

Subscribe to RSS
DOI: 10.1055/s-0043-1775855
CT Arterioportography for Complex Portomesenteric Venous Interventions
Authors


Abstract
Authors report the use of computed tomography arterioportography (CTAP) in the diagnosis and endovascular treatment of portomesenteric venous occlusion. Three patients (2 male and 1 female; median age: 51 years) with an extrahepatic portal or mesenteric venous occlusion and variceal bleeding were included in this institutional review boards-approved retrospective study. CTAP was performed with an angiographic catheter positioned in the proximal superior mesenteric artery, and CT was obtained during the venous phase following the intra-arterial injection of contrast material. CTAP provided excellent opacification and delineation of portomesenteric veins, including occlusion length, intravascular webs, venous collaterals, and bleeding varices. This enabled preoperative planning for complex recanalization or extra-anatomic bypass to treat extrahepatic portal and mesenteric venous obstruction. There were no complications related to CTAP.
Keywords
CT arterioportography - porto-mesenteric venous disease - variceal bleeding - transjugular intrahepatic portosystemic shunt - mesenteric venous stentIntroduction
Computed tomography arterioportography (CTAP) has been used to assess the presence, location, and number of primary and secondary tumors in the liver.[1] In this technique, the superior mesenteric or splenic arteries are selectively catheterized. CT of the liver is performed during the portal venous phase following intra-arterial injection of contrast material. This was once considered the most sensitive test for detecting hepatic tumors but is now replaced with contrast-enhanced magnetic resonance imaging (MRI).[2] Recently, the utility of CTAP in assessing the patency of portal and mesenteric veins, and the physiological effects of portal hypertension, including various portosystemic collateral pathways, has been reported in pediatric patients.[3] [4] In this study, we report the clinical utility of CTAP in assessing the complex portal and mesenteric venous anatomy before interventional therapy in patients who presented with an extrahepatic portal or mesenteric venous occlusion and variceal bleeding.
CT Arterioportography: Technique
A standard protocol was applied for CTAP in all the cases presented in this study. The superior mesenteric artery was catheterized with a 5F catheter via a right femoral arterial access in an angiography suite. A digital subtraction angiography (DSA) of the superior mesenteric artery was performed in an anteroposterior projection, and the image acquisition was continued to include the venous phase. The time required to opacify the portal vein from the initial intra-arterial contrast material injection was calculated. This time was used during CTAP as the time delay from contrast material injection to image acquisition. The patient was transferred to a dual-energy multi-detector CT scanner (SOMATOM Force, Siemens, Germany). CT images were acquired during the arterial phase, portovenous phase, and delayed phase. The arterial and portovenous phases were obtained in dual-energy mode (0.5mm detector width, rotation time of 0.25sec, 80kVp, and 140kVp, and table speed of 70 cm/s). The delayed venous phase images were acquired in single energy mode at 140kVp. Images were reconstructed at 1 mm slice thickness at 70keV and 50keV. Data were reconstructed in multiplanar reformations and three-dimensional volume rendering. The arterial catheter was removed, and the arterial access was closed with a closure device. The intervention was performed a few days later.
Case 1
A 57-year-old man presented with acute upper gastrointestinal bleeding. He was hemodynamically stable. Prior history was significant for a known superior mesenteric vein thrombosis 10 years prior to presentation, which was managed conservatively with anticoagulation. An endoscopy at admission showed large submucosal varices with active bleeding in the third portion of the duodenum. The bleeding varix was treated endoscopically. A contrast-enhanced CT ([Fig. 1A]) and a subsequent contrast-enhanced MRI of the abdomen showed large duodenal varices and focal questionable narrowing of the superior mesenteric vein. The rest of the portomesenteric and splenic veins were normal. A superior mesenteric angiography ([Fig. 1B, C]) showed a patent superior mesenteric artery, no arteriovenous malformation, multiple midline varices, and a patent portal vein but inadequate opacification of the superior mesenteric vein. CTAP ([Fig. 1D–E]) demonstrated focal web-like structures within the proximal superior mesenteric vein and large duodenal varices. The portal vein and the rest of the superior mesenteric vein were patent.

