

Subscribe to RSS
DOI: 10.1055/s-0043-57243
Corrective Osteotomy in a Dog to Address Increased Distal Femoral Procurvatum Ascribed to a Distal Femoral Salter-Harris Type V Injury
Authors

Abstract
Increased distal femoral procurvatum has been reported sporadically in dogs following malunion of Salter-Harris type I, II, and III fractures of distal femur. The resultant increased procurvatum can be poorly tolerated because of subsequent loss of stifle extension. This case report represents a dog with the increased procurvatum of the distal femur ascribed to a previous Salter-Harris type V injury. Surgical planning and successful outcome following the corrective procedures have been documented. A 6.5-month-old fox-terrier presented with a persistent weight bearing left pelvic limb lameness, 2 months after being hit by a car. The predominant orthopaedic finding was a 20-degree decrease in left stifle extension. Radiographic and computerized tomography evaluation revealed premature eccentric closure of the left distal femoral physis ascribed to a previous Salter-Harris type V injury. The left femoral procurvatum was 30 degrees. The left tibial plateau angle was increased by 11.5 degrees compared with the right. The femoral deformity was characterized, and a corrective procedure was planned using Paley's centre of rotation of angulation methodology. A cranial closing wedge ostectomy of the left distal femur was performed and stabilized using a locking plate. Proximal tibial epiphysiodesis was also performed to reduce the tibial plateau slope. Union of the osteotomy site and reduction in tibial plateau angle by 5.4 degrees were documented 50 days after surgery with a good functional outcome.
Introduction
Distal femoral physeal fractures in dogs are predominantly Salter-Harris (SH) type II or occasionally SH type I fractures.[1] [2] SH type III and IV fractures of the distal femur are infrequently reported, and there are no reports for SH type V fractures in dogs.[1] [2] [3] [4] [5] [6] Early surgical reduction and stabilization of these fractures are recommended to restore normal femoral morphology and prevent malunion.[2] [4] [7] Typically, malunion results in caudoproximal epiphyseal displacement, producing pronounced procurvatum of the distal femur.[3] [5] Caudoproximal displacement occurs because of tension exerted by semi-tendinosus and semi-membranosus muscles on the caudal aspect of the proximal tibia.[3] [4] [5]
Another consequence of distal femoral physeal fractures is premature physeal closure which can contribute to osseous deformity.[2] [8] Symmetric premature closure of distal femoral physis can result in a shortened femur. If the length discrepancy is less than 20%, limb function can be preserved by compensatory increases in ipsilateral joint angles and/or, less frequently, by tibial overgrowth.[2] [3] [9] [10] [11] [12] Asymmetric premature distal femoral physeal closure can cause femoral deformity in the frontal plane, transverse plane or combination which may affect alignment of the quadriceps mechanism and lead to patellar luxation.[4] [11] In addition, asymmetric distal femoral physeal closure can cause sagittal plan deformity which has been rarely reported.[7] [13] In humans, knee sagittal malalignment is generally tolerated better than frontal malalignment because the hip, knee and ankle move in the sagittal plane and can therefore compensate for sagittal malalignment.[14] Knee kinematics studies in dogs[15] may suggest that a similar concept could be applied to sagittal plane deformities in dogs. The loss of stifle extension caused by severe distal femoral procurvatum, however, has been associated with poor limb usage in both humans and dogs.[3] [14] Increased femoral procurvatum in humans can disrupt the femoral–patellar relationship and result in a knee fixed flexion deformity, which is often debilitating.[14] In dogs, persistent lameness was ascribed to a loss of more than 10 degrees of stifle extension.[16] Stifle extension may be further hindered by hamstring contracture and joint capsule fibrosis due to limb disuse.[3] [5]
There are a limited number of reports describing increased distal femoral procurvatum and its surgical correction in dogs.[3] [4] [5] None of the reports describe increased distal femoral procurvatum resultant from SH type V injury of the distal femoral physis. This case report describes a dog with asynchronous premature closure of the distal femoral physis ascribed to a distal femoral SH type V injury, which resulted in increased distal femoral procurvatum. We further discuss the diagnostic considerations, preoperative planning and corrective procedure which yielded functional recovery in this dog.
