Subscribe to RSS
DOI: 10.1055/s-0043-1776134
Acupuncture in the Treatment of a Series of Patients with Chronic Pain Associated with Hip Osteoarthritis
Article in several languages: português | English
Abstract
Objective Hip osteoarthritis (HO) causes pain and deranges functioning. Surgical treatment is the preferred approach in severe cases, but clinical comorbidities, age and the long waiting list may compromise quality of life. This study aimed to describe the results of acupuncture for the control pain and improvement of functioning in subjects with HO.
Method Twelve severe HO patients were treated with ten weekly sessions of a standardized acupuncture point protocol. Pain intensity was assessed with the Visual Analog Pain Scale (VAS) and quality of life with WOMAC Index.
Results Pain intensity (VAS) reduced from 75.8 ± 18.8 mm to 20.0 ± 22.6 mm after 10 acupuncture sessions and 48.3 ± 26.6mm in the follow-up (ANOVA F = 7.99; p < 0.001). WOMAC Index values reduced from 74.7 ± 12.7 to 45.7 ± 22.1 and 54.6 ± 22.9 at the same timepoints.
Conclusion Acupuncture is an effective conservative rehabilitation strategy to reduce pain and improve quality of life in subjects with severe HO.
#
Introduction
Hip osteoarthritis (HO) is a prevalent joint disease which is characterized by pain both during rest or, most commonly, while standing, walking, and moving around. The treatment of HO aims to relieve pain and restore functioning and quality of life. Severe anatomic impairment of the joint is satisfactorily treated with hip replacement, but old age, comorbidities[1] and the long waiting lists for this procedure in the Brazilian public health system[2] demand conservative analgesic and rehabilitative interventions for these patients.
Acupuncture, used in China and other Asian countries over the last 3,000 years, represents a valuable complementary therapy for pain control,[3] in addition to representing lower health costs by reducing the number of prescription drugs and hospitalizations.[4]
A recent systematic review on the effects of acupuncture on HO concluded, however, that acupuncture has little or no effect in reducing pain or improving function relative to sham acupuncture.[5] However, many studies included in this review have methodologic limitation and comprise control groups with a weak acupuncture effect. Given this scenario, acupuncture should be tested as a conservative treatment to total hip replacement (THR).
This study aimed to describe the results of acupuncture treatment for analgesia and improved quality of life in a series of patients with severe HO in a waiting list for THR.
#
Methods
This study was approved by the Internal Review Board at the Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto (HCRP) (Protocol 4,105,165 and CAAE 32396920.9.0000.5440) and the subjects signed an informed consent form.
Five women and seven men with severe HO (mean age: 57.9 ± 10.6 years) were prospectively recruited of rehabilitation outpatient clinic from June 2020 to January 2021. The sample size was calculated using the Sample Size Calculation tool from the MGH Biostatistic Center. Eleven participants were required for 80% power to detect difference of 25% in the pain VAS, assuming SD= 25mm and significance level of 0.05. We started the study with fifteen participants to prevent dropout losses and ended the study with a total of twelve individuals. The COVID19 pandemic restricted sample size because of the health care interruption. Quantitative variables were summarized by measures of central tendency and dispersion, while categorical variables were classified and summarized by percentages of categories. After verifying the normality of the distribution of variables, the ANOVA test for repeated measures was used to test the hypothesis that pain intensity and functioning would improve with treatment. The significance level was 0.05.
Subjects should be adults diagnosed with unilateral HO according to clinical criteria,[6] be classified as grade three or four in the Kellgren-Lawrence radiological classification,[7] present with pain intensity greater than four assessed by the Visual Analog Scale (VAS), failure in conservative treatment consisting of: exercises, pharmacological therapies such as analgesics or anti-inflammatory drugs, use of walking aids, or no improvement when performing trigger point blocks[8]; and not being previously treated with acupunture were also required. Exclusion criteria included any limitation to understand the assessment or treatment, difficulty in clinical follow-up and attendance at reassessments for any reason, other diagnoses of hip or other lower limb painful condition.
The first assessment was performed immediately after recruitment and subjects pain intensity was assessed with VAS,[9] The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) considers three dimensions of functioning of HO: pain (range 0–20 points), stiffness (range 0–8 points) and physical function (range 0–68 points),[10] and the ten-meter walk test (performed on a flat, 14-meter straight surface for the highest possible walking speed).[11] The Medication Consumption Diary quantified the use of analgesics and anti-inflammatories to relieve pain.[12] Two other evaluations were performed immediately after treatment and five weeks after the end of treatment.
