Keywords
spinal cord compression - erythropoiesis - arachnoid cysts
Palavras-chave
compressão da medula espinhal - eritropoiese - cistos aracnóideos
Introduction
Thalassemia is an inherited defect in the formation of hemoglobin, which has effects on various organs and systems in the human body. Normal hemoglobin electrophoresis reveals 97% of hemoglobin A, consisting of 2 α chains and 2 B chains; 2% of hemoglobin B, consisting of 2 α chains and 2 delta chains; and, finally, 1% of fetal hemoglobin, consisting of 2 α chains and 2 gamma chains.[1]
Thalassemia patients do not produce enough hemoglobin A because their cells cannot make the α or β chains. Thus, α thalassemias only affect the production of α chains, and β thalassemia only affects the production of β chains. Clinically, both α and β thalassemias may occur in major (homozygous), intermediate, and minor (heterozygous) forms.[1]
The HBB gene, on chromosome 11, is formed by 2 β alleles; however, in major β thalassemia, there is a mutation in this gene, which is formed by the Beta 0/Beta 0 or Beta 0/Beta + alleles. Other mutation combinations may cause the less severe forms of β thalassemia, such as the intermediate or minor subtypes.[2]
In major β thalassemia, there is formation of α chain tetramers that undergo chronic intramedullary and extravascular hemolysis. Patients have hemoglobin levels of 3 and 5 mg/dl, with 98% of fetal hemoglobin.[2]
Extramedullary hematopoiesis is a compensatory phenomenon, most commonly affecting the liver, the spleen and the lymph nodes. In severe cases, hematopoietic tissues may form in the intra-abdominal, paravertebral, pleural, nasopharyngeal, and epidural spaces. In addition to thalassemia, other diseases such as hemolytic anemia, polycythemia vera, and myelofibrosis also have extramedullary erythropoiesis.[3]
Spinal arachnoid cysts also are rare lesions, and represent between 1 and 3% of intrarachian expansive lesions.[4] They result from minor arachnoid membrane defects that induce cerebrospinal fluid (CSF) accumulation, which leads to arachnoid herniation. The mechanism for the formation of arachnoid cysts is not well understood; they increase in size during intense exercise and activity, or due to changes that cause elevations in intracranial pressure.[4] They may be primary, when they are congenital or idiopathic, or secondary, when they are associated with inflammatory reactions related to trauma, meningitis, subarachnoid hemorrhage or iatrogenesis (intradural surgery, postlumbar puncture).[4]
[5] They are more common in the thoracic spine (54 to 94%), especially in the posterior and posterolateral portions of the spinal canal.[4]
[5] Regarding their location, they can be classified as intradural or extradural, the latter of which are more common.[4] These lesions are often asymptomatic, causing root symptoms or spinal cord compression.[4]
[5] Consequently, they are commonly diagnosed incidentally.[4] In addition, they are underdiagnosed because they are easily missed on standard magnetic resonance images, due to their thin walls and pulsatile CSF motion.[5] Accidental and asymptomatic arachnoid cysts are usually treated conservatively, whereas symptomatic arachnoid cysts require surgical approaches. Thus, surgical interventions on spinal arachnoid cysts are uncommon.[4]
Case Report
RMS, 31 years old, male, with major β thalassemia with the need for biweekly blood transfusions, had been presenting progressive paraparesis for 2 months; evolving with a fall from his own height 1 month prior and since then restricted to a wheelchair; the patient evolved with urinary retention, so he was referred to the Baleia de Belo Horizonte Hospital for propaedeutics and treatment. Physical examination revealed grade 2 paraparesis in the lower limbs, Babinsky and bilateral clonus, as well as hypoesthesia with T2-sensory level.
The propedeutics performed showed an extensive intrarachial and extramedullary expansive lesion with homogeneous contrast uptake of the T3-T11, as well as a T1-T3 CSF cystic lesion. [Fig. 1].
 Fig. 1 Ressonância magnética na sequência T1 com contraste e T2 mostrando massa eritropoiética epidural T3-T11 e cisto aracnóideo T1-T3
Fig. 1 Ressonância magnética na sequência T1 com contraste e T2 mostrando massa eritropoiética epidural T3-T11 e cisto aracnóideo T1-T3
After the diagnosis of the spinal cord compression by proliferative hematopoietic tissue, the patient was immediately submitted to a fractional radiotherapy treatment of 10 sessions, totaling 3,500 Gy, in addition to a hypertransfusion with 600 ml of phenotyped red blood cell concentrate per week, for 3 weeks. The hypothesis was that eliminating the blocking of the subarachnoid space by the proliferative tissue, there would be a reduction of the arachnoid cyst by reducing the high intrarachial pressure that contributed to the expansion of the cystic lesion. In addition, the possibility of massive bleeding in a patient with very low hemoglobin levels made an initial conservative approach more appropriate. However, after the radiotherapy and hypertransfusion, the patient showed no improvement in neurological deficits, despite the excellent radiological response with almost complete disappearance of the intrarachial mass. Nevertheless, there was a persistence of the spinal cord compression by the cystic lesion on T1-T3, located just above the erythropoietic mass, [Fig. 2].