Case Description
A 4-month-old intact male fox-terrier, weighing 6.6 kg, was presented to the University of Padova Veterinary Teaching Hospital after being hit by a car. On orthopaedic examination, the dog would not bear weight on the left pelvic limb. Pain was elicited on stifle manipulation. The stifle was palpably stable in the sagittal and frontal planes and the patella position was normal. Radiographic evaluation of both pelvic limbs obtained under sedation revealed irregularities in the left distal femoral physis ([Fig. 1B,C]). Because there was no demonstrable clinical instability, conservative therapy with cage confinement and administration of meloxicam (1 mg/kg per os every 24 hours for 10 days) was recommended.

The dog re-presented 2 months later with a persistent weight-bearing lameness of the left pelvic limb. There was moderate muscular atrophy in the left pelvic limb. The most prominent finding of orthopaedic examination was a 20-degree decrease in left stifle extension ([Fig. 1E]). Flexion angles were comparable in both stifles. Joint effusion, patellar luxation and other orthopaedic abnormalities were not appreciated in the affected stifle.
Radiographic Findings
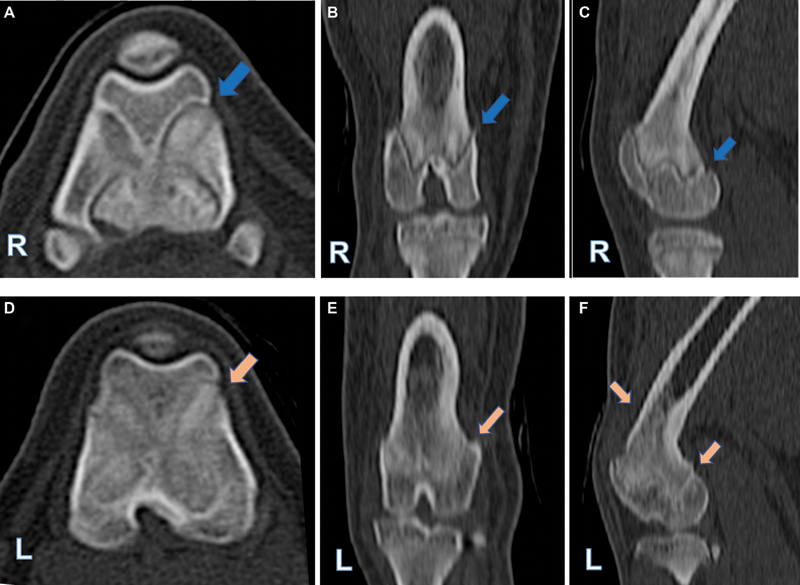
Orthogonal radiographs of both pelvic limbs were obtained under sedation ([Fig. 1F–I]). On the frontal plane radiograph, no valgus or varus deformity of the left femur was detected. On sagittal plane radiographs, increased procurvatum of the left distal femur was present. Definition of the left distal femoral physis was indistinct along with sclerosis of the distal metaphysis, increased opacity and irregularity of the caudal aspect of distal physis and caudal cortical thickening of the distal femur adjacent to the deformity. Asymmetric premature closure of caudal portion of the left distal femoral physis ascribed to a previous crushing type (SH type V) injury was diagnosed. Radiographic evaluation of the tibiae was normal in the frontal plane, but the left tibial plateau angle (TPA) was higher than right TPA in sagittal radiographs ([Table 1], [Fig. 1I]). Additionally, a slight compensatory increase in the length of left tibia was documented ([Table 1]). Computed tomography scan evaluation of both femurs verified the radiographic findings of eccentric premature closure of left distal femoral physis ([Fig. 2]).
Abbreviations: aCdDFA, anatomical caudal distal femoral angle; NA, data not available; TPA, tibial plateau angle.
Note: Femoral and tibial length were measured on frontal radiographs, while aCdDFA and TPA were measured on sagittal radiographs. Two months after injury, the left (affected) femur was 0.01% shorter than the right (unaffected) femur, with 0.03% compensatory overgrowth of the ipsilateral tibia. The affected femur was 0.01 and 0.02% shorter than the right femur on radiographs performed immediately and 50 days after surgery respectively.