For ten acupuncture sessions, subjects were laterally positioned over the unaffected side. The treatment was performed by the same physician (RA – five years of acupuncture practice, board certified) with deep insertion of sterile acupuncture needles (0.30mm diameter, 70mm length) until the “de Qi” sensation for 20 minutes. Six points were used: GB29, GB30, GB34, GB36, BL62, SJ5[13] [14] based on Traditional Chinese Medicine (TCM) techniques.[15]
All participants also received the standard treatment at the HCRP Rehabilitation Center, which includes physiotherapy at the institution and behavioral and exercise guidance at home, as well as the use of optimized medications.
#
Results
All twelve patients remained until the end of the study. The biodemographic and baseline clinical data of HO subjects is illustrated in [Table 1].
|
Baseline biodemographic and clinical data of HO subjects |
|
|---|---|
|
Variable |
n (%) |
|
Gender |
Subjects |
|
Male |
7 (58.4%) |
|
Female |
5 (41.6%) |
|
Affected Side |
|
|
Right |
2 (16.7%) |
|
Left |
10 (83.3%) |
|
Variable |
Mean (SD) |
|
Age (years) |
57.9 (10.6) |
|
Diagnosis Time (years) |
19.5 (14.0) |
|
VAS (mm) |
75.8 (18.8) |
|
WOMAC (points) |
74.7 (12.7) |
|
Ten-meter walk test (seconds) |
17.4 (14.9) |
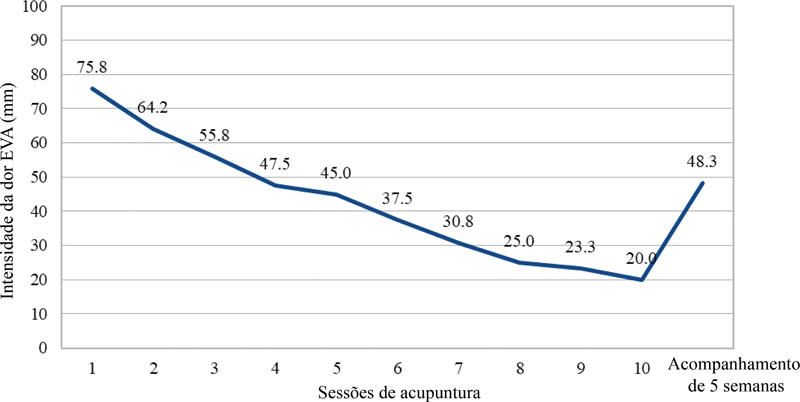
Pain intensity (VAS) reduced from 75.8 ± 18.8mm to 20.0 ± 22.6mm after 10 acupuncture sessions and 48.3 ± 26.6 mm in the follow-up ([Fig. 1]–ANOVA F = 7.99; p < 0.001). After treatment, there was a significant decrease in mean pain of 55.8 ± 28.4mm on the 100 mm VAS (p < 0.001), which corresponded to a reduction of 73.6%. At the follow-up assessment, the VAS increased, but did not return to baseline levels.

Mean WOMAC scores decreased significantly from 74.7 ± 12.7 (pre-treatment) to 45.7 ± 22.1 (post-treatment; p = 0.003) and 54.6 ± 22.9 (five-weeks follow-up; p = 0.02) ([Fig. 2]), demonstrating a lasting effect for more than five weeks.

Significant changes were not observed in mean ten-meter walk tests scores. Subjectively, all patients reported improvement in pain, and quality of life, and reduced pain killing drugs consumption. Eight participants did not use medication in the last week of treatment; and the four participant who needed daily medication reduced its consumption by 70%. No serious adverse effects of acupuncture treatment were observed; some patients felt pain or slight bleeding at the needle insertion sites, with spontaneous resolution within a few seconds.
#
Discussion
This case series confirmed our initial hypothesis of the potential therapeutic use of acupuncture in subjects with a severe HO indicated for THR, because of substantial improvement pain, functioning, and quality of life summed to reduction in analgesics and anti-inflammatory drugs consumption, but not in terms of walking speed.
Two randomized clinical trials compared real acupuncture with a control group. Fink et al.[13] and White et al.[16] demonstrated a reduction in mean EVA of 18 mm and 17 mm, respectively, after treatment with acupuncture, which was much less than 55.8 mm as we observed. Wider improvement in pain control is explained by the selection subjects with more intense pain (VAS = 75.8 ± 18.8 mm; while Fink had mean baseline of 54.6 ± 18.9 mm and White, 60.5 ± 14.2 mm), although total number and duration of sessions was similar.