 Fig. 2 Ressonância magnética na sequência T2 mostrando regressão importante da massa eritropoiética epidural, mas manutenção do cisto aracnóideo T1-T3 com efeito compressivo sobre a medula espinhal.
Fig. 2 Ressonância magnética na sequência T2 mostrando regressão importante da massa eritropoiética epidural, mas manutenção do cisto aracnóideo T1-T3 com efeito compressivo sobre a medula espinhal.
The patient underwent hemilaminectomy from T1 to T3 and total microsurgical resection of the arachnoid cyst. Intraoperatively, this cyst was filled with a translucent liquid suggestive of CSF with no signs of blood or inflammatory reactions. After complete surgical resection, the spinal cord had a normal appearance without the previous anterior deviation resulting from the mass effect of the cystic lesion. There were no perioperative complications and the patient was discharged on the 3rd postoperative day, with sphincter control but maintaining grade 2 strength in the inferior limbs. The patient underwent intensive physical therapy and returned within 14 days with significant motor improvement, grade 4 muscle strength in the lower limbs, walking with occasional support but without assistance from others. [Fig. 3].
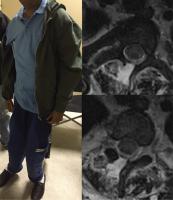 Fig. 3 Paciente RMS no 14° dia de pós-operatório, em ortostatismo sem apoio, em Rankin 3. Ressonância magnética mostrando descompressão satisfatória da medula, ao nível de T1-T3.
Fig. 3 Paciente RMS no 14° dia de pós-operatório, em ortostatismo sem apoio, em Rankin 3. Ressonância magnética mostrando descompressão satisfatória da medula, ao nível de T1-T3.
Arachnoid cyst resection by microsurgery was chosen, with hemilaminectomy of the affected levels. Postoperatively, the patient showed an improved sphincter control and improvement of the motor deficits, with a remarkable functional gain.
Discussion
The first description in the literature of spinal cord compression by an erythropoietic mass was made in 1954 by Gatto et al. The epidural “compartment” is affected in up to 15% of the cases of extramedullary erythropoiesis; however, it is asymptomatic in most cases. When there is spinal cord compression, the patient presents progressive paraparesis, as well as sphincter and sensory alterations below the level of the lesion.[6]
The diagnosis is made by magnetic resonance imaging (MRI) associated with the clinical history compatible with diseases that cause extramedullary hematopoiesis. An isointense epidural mass at T1 and hyperintense at T2 is visible, homogeneously capturing in the thoracic spine, associated with paravertebral masses of the same radiological aspect and bone hyperplasia.[7]
Surgical treatment was classically the most used because of its benefit of immediate decompression; however, because these patients are usually at high surgical risk, with very low basal hemoglobin levels, this treatment has been replaced by radiotherapy associated with hypertransfusion, with optimal clinical and radiological results, except when there is already plegia. In cases of intermediate thalassemia, hydroxyurea may also be associated to stimulate fetal hemoglobin production; a strategy that does not benefit patients with major β thalassemia, as they already have ∼ 98% fetal hemoglobin.[6]
[7]
Regarding the surgical treatment of arachnoid cysts, it has two basic objectives: performing spinal decompression and reestablishing the CSF flow.[5] Since arachnoid cysts do not contain proliferative and secretory cells, complete resection is not necessary to achieve these goals, since extensive fenestration or partial resection can cause complete collapse of the cyst.[4]
[5] These measures aim to avoid injuries, scarring and the formation of adhesions in neural structures, which may cause spinal cord anchorage and obstruction of the CSF flow.[4]
[5] For these reasons, complete resections of the limbs are restricted to those cases that span up to three vertebral segments, such as the case presented in the present report.[5]
In the literature, alternative treatment methods such as endoscopic fenestration and drainage of cysts with valve devices are pointed out. However, they introduce a foreign body into the subarachnoid space that may lead to adhesion formation and may also be related to the obstruction of the device by cyst collapse, intracranial hypotension syndromes, and slit ventricles. Endoscopic approaches have the risk of damaging medullary blood vessels present in the cyst walls and of performing fenestrations too small to prevent the reclection of cysts.[5] Thus, conventional surgical approaches remain the treatments of choice.
Conclusion
Despite the evidence showing excellent clinical response to the treatment of spinal cord compressions by hematopoietic tissue with radiotherapy and hypertransfusion, the case reported here needed to be individualized, as besides the erythropoietic tissue, there was also the arachnoid cyst causing compressive myelopathy. Thus, the combined treatment was chosen, initially with 3,500 Gy and 1,800 ml of packed red blood cells, both fractionally, followed by surgical decompression with total resection of the arachnoid cyst, with excellent radiological, clinical and functional results.[4]
[5]