Surgical Planning
Using the sagittal radiographic images of both femurs, centre of rotation of angulation (CORA) methodology was employed to define the location and magnitude of the procurvatum deformity in the left femur.[3] Paley's methodology was used to define the joint orientation line (JOL) and anatomical axis (AA) of the distal femur and to measure the anatomical caudal distal femoral angle (aCdDFA).[3] [14] [17] The normal right aCdDFA (90.5 degrees) was used to measure the amount of deformity in the left femur. The CORA, formed by intersecting the left femoral distal AA with the transposed right aCdDFA, was located 12 mm proximal to the lateral trochlear ridge. As determined by CORA, the excessive procurvatum of the left distal femur was measured 30 degrees, which was also the amount of correction needed to be addressed.[1] [3] A cranial closing wedge ostectomy (CCWO) was planned with the apex of the wedge positioned along the caudal cortex of the femur. The height of cranial wedge (y = 7 mm) was calculated using the trigonometric formula (y = x ∙ tan θ) where θ is the desired angle of correction (30 degrees) and x is the femoral width (12.13 mm) measured on calibrated radiographs along the transverse bisecting line.[12] Because the left TPA was 11.5 degrees greater than the contralateral tibia, a proximal tibial epiphysiodesis (PTE) was also planned ([Fig. 3]).

Surgery
The dog was premedicated by intramuscular injection of methadone (0.2 mg/kg), dexmedetomidine (4 µg/kg), and ketamine (1 mg/kg). Anaesthesia was induced with propofol (3 mg/kg intravenous) and was maintained with sevoflurane. Cefazolin (22 mg/kg, intravenous) was administered at the time of induction and then repeated every 90 minutes. The dog was prepared for aseptic surgery and positioned in dorsal recumbency. A lateral approach to the left femur was performed which was extended to the craniolateral aspect of the stifle. Two parallel Steinmann pins were placed in the cranial surface of the femur and connected to a tibial plateau levelling osteotomy jig to maintain the alignment and facilitate reduction. For CCWO, the initial osteotomy was made at the CORA location along the pre-determined transverse bisecting. The second osteotomy was made proximal to the first osteotomy in a 30-degree oblique fashion to excise a 7 mm cranial wedge. After reduction, a straight 6-hole Mini-series Fixin plate (Intrauma S.r.l., Rivoli, Italy) was applied laterally on the femur using 2.5 mm locking screws. The PTE was then performed under the fluoroscopy guide. A 2.4 mm cortical screw (DePuy Synthes, West Chester, United States) was inserted cranially in the tibial plateau and directed parallel to the proximal tibial shaft using a limited medial approach.[18] The fascia, subcutaneous tissue and skin were closed routinely in layers.
Outcome
Immediate postoperative radiographs revealed excellent femoral alignment and bone apposition in the frontal plane. The postoperative left aCdDFA was 95.5 degrees as measured on the sagittal view radiograph, indicating that procurvatum of the left distal femur had been erroneously overcorrected resulting in 5 degrees of recurvatum ([Table 1], [Fig. 4A,B]). After surgery, adequate analgesic, anti-inflammatory and prophylactic antibiotic therapy was administered. The dog was placing nominal weight on the affected limb when discharged the day following surgery. The limb was not bandaged. The owners were advised to restrict the dog's activity to short leash walks for 8 weeks.

Within 3 days of surgery, the dog started to bear weight on the affected limb. A weight- bearing lameness was present 10 days after surgery. The dog was re-evaluated 50 days after surgery and did not have appreciable lameness when walking and trotting and both stifles could be extended completely. Radiographs obtained at this time revealed union of the osteotomy with a 4.9-degree reduction in the femoral recurvatum. Healing was notable by adequate formation of bridging callus which was suggestive of secondary bone healing related to use of a fixed-angle construct. The left TPA was reduced by 5.4 degrees ([Table 1], [Fig. 4C–E]). The owners were advised to gradually increase the dog's activity over the next 2 weeks and then the dog could resume normal activity. Mid-term follow-up was obtained by phone, 6 months after surgery and the owner reported that the dog's left pelvic limb was normal.