Also, the choice of more effective acupuncture points may explain the more intense results. While Fink used a protocol of local and distant points for all patients (Ashi points on the hip, GB30, GB31, GB34, E40, B37, and B54), White let the therapist free to choose acupuncture points of his preference. Out of the TCM theories of energy harmonization, the cumulative and lasting effect of acupuncture can be explained by the reduction of nociceptive input, which may lead to improved mobilization of joints and lower limbs, which result in less limitation and progressive pain control. Additional acupuncture sessions may strengthen the initial analgesic effect and enhance a virtuous therapeutic cycle.
Functioning improvement assessed by WOMAC was documented in studies with anti-inflammatory[17] or analgesic drugs or pain controlling procedures like obturator nerve block,[18] which are therapeutic interventions in which the anatomic deformities of HO are not modified. For patients undergoing THR, mean WOMAC reduction ranges from 50 to 70 points after surgery.[19] This study demonstrated that acupuncture decreased WOMAC scores by 29 points.
Insertion of the acupuncture needle stimulates a wide peripheral neural network and reaches the central nervous system, promoting a phenomenon of neuromodulation at three levels - local, spinal, and supraspinal - resulting in the release of various substances, mainly neurotransmitters such as opioid peptides (enkephalin, dynorphin, and beta endorphin) and monoamines (serotonin, norepinephrine, histamine, dopamine), modulating motor, sensory, autonomic, neuroendocrine, and emotional functions.[20] For this, we use local hip points and distant points that act indirectly on the hip region or musculoskeletal structures. Points GB29 and GB30, are closely related to local neuromuscular structures: GB29 is superficially related to the tensor fasciae latae muscle, the lateral cutaneous nerve of the thigh; and deeply related to the muscular branches of the femoral nerve.[15] GB30 is superficially related to the gluteus maximus muscle and the inferior margin of the piriformis muscle, as well as with the middle cluneal nerves; and deeply related to the inferior gluteal and sciatic nerves.[15] Riberto et al.[21] described the presence of trigger points associated with myofascial pain syndrome and the symptom of persistent pain and disability in patients with HO, and later described the result of treating this syndrome with 1% lidocaine blockade for reduced pain and increased pressure pain measurement.[22] The muscles in which trigger points were most frequently identified in these studies were: piriformis (20%), iliopsoas (18%), long adductor (18%), gluteus medius (12%), gluteus minimus (12%), which are penetrated while needling of points GB29 and GB30.
The benefits demonstrated in this article are the result of ten acupuncture sessions, performed during five weeks, however, acupuncture can be maintained indefinitely, further prolonging its effect. Furthermore, this therapeutic modality has no absolute contraindications[23] and reports of serious adverse effects are rare.[24]
Given that this is a pilot project, this series of cases has limitations regarding its sample size and lack of comparison with control groups. The clinical follow-up period of patients was relatively short: only ten weeks; but for patients with such intense and prolonged complaints, the intensity and duration of the results were clinically significant. We suggest a randomized controlled trial to confirm the therapeutic superiority of real acupuncture over sham acupuncture or conventional treatment.
#
Conclusion
Acupuncture is an effective conservative rehabilitation strategy to reduce pain and improve quality of life in subjects with severe HO, and these benefits can lasts for at least five weeks post-treatment.
#
#
Authors' Contributions
RA wrote the manuscript, performed data collection and intervention. MR supervised the research, performed the statistical analysis of the data and revised the manuscript. All authors read and approved the final manuscript.
Work developed in the Hospital das Clínicas da Faculdade de Medicine of Ribeirão Preto da Universidade de São Paulo, RibeirãoPreto, SP, Brazil.