Under moderate sedation and a transhepatic portal venous approach, the superior mesenteric venous webs were crossed with a combination of a 5F Kumpe catheter and 0.035” angled hydrophilic guide wire. A superior mesenteric venography ([Fig. 1F–G]) showed focal occlusion of the proximal superior mesenteric vein secondary to the web and subsequent flow of contrast material into the portal vein via the duodenal varices. The focal occlusions were treated with balloon angioplasty using a 6 × 40mm high-pressure balloon (Conquest, Boston Scientific, Natick, Massachusetts, United States) and subsequently by placing a 12mm x 40mm Protégé self-expanding bare metallic stent (Medtronic, Minneapolis, Minnesota, United States) ([Fig. 1H]). The stent was dilated to 10 mm with a 10 × 40mm Armada balloon (Abbott, Plymouth, Minnesota, United States). Postintervention, superior mesenteric venography ([Fig. 1I]) showed a widely patent portal and mesenteric veins with no opacification of duodenal varices. The patient was prescribed warfarin for 6 months and aspirin for life. A 1-month follow-up CT and ultrasound at 28 months showed a patent stent with no significant duodenal varices. Endoscopy at 3 months showed no duodenal varices. Clinically, the patient reported no recurrent gastrointestinal bleeding.
Case 2
A 34-year-old man with a history of recurrent upper and lower gastrointestinal bleeding from duodenal and jejunal varices was referred to interventional radiology. He had multiple episodes of variceal bleeding, which were treated with endoscopic therapies. His medical history was significant for chronic portal vein thrombosis from infancy, Factor V Leiden deficiency, prior cardiac surgery for congenital cardiac defects, splenectomy for portal hypertension, and failed splenorenal and mesocaval surgical shunts. CT demonstrated an occluded main portal vein but a patent superior mesenteric vein. A superior mesenteric angiography ([Fig. 2A]) showed inadequate opacification of the portomesenteric veins due to the blush of overlying structures and the bowel. CTAP was performed to assess for collaterals, varices, and anatomy of intrahepatic portal veins.

CTAP showed a chronically occluded portal vein with extensive portosystemic collaterals, including a large superior mesenteric collateral that contributed to peri-gallbladder varices, varices around the gastric antrum, gastric fundus, duodenum, lower esophagus, descending colon, and rectum, and pericapsular varices around the left lobe draining into the left portal vein and mild nodularity of the anterior liver contour consistent with cirrhosis ([Fig. 2B]).
A few weeks later, the patient underwent a successful direct intrahepatic mesocaval shunt between the inferior vena cava and the large superior mesenteric collateral that contributed to the gallbladder varices. This was performed via a transjugular venous approach, aided by a transfemoral venous intravascular ultrasound guidance and percutaneous access to the collateral from the mid-abdomen ([Fig. 2C–E]). A constrained Viatorr (Gore, Flagstaff, Arizona, United States) graft was used for the mesocaval shunt, and the stent was dilated to 10mm. The procedure was complicated by intraprocedural thrombosis of the stent graft and the superior mesenteric vein, successfully treated with suction thrombectomy. Post-stent subtraction venogram demonstrated patent blood flow through the stent with a decrease in the caliber of the collaterals ([Fig. 2F]). The patient was discharged on Apixaban. The mesocaval shunt remained patent on ultrasound during the 10-month follow-up with no clinical signs of variceal bleeding. The patient had one hepatic encephalopathy episode, which was successfully treated with medical therapy.
Case 3
A 51-year-old woman with a known diagnosis of autoimmune hepatitis and biliary stricture presented with massive upper gastrointestinal bleeding during endoscopic retrograde cholangiopancreatography (ERCP). The patient had a prior history of main portal vein thrombosis and splenic vein thrombosis with peribiliary varices. MRI showed peribiliary varices ([Fig. 3A]), but the extent of main portal vein obstruction and intrahepatic portal vein status was unclear. A superior mesenteric angiography ([Fig. 3B]) showed inadequate opacification of the portomesenteric veins due to the blush of overlying structures and the bowel.