Discussion
The dog in this case report likely sustained a SH type V injury resulting in premature closure at the caudal aspect of the distal femoral physis. We assume that continued growth from the cranial portion of the distal femoral physis resulted in accentuated distal femoral procurvatum. The injury sustained by the dog reported in the current report varies from the previously reported 7 cases of increased distal femoral procurvatum, in which the deformity was caused by malunion of SH type I,[3] [5] type II,[3] or type III[4] fractures.
Femoral shortening secondary to distal femoral SH malunion was present in all seven previously reported dogs.[3] [4] [5] The dog in the current case report had 1.5 mm decrease of femoral length in the affected limb which is nominal. Additionally, tibial overgrowth has been described as a compensatory mechanism for femoral shortening.[2] [12] In our case, 4.6 mm of tibial overgrowth had occurred 2 months after injury ([Table 1]). An increased TPA identified in our case has not been reported previously. We assume that the increased TPA was caused by an unrecognized injury to proximal tibial physis sustained when the dog was hit by a car or by anomalous biomechanical forces affecting the proximal tibial physis resultant from increased femoral procurvatum. These forces may have caused a delay in the growth of the caudal part of the tibial physis, while the cranial part continued to grow. This phenomenon, known as ‘Hueter-Volkmann Law’, is well described in humans. Body weight forces in human tibiae can retard growth in the posterior portion of tibial condyles, resulting in posterior rotation and so-called ‘rhomboid transformation’ of tibial condyles.[19] [20]
Because femoral sagittal plane deformity has been poorly described in dogs, Paley's methodology used in human orthopaedics was adopted to define and correct the femoral sagittal plane deformity in dogs.[3] [14] We found accurately measuring the increase in procurvatum and planning the sagittal plane correction challenging for two reasons.[7] [21] First, there is lacking information regarding assessing normal femoral sagittal plane alignment and femoral sagittal plane deformity in dogs.[3] [15] Normal breed reference values are also lacking.[3] [7] [13] [21] Second, methodologies proposed to measure femoral sagittal plane alignment in dogs are variable.[3] [7] [17] [21] [22] In a recent study, Paley's landmarks for defining distal JOL[3] [21] and distal AA of the dog's femur[3] [22] were assumed to be inaccurate because distal JOL landmarks may be obscured by osteophytosis or alterations/abnormalities of the distal physis.[7] [14] Interobserver variability may exist in AA identification. Although a consistent and accurate approach for measuring femoral sagittal plane alignment in dogs has been reported, the reliability of this methodology in femurs with deformity and across breeds needs to be investigated.[7]
We performed a CCWO to address increased procurvatum of the femur which yielded an excellent functional outcome. In previous cases involving surgical management of dogs with distal femoral procurvatum, caudal closing wedge ostectomy (1 case),[3] CCWO (2 cases),[3] [4] and simple ostectomy for addressing quadriceps impingement without corrective osteotomy (4 cases)[5] were applied. Slight femoral recurvatum (5 degrees) was present after surgery in our case which is similar to the result obtained by others.[3] [23] This illustrates the technical challenges in correcting distal femoral procurvatum deformity due to the femur's inherent procurvatum and the short length of the distal segment, which can limit distal osteotomies and cause a shift in CORA location. We believe the femoral recurvatum in the current report was produced by removing a larger wedge of the bone during the corrective procedure. The accuracy of the corrective osteotomy can be improved by use of a three-dimensional-printed guide instead of the free-hand technique.[24] Although the minor degree of recurvatum was well tolerated and did not appear to have an adverse impact on limb function, increased recurvatum should be avoided.[23] The extent of the recurvatum has been shown to reduce over time by bone remodelling, particularly in dogs with continued longitudinal growth.[23]
The PTE has been advocated for reducing the TPA in skeletally immature dogs with cranial cruciate ligament deficiency.[18] The dog in our study did not have any clinical abnormalities consistent with cranial cruciate insufficiency during the study. We decided to perform the PTE as a tentative procedure to reduce the high tibial slope. In our case, PTE induced a 5.4-degeee decrease in the left TPA which is indicative that some amounts of residual growing potential were still available at the time of PTE. According to Vezzoni and colleagues, the younger the animal at the time of PTE, the greater the potential for TPA reduction. However, no similar data are available regarding the performance of PTE in small-breed dogs.[18] The increased distal femoral procurvatum resulted in restricted stifle extension and persistent lameness in the dog described in this case report. The CCWO yielded an excellent functional outcome in this dog. The stifle extension was increased by 20 degrees and overall limb function was markedly improved. Our results are consistent with prior reports describing dogs with distal femoral procurvatum having good to excellent outcomes following surgery.[3] [4] [5] While the CORA methodology proved useful, the inaccuracy we experienced suggests that further studies are warranted to refine femoral sagittal plane deformity correction in dogs.
