of the accuracy and safety of vertebral body pin placement using a fluoroscopically guided versus an open surgical approach: an in vitro study. Vet Surg 2002; 31 (05) 468-474
- 18 Vallefuoco R, Bedu AS, Manassero M, Viateau V, Niebauer G, Moissonnier P. Computed tomographic study of the optimal safe implantation corridors in feline thoraco-lumbar vertebrae. Vet Comp Orthop Traumatol 2013; 26 (05) 372-378
- 19 Gallastegui A, Davies E, Zwingenberger AL, Nykamp S, Rishniw M, Johnson PJ. MRI has limited agreement with CT in the evaluation of vertebral fractures of the canine trauma patient. Vet Radiol Ultrasound 2019; 60 (05) 533-542
- 20 Kinns J, Mai W, Seiler G. et al. Radiographic sensitivity and negative predictive value for acute canine spinal trauma. Vet Radiol Ultrasound 2006; 47 (06) 563-570
- 21 Johnson P, Beltran E, Dennis R, Taeymans O. Magnetic resonance imaging characteristics of suspected vertebral instability associated with fracture or subluxation in eleven dogs. Vet Radiol Ultrasound 2012; 53 (05) 552-559
- 22 Hamilton-Bennett SE, Oxley B, Behr S. Accuracy of a patient-specific 3D printed drill guide for placement of cervical transpedicular screws. Vet Surg 2018; 47 (02) 236-242
- 23 Oxley B, Behr S. Stabilisation of a cranial cervical vertebral fracture using a 3D-printed patient-specific drill guide. J Small Anim Pract 2016; 57 (05) 277
Address for correspondence
Publication History
Received: 09 April 2023
Accepted: 30 June 2023
Article published online:
23 November 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Aikawa T, Kanazono S, Yoshigae Y, Sharp NJH, Muñana KR. Vertebral stabilization using positively threaded profile pins and polymethylmethacrylate, with or without laminectomy, for spinal canal stenosis and vertebral instability caused by congenital thoracic vertebral anomalies. Vet Surg 2007; 36 (05) 432-441
- 2 Auger J, Dupuis J, Quesnel A, Beauregard G. Surgical treatment of lumbosacral instability caused by discospondylitis in four dogs. Vet Surg 2000; 29 (01) 70-80
- 3 Fujioka T, Nakata K, Nishida H. et al. A novel patient-specific drill guide template for stabilization of thoracolumbar vertebrae of dogs: cadaveric study and clinical cases. Vet Surg 2019; 48 (03) 336-342
- 4 Jeffery ND. Vertebral fracture and luxation in small animals. Vet Clin North Am Small Anim Pract 2010; 40 (05) 809-828
- 5 Sharp NJH, Wheeler SJ. Small Animal Spinal Cord Disorders. 2nd ed. Philadelphia, PA: Elsevier Mosby; 2005: 60-61 , 299, 321–322
- 6 Steffen F, Voss K, Morgan JP. Distraction-fusion for caudal cervical spondylomyelopathy using an intervertebral cage and locking plates in 14 dogs. Vet Surg 2011; 40 (06) 743-752
- 7 Blass CE, Seim III HB. Spinal fixation in dogs using Steinmann pins and methyl methacrylate. Vet Surg 1984; 13 (04) 203-210
- 8 Gougeon E, Meheust P. Pedicle screws implantation in polymethylmethacrylate construct to stabilise sixth lumbar vertebral body fracture in dogs: 5 cases (2015-2018). J Small Anim Pract 2021; 62 (11) 1007-1015
- 9 Trotter EJ. Cervical spine locking plate fixation for treatment of cervical spondylotic myelopathy in large breed dogs. Vet Surg 2009; 38 (06) 705-718
- 10 Guevar J, Bleedorn J, Cullum T, Hetzel S, Zlotnick J, Mariani CL. Accuracy and safety of three-dimensionally printed animal-specific drill guides for thoracolumbar vertebral column instrumentation in dogs: bilateral and unilateral designs. Vet Surg 2021; 50 (02) 336-344
- 11 Hettlich BF, Fosgate GT, Levine JM. et al. Accuracy of conventional radiography and computed tomography in predicting implant position in relation to the vertebral canal in dogs. Vet Surg 2010; 39 (06) 680-687
- 12 Tran JH, Hall DA, Morton JM, Deruddere KJ, Snelling SR. Accuracy and safety of pin placement during lateral versus dorsal stabilization of lumbar spinal fracture-luxation in dogs. Vet Surg 2017; 46 (08) 1166-1174
- 13 Samer ES, Forterre F, Rathmann JMK, Stein VM, Precht CM, Guevar J. Accuracy and safety of image-guided freehand pin placement in canine cadaveric vertebrae. Vet Comp Orthop Traumatol 2021; 34 (05) 338-345
- 14 Schmitt EM, Early P, Bergman R. et al. Computed tomography evaluation of proposed implant corridors in canine thoracic vertebrae. Vet Surg 2021; 50 (07) 1427-1433
- 15 Smolders LA, Voorhout G, van de Ven R. et al. Pedicle screw-rod fixation of the canine lumbosacral junction. Vet Surg 2012; 41 (06) 720-732
- 16 Watine S, Cabassu JP, Catheland S, Brochier L, Ivanoff S. Computed tomography study of implantation corridors in canine vertebrae. J Small Anim Pract 2006; 47 (11) 651-657
- 17 Wheeler JL, Cross AR, Rapoff AJ. A comparison of the accuracy and safety of vertebral body pin placement using a fluoroscopically guided versus an open surgical approach: an in vitro study. Vet Surg 2002; 31 (05) 468-474
- 18 Vallefuoco R, Bedu AS, Manassero M, Viateau V, Niebauer G, Moissonnier P. Computed tomographic study of the optimal safe implantation corridors in feline thoraco-lumbar vertebrae. Vet Comp Orthop Traumatol 2013; 26 (05) 372-378
- 19 Gallastegui A, Davies E, Zwingenberger AL, Nykamp S, Rishniw M, Johnson PJ. MRI has limited agreement with CT in the evaluation of vertebral fractures of the canine trauma patient. Vet Radiol Ultrasound 2019; 60 (05) 533-542
- 20 Kinns J, Mai W, Seiler G. et al. Radiographic sensitivity and negative predictive value for acute canine spinal trauma. Vet Radiol Ultrasound 2006; 47 (06) 563-570
- 21 Johnson P, Beltran E, Dennis R, Taeymans O. Magnetic resonance imaging characteristics of suspected vertebral instability associated with fracture or subluxation in eleven dogs. Vet Radiol Ultrasound 2012; 53 (05) 552-559
- 22 Hamilton-Bennett SE, Oxley B, Behr S. Accuracy of a patient-specific 3D printed drill guide for placement of cervical transpedicular screws. Vet Surg 2018; 47 (02) 236-242
- 23 Oxley B, Behr S. Stabilisation of a cranial cervical vertebral fracture using a 3D-printed patient-specific drill guide. J Small Anim Pract 2016; 57 (05) 277