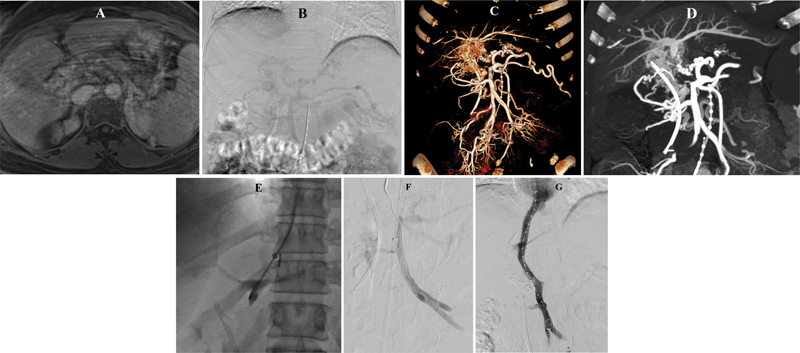
CTAP ([Fig. 3C, D]) showed occlusion of the main portal vein from the splenoportal confluence and up to portal vein bifurcation, occlusion of proximal right and left portal veins but reconstituted and patent distal left and distal right portal vein branches. The splenic vein was occluded. There were large peribiliary varices. The perihepatic collaterals connected the left gastric veins to the left portal vein.
Under general anesthesia and intravascular ultrasound guidance, the left portal vein was accessed from the middle hepatic vein via a transjugular venous approach using a Colapinto needle (Ring Set, Cook Medical, Bloomington, Illinois, United States; [Fig. 3E, F]). The occluded left and main portal veins were crossed with a 0.018” guide wire and microcatheter, which were subsequently upsized for a 0.035” wire. The occluded veins were dilated, and a Viatorr stent graft was placed across the parenchymal tract. The peribiliary varices were embolized using 33% n-butyl cyanoacrylate. Post-transjugular portosystemic stent shunt (TIPS) and variceal embolization, there was good flow from the superior mesenteric vein to the right atrium ([Fig. 3G]). The procedure was subsequently complicated by stent thrombosis 4 weeks later, which was treated with suction thrombectomy, portal vein angioplasty, and additional perisplenic and gastric variceal embolization. During a 5-month follow-up, the patient had no bleeding episodes and had successful ERCP and biliary stent exchanges. CT at 2 months showed patent TIPS and patent portomesenteric veins.
Discussion
Conventional CT and DSA have limitations when imaging the portomesenteric venous system due to the dilution of iodinated contrast material in the venous system. Mesenteric venous imaging during DSA is also prone to artifacts from the blush of overlying structures and the bowel. CTAP is capable of objectively and comprehensively revealing all types of portomesenteric venous anomalies in a three-dimensional manner. It can provide excellent opacification and delineation of portomesenteric veins, including occlusion length, intravascular webs, venous collaterals, and bleeding varices. This ability of CTAP is extremely valuable in complex cases that require interdisciplinary discussions involving interventional radiologists, surgeons, and gastroenterologists to determine the most suitable management approach.
In the case series described above, CTAP helped us identify portosystemic collaterals that were not visible on CT and DSA and offered alternative access routes for interventional radiological shunt creation and treatment of varices. It also helped evaluate the patency and direction of flow in the mesenteric veins and the specific source of the varices. This allowed complex recanalization and extra-anatomic bypass to treat extrahepatic portal and mesenteric venous obstruction in the cases we described. There were no complications related to CTAP.
Therefore, CTAP can be implemented before considering more invasive procedures, as it provides valuable insights for individualized management. Though a hybrid-CT (angio-CT) suite streamlines the process of acquiring CTAP images, the technique provides high value and should be considered even in institutions where a hybrid suite is not available.
Conflict of Interest
Dr. Patrick D. Sutphin reported following:
"Grants or contracts from “Research funding from TriSalus Life Sciences, Inc. unrelated to current work” and “Spark Award from Massachusetts General Hospital research funding, unrelated to current work.”.
Patents from “US9079859B2: Synthetic lethal targeting of glucose transport”
Stock from “CVS Health Corp, Gilead Sciences Inc, Crispr Therapeutics Ag Namen Akt, Intellia Therapeutics Inc, Teladoc Health Inc” of these “American Well Corp, Axcella Health Inc, Editas Medicine Inc, Rubius Therapeutics Inc” have made payments.
Dr. Sanjeeva P. Kalva reported following:
Grants or contracts from “NIH, BD, Black Swan, Trisalus, CRICO”.