Conflict of Interest
None declared.
Authors' Contributions
Parastoo Memarian, DVM, performed the measurements, assisted in surgery, wrote the manuscript, revised and approved the final manuscript; Daniel D. Lewis, DVM, Diplomate American College of Veterinary Surgeons, American College Veterinary Surgeons Founding Fellow, Minimally Invasive Surgery (Small Animal Orthopedics), assisted in records' interpretation, revised the manuscript, read and approved the final manuscript; Massimo Bucci, DVM, PhD, performed the anaesthesia, collaborated in writing the manuscript, read and approved the final manuscript; Maurizio Isola, DVM, PhD, performed the planning and the surgery, revised the manuscript, read and approved the final manuscript.
-
References
- 1 Johnston SA, Tobias KM. Veterinary Surgery Small Animal. 2nd ed. Elsevier, St. Louis, MO; 2018: 2887-2910
- 2 Berg RJ, Egger EL, Konde LJ, McCurnin DVM. Evaluation of prognostic factors for growth following distal femoral physeal injuries in 17 dogs. Vet Surg 1984; 13 (03) 172-180
- 3 Kim SE, Lewis DD. Corrective osteotomy for procurvatum deformity caused by distal femoral physeal fracture malunion stabilised with String-of-Pearls locking plates: results in two dogs and a review of the literature. Aust Vet J 2014; 92 (03) 75-80
- 4 Smalle TM, Coetzee GL, Naude SH. Corrective wedge ostectomy for an atypical femoral procurvatum deformity stabilised with a supracondylar bone plate. J S Afr Vet Assoc 2018; 89 (00) e1-e6
- 5 Jones SC, Tryon EK, Kieves NR, Dyce J. Simple ostectomy to address quadriceps impingement caused by distal femoral malunion in four dogs. J Small Anim Pract 2021; 62 (05) 397-402
- 6 Lazarus MA, Lewis DD, Johnson MD, Porter EG. Use of a circular fixator construct to facilitate closed reduction and percutaneous stabilization of a distal femoral physeal fracture in a dog. Open Vet J 2021; 11 (01) 89-95
- 7 Peterson JL, Torres BT, Hutcheson KD, Fox DB. Radiographic determination of normal canine femoral alignment in the sagittal plane: a cadaveric pilot study. Vet Surg 2020; 49 (06) 1230-1238
- 8 Johnson JM, Johnson AL, Eurell JA. Histological appearance of naturally occurring canine physeal fractures. Vet Surg 1994; 23 (02) 81-86
- 9 Culvenor JA, Hulse DA, Patton CS. Closure after injury of the distal femoral growth plate in the dog. J Small Anim Pract 1978; 19 (10) 549-560
- 10 Blaeser LL, Gallagher JG, Boudrieau RJ. Treatment of biologically inactive nonunions by a limited en bloc ostectomy and compression plate fixation: a review of 17 cases. Vet Surg 2003; 32 (01) 91-100
- 11 DeTora MD, Boudrieau RJ. Complex angular and torsional deformities (distal femoral malunions). Preoperative planning using stereolithography and surgical correction with locking plate fixation in four dogs. Vet Comp Orthop Traumatol 2016; 29 (05) 416-425
- 12 Petazzoni M, Palmer RH. Femoral angular correction and lengthening in a large-breed puppy using a dynamic unilateral external fixator. Vet Surg 2012; 41 (04) 507-514
- 13 Aghapour M, Bockstahler B, Vidoni B. Evaluation of the femoral and tibial alignments in dogs: a systematic review. Animals (Basel) 2021; 11 (06) 1-24
- 14 Paley D. Normal lower limb alignment and joint orientation. In: Principles of Deformity Correction. Springer, Berlin, Heidelberg; 2002: 1-18