-
Referências
- 1 Bellamy N. WOMAC: a 20-year experiential review of a patient-centered self-reported health status questionnaire. J Rheumatol 2002; 29 (12) 2473-2476
- 2 Lima ABDU. Avaliação da qualidade de vida dos pacientes submetidos a artroplastia total primária do quadril antes e após a cirurgia [tese]. Botocatu, SP: Faculdade de Medicina, Universidade Estadual Paulista “Júlio de Mesquita Filho”;; 2015
- 3 Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med 2004; 141 (12) 901-910
- 4 Kooreman P, Baars EW. Patients whose GP knows complementary medicine tend to have lower costs and live longer. Eur J Health Econ 2012; 13 (06) 769-776
- 5 Manheimer E, Cheng K, Wieland LS. et al. Acupuncture for hip osteoarthritis. Cochrane Database Syst Rev 2018; 5 (05) CD013010
- 6 Kolasinski SL, Neogi T, Hochberg MC. et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. [published correction appears in Arthritis Care Res (Hoboken). 2021;73(5):764] Arthritis Care Res (Hoboken) 2020; 72 (02) 149-162
- 7 Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis 1957; 16 (04) 494-502
- 8 Coimbra I, Pastor E, Greve J. et al. Osteoartrite (artrose): tratamento. Rev Bras Reumatol 2004; 44 (06) 450-453
- 9 Boonstra AM, Schiphorst Preuper HR, Reneman MF, Posthumus JB, Stewart RE. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res 2008; 31 (02) 165-169
- 10 Fernandes MI. Tradução e validação do questionário de qualidade de vida específico para osteoartrose WOMAC (Western Ontario Mcmaster Universities) para a língua portuguesa [dissertação]. São Paulo: Escola Paulista de Medicina, Universidade Federal de São Paulo. São Paulo;; 2001
- 11 Salbach NM, Mayo NE, Higgins J, Ahmed S, Finch LE, Richards CL. Responsiveness and predictability of gait speed and other disability measures in acute stroke. Arch Phys Med Rehabil 2001; 82 (09) 1204-1212
- 12 Meng CF, Wang D, Ngeow J, Lao L, Peterson M, Paget S. Acupuncture for chronic low back pain in older patients: a randomized, controlled trial. Rheumatology (Oxford) 2003; 42 (12) 1508-1517
- 13 Fink MG, Kunsebeck H, Wipperman B, Gehrke A. Non-specific effects of traditional Chinese acupuncture in osteoarthritis of the hip. Complement Ther Med 2001; 9 (02) 82-89
- 14 Haslam R. A comparison of acupuncture with advice and exercises on the symptomatic treatment of osteoarthritis of the hip–a randomised controlled trial. Acupunct Med 2001; 19 (01) 19-26
- 15 Yamamura Y. Acupuntura tradicional: a arte de inserir. 2ª ed. São Paulo:: Roca;; 2001
- 16 White P, Bishop FL, Prescott P, Scott C, Little P, Lewith G. Practice, practitioner, or placebo? A multifactorial, mixed-methods randomized controlled trial of acupuncture. Pain 2012; 153 (02) 455-462
- 17 Svensson O, Malmenäs M, Fajutrao L, Roos EM, Lohmander LS. Greater reduction of knee than hip pain in osteoarthritis treated with naproxen, as evaluated by WOMAC and SF-36. Ann Rheum Dis 2006; 65 (06) 781-784
- 18 Crema CMT. Tratamento da dor crônica na osteoartrite do quadril: comparação da neurólise do nervo obturador com fenol e bloqueio de lidocaína. Ribeirão Preto:: Faculdade de Medicina de Ribeirão Preto;; 2019
- 19 Ilfeld BM, Ball ST, Gearen PF. et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg 2009; 109 (02) 586-591
- 20 Maeda Y, Kim H, Kettner N. et al. Rewiring the primary somatosensory cortex in carpal tunnel syndrome with acupuncture. Brain 2017; 140 (04) 914-927
- 21 Riberto M, Imamura M, Kaziyama HH, Imamura ST. Dor miofascial em pacientes com osteoartrose do quadril. Acta Fisiátrica 1997; 4 (02) 90-96
- 22 Imamura ST, Riberto M, Fischer AA, Imamura M, Kaziyama HHS, Teixeira MJ. Successful pain relief by treatment of myofascial components in patients with hip pathology scheduled for total hip replacement. Journal of Musculoskeletal Pain 1998; 6 (01) 73-79 Doi: http://dx.doi.org/10.1300/J094v06n01_06
- 23 Crawford III PF, Moss DA, Hawks MK, Snyder MJ. Integrative Medicine: Acupuncture. FP Essent 2021; 505: 18-22
- 24 Witt CM, Pach D, Brinkhaus B. et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplement Med 2009; 16 (02) 91-97
Endereço para correspondência
Publication History
Received: 03 February 2023
Accepted: 26 June 2023