Royalties or licenses from “Elsevier, Springer, Thieme”.
Consulting fees from “Penumbra, Okami Medical, Boston Scientific, Medtronic, Covidien, Instylla, BD, Cannon, Varian, SIRTEX,”.
Payment or honoraria from “Boston Scientific, Medtronic, Cannon”.
Support from “Cannon Medical”.
Participation with “NIH”.
Role in “Chief, Interventional Radiology, Massachusetts General Hospital, Boston, MA ”, “Chair, Vascular Panel, ACR Appropriateness Criteria”, “International Editor, Journal of Clinical Interventional Radiology ISVIR; Assistant Editor/Consultant to Editor, Radiology – Cardiothoracic, RSNA; Adjunct faculty, Christian Medical College, Vellore, India; Advisor, KMCH Institute of Health Sciences, Coimbatore, India”.
Stock in “Biogen Inc, Clover Health Investments Corp, Inovio Pharmaceuticals, Moderna Inc, Pfizer Inc, Novavax Inc, Orphazyme, Cassava Sciences Inc, Vivos Therapeutics Inc, Ardelyx Inc, Althea Health, Sarepta Therapeutics, Clover Health Investments Corp, CureVac BV, Immunoprecise Antibodies Ltd, Infinity Pharmaceuticals Inc, Zymergen Inc, BioNTech SE, Trillium Therapeutics Inc, Theravance Biopharma Inc, Doximity Inc, Eargo Inc, Allogent Therapeutics Inc, NRx Pharmaceuticals Inc, Atea pharmaceuticals Inc, Fate Therapeutics”.
Interests in “University of Texas Southwestern Medical Center” and “Harvard Medical School”.
All other authors reported no conflict of interest.
-
References
- 1 Soyer P, Bluemke DA, Fishman EK. CT during arterial portography for the preoperative evaluation of hepatic tumors: how, when, and why?. AJR Am J Roentgenol 1994; 163 (06) 1325-1331
- 2 Kim YK, Kwak HS, Han YM, Kim CS. Usefulness of combining sequentially acquired gadobenate dimeglumine-enhanced magnetic resonance imaging and resovist-enhanced magnetic resonance imaging for the detection of hepatocellular carcinoma: comparison with computed tomography hepatic arteriography and computed tomography arterioportography using 16-slice multidetector computed tomography. J Comput Assist Tomogr 2007; 31 (05) 702-711
- 3 Hammer S, Zeman F, Schlitt HJ. et al. Comparison of sequential CT arterioportography-arteriosplenography with standard cross-sectional imaging and endoscopy in children with portal hypertension. Sci Rep 2022; 12 (01) 6554
- 4 Hammer S, Schlitt HJ, Knoppke B, Huf VI, Wohlgemuth WA, Uller W. Sequential CT arterioportography-arteriosplenography depicts individual haemodynamic changes in children with portal hypertension without cirrhosis. Eur Radiol Exp 2020; 4 (01) 65
Address for correspondence
Publication History
Article published online:
19 October 2023
© 2023. Indian Society of Vascular and Interventional Radiology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Soyer P, Bluemke DA, Fishman EK. CT during arterial portography for the preoperative evaluation of hepatic tumors: how, when, and why?. AJR Am J Roentgenol 1994; 163 (06) 1325-1331
- 2 Kim YK, Kwak HS, Han YM, Kim CS. Usefulness of combining sequentially acquired gadobenate dimeglumine-enhanced magnetic resonance imaging and resovist-enhanced magnetic resonance imaging for the detection of hepatocellular carcinoma: comparison with computed tomography hepatic arteriography and computed tomography arterioportography using 16-slice multidetector computed tomography. J Comput Assist Tomogr 2007; 31 (05) 702-711
- 3 Hammer S, Zeman F, Schlitt HJ. et al. Comparison of sequential CT arterioportography-arteriosplenography with standard cross-sectional imaging and endoscopy in children with portal hypertension. Sci Rep 2022; 12 (01) 6554
- 4 Hammer S, Schlitt HJ, Knoppke B, Huf VI, Wohlgemuth WA, Uller W. Sequential CT arterioportography-arteriosplenography depicts individual haemodynamic changes in children with portal hypertension without cirrhosis. Eur Radiol Exp 2020; 4 (01) 65