- 15 Kim SE, Jones SC, Lewis DD. et al. In-vivo three-dimensional knee kinematics during daily activities in dogs. J Orthop Res 2015; 33 (11) 1603-1610
- 16 Jandi AS, Schulman AJ. Incidence of motion loss of the stifle joint in dogs with naturally occurring cranial cruciate ligament rupture surgically treated with tibial plateau leveling osteotomy: longitudinal clinical study of 412 cases. Vet Surg 2007; 36 (02) 114-121
- 17 Petazzoni M, Jaeger GH. Atlas of Clinical Goniometry and Radiographic Measurements of the Canine Pelvic Limb. 2nd ed. Milan: : Merial; 2008: 1-97
- 18 Vezzoni A, Bohorquez Vanelli A, Modenato M, Dziezyc J, Devine Slocum T. Proximal tibial epiphysiodesis to reduce tibial plateau slope in young dogs with cranial cruciate ligament deficient stifle. Vet Comp Orthop Traumatol 2008; 21 (04) 343-348
- 19 Nagamine R, Kawasaki M, Kim K-I, Sakai A, Suguro T. The posterior tibial slope is mainly created by the posterior rotation of the tibial condyles. J Orthop Surg (Hong Kong) 2020; 28 (03) 2309499020975580
- 20 D'Andrea CR, Alfraihat A, Singh A. et al. Part 1. Review and meta-analysis of studies on modulation of longitudinal bone growth and growth plate activity: a macro-scale perspective. J Orthop Res 2021; 39 (05) 907-918
- 21 Kara ME, Sevil-Kilimci F, Dilek ÖG, Onar V. Proximal and distal alignment of normal canine femurs: a morphometric analysis. Ann Anat 2018; 217: 125-128
- 22 Yasukawa S, Edamura K, Tanegashima K. et al. Evaluation of bone deformities of the femur, tibia, and patella in Toy Poodles with medial patellar luxation using computed tomography. Vet Comp Orthop Traumatol 2016; 29 (01) 29-38
- 23 Pavarotti GS, Boudrieau RJ. Treatment of a paediatric distal femoral malunion deformity. Vet Comp Orthop Traumatol 2018; 31 (03) 222-228
- 24 Memarian P, Pishavar E, Zanotti F. et al. Active materials for 3D printing in small animals: current modalities and future directions for orthopedic applications. Int J Mol Sci 2022; 23 (03) 1045
Address for correspondence
Publication History
Received: 08 November 2022
Accepted: 26 February 2023
Article published online:
02 May 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Johnston SA, Tobias KM. Veterinary Surgery Small Animal. 2nd ed. Elsevier, St. Louis, MO; 2018: 2887-2910
- 2 Berg RJ, Egger EL, Konde LJ, McCurnin DVM. Evaluation of prognostic factors for growth following distal femoral physeal injuries in 17 dogs. Vet Surg 1984; 13 (03) 172-180
- 3 Kim SE, Lewis DD. Corrective osteotomy for procurvatum deformity caused by distal femoral physeal fracture malunion stabilised with String-of-Pearls locking plates: results in two dogs and a review of the literature. Aust Vet J 2014; 92 (03) 75-80
- 4 Smalle TM, Coetzee GL, Naude SH. Corrective wedge ostectomy for an atypical femoral procurvatum deformity stabilised with a supracondylar bone plate. J S Afr Vet Assoc 2018; 89 (00) e1-e6
- 5 Jones SC, Tryon EK, Kieves NR, Dyce J. Simple ostectomy to address quadriceps impingement caused by distal femoral malunion in four dogs. J Small Anim Pract 2021; 62 (05) 397-402
- 6 Lazarus MA, Lewis DD, Johnson MD, Porter EG. Use of a circular fixator construct to facilitate closed reduction and percutaneous stabilization of a distal femoral physeal fracture in a dog. Open Vet J 2021; 11 (01) 89-95