Article published online:
30 October 2023
© 2023. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Bellamy N. WOMAC: a 20-year experiential review of a patient-centered self-reported health status questionnaire. J Rheumatol 2002; 29 (12) 2473-2476
- 2 Lima ABDU. Avaliação da qualidade de vida dos pacientes submetidos a artroplastia total primária do quadril antes e após a cirurgia [tese]. Botocatu, SP: Faculdade de Medicina, Universidade Estadual Paulista “Júlio de Mesquita Filho”;; 2015
- 3 Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med 2004; 141 (12) 901-910
- 4 Kooreman P, Baars EW. Patients whose GP knows complementary medicine tend to have lower costs and live longer. Eur J Health Econ 2012; 13 (06) 769-776
- 5 Manheimer E, Cheng K, Wieland LS. et al. Acupuncture for hip osteoarthritis. Cochrane Database Syst Rev 2018; 5 (05) CD013010
- 6 Kolasinski SL, Neogi T, Hochberg MC. et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. [published correction appears in Arthritis Care Res (Hoboken). 2021;73(5):764] Arthritis Care Res (Hoboken) 2020; 72 (02) 149-162
- 7 Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis 1957; 16 (04) 494-502
- 8 Coimbra I, Pastor E, Greve J. et al. Osteoartrite (artrose): tratamento. Rev Bras Reumatol 2004; 44 (06) 450-453
- 9 Boonstra AM, Schiphorst Preuper HR, Reneman MF, Posthumus JB, Stewart RE. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res 2008; 31 (02) 165-169
- 10 Fernandes MI. Tradução e validação do questionário de qualidade de vida específico para osteoartrose WOMAC (Western Ontario Mcmaster Universities) para a língua portuguesa [dissertação]. São Paulo: Escola Paulista de Medicina, Universidade Federal de São Paulo. São Paulo;; 2001
- 11 Salbach NM, Mayo NE, Higgins J, Ahmed S, Finch LE, Richards CL. Responsiveness and predictability of gait speed and other disability measures in acute stroke. Arch Phys Med Rehabil 2001; 82 (09) 1204-1212
- 12 Meng CF, Wang D, Ngeow J, Lao L, Peterson M, Paget S. Acupuncture for chronic low back pain in older patients: a randomized, controlled trial. Rheumatology (Oxford) 2003; 42 (12) 1508-1517
- 13 Fink MG, Kunsebeck H, Wipperman B, Gehrke A. Non-specific effects of traditional Chinese acupuncture in osteoarthritis of the hip. Complement Ther Med 2001; 9 (02) 82-89
- 14 Haslam R. A comparison of acupuncture with advice and exercises on the symptomatic treatment of osteoarthritis of the hip–a randomised controlled trial. Acupunct Med 2001; 19 (01) 19-26
- 15 Yamamura Y. Acupuntura tradicional: a arte de inserir. 2ª ed. São Paulo:: Roca;; 2001
- 16 White P, Bishop FL, Prescott P, Scott C, Little P, Lewith G. Practice, practitioner, or placebo? A multifactorial, mixed-methods randomized controlled trial of acupuncture. Pain 2012; 153 (02) 455-462
- 17 Svensson O, Malmenäs M, Fajutrao L, Roos EM, Lohmander LS. Greater reduction of knee than hip pain in osteoarthritis treated with naproxen, as evaluated by WOMAC and SF-36. Ann Rheum Dis 2006; 65 (06) 781-784
- 18 Crema CMT. Tratamento da dor crônica na osteoartrite do quadril: comparação da neurólise do nervo obturador com fenol e bloqueio de lidocaína. Ribeirão Preto:: Faculdade de Medicina de Ribeirão Preto;; 2019
- 19 Ilfeld BM, Ball ST, Gearen PF. et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg 2009; 109 (02) 586-591
- 20 Maeda Y, Kim H, Kettner N. et al. Rewiring the primary somatosensory cortex in carpal tunnel syndrome with acupuncture. Brain 2017; 140 (04) 914-927
- 21 Riberto M, Imamura M, Kaziyama HH, Imamura ST. Dor miofascial em pacientes com osteoartrose do quadril. Acta Fisiátrica 1997; 4 (02) 90-96
- 22 Imamura ST, Riberto M, Fischer AA, Imamura M, Kaziyama HHS, Teixeira MJ. Successful pain relief by treatment of myofascial components in patients with hip pathology scheduled for total hip replacement. Journal of Musculoskeletal Pain 1998; 6 (01) 73-79 Doi: http://dx.doi.org/10.1300/J094v06n01_06
- 23 Crawford III PF, Moss DA, Hawks MK, Snyder MJ. Integrative Medicine: Acupuncture. FP Essent 2021; 505: 18-22
- 24 Witt CM, Pach D, Brinkhaus B. et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplement Med 2009; 16 (02) 91-97