- 7 Peterson JL, Torres BT, Hutcheson KD, Fox DB. Radiographic determination of normal canine femoral alignment in the sagittal plane: a cadaveric pilot study. Vet Surg 2020; 49 (06) 1230-1238
- 8 Johnson JM, Johnson AL, Eurell JA. Histological appearance of naturally occurring canine physeal fractures. Vet Surg 1994; 23 (02) 81-86
- 9 Culvenor JA, Hulse DA, Patton CS. Closure after injury of the distal femoral growth plate in the dog. J Small Anim Pract 1978; 19 (10) 549-560
- 10 Blaeser LL, Gallagher JG, Boudrieau RJ. Treatment of biologically inactive nonunions by a limited en bloc ostectomy and compression plate fixation: a review of 17 cases. Vet Surg 2003; 32 (01) 91-100
- 11 DeTora MD, Boudrieau RJ. Complex angular and torsional deformities (distal femoral malunions). Preoperative planning using stereolithography and surgical correction with locking plate fixation in four dogs. Vet Comp Orthop Traumatol 2016; 29 (05) 416-425
- 12 Petazzoni M, Palmer RH. Femoral angular correction and lengthening in a large-breed puppy using a dynamic unilateral external fixator. Vet Surg 2012; 41 (04) 507-514
- 13 Aghapour M, Bockstahler B, Vidoni B. Evaluation of the femoral and tibial alignments in dogs: a systematic review. Animals (Basel) 2021; 11 (06) 1-24
- 14 Paley D. Normal lower limb alignment and joint orientation. In: Principles of Deformity Correction. Springer, Berlin, Heidelberg; 2002: 1-18
- 15 Kim SE, Jones SC, Lewis DD. et al. In-vivo three-dimensional knee kinematics during daily activities in dogs. J Orthop Res 2015; 33 (11) 1603-1610
- 16 Jandi AS, Schulman AJ. Incidence of motion loss of the stifle joint in dogs with naturally occurring cranial cruciate ligament rupture surgically treated with tibial plateau leveling osteotomy: longitudinal clinical study of 412 cases. Vet Surg 2007; 36 (02) 114-121
- 17 Petazzoni M, Jaeger GH. Atlas of Clinical Goniometry and Radiographic Measurements of the Canine Pelvic Limb. 2nd ed. Milan: : Merial; 2008: 1-97
- 18 Vezzoni A, Bohorquez Vanelli A, Modenato M, Dziezyc J, Devine Slocum T. Proximal tibial epiphysiodesis to reduce tibial plateau slope in young dogs with cranial cruciate ligament deficient stifle. Vet Comp Orthop Traumatol 2008; 21 (04) 343-348
- 19 Nagamine R, Kawasaki M, Kim K-I, Sakai A, Suguro T. The posterior tibial slope is mainly created by the posterior rotation of the tibial condyles. J Orthop Surg (Hong Kong) 2020; 28 (03) 2309499020975580
- 20 D'Andrea CR, Alfraihat A, Singh A. et al. Part 1. Review and meta-analysis of studies on modulation of longitudinal bone growth and growth plate activity: a macro-scale perspective. J Orthop Res 2021; 39 (05) 907-918
- 21 Kara ME, Sevil-Kilimci F, Dilek ÖG, Onar V. Proximal and distal alignment of normal canine femurs: a morphometric analysis. Ann Anat 2018; 217: 125-128
- 22 Yasukawa S, Edamura K, Tanegashima K. et al. Evaluation of bone deformities of the femur, tibia, and patella in Toy Poodles with medial patellar luxation using computed tomography. Vet Comp Orthop Traumatol 2016; 29 (01) 29-38
- 23 Pavarotti GS, Boudrieau RJ. Treatment of a paediatric distal femoral malunion deformity. Vet Comp Orthop Traumatol 2018; 31 (03) 222-228
- 24 Memarian P, Pishavar E, Zanotti F. et al. Active materials for 3D printing in small animals: current modalities and future directions for orthopedic applications. Int J Mol Sci 2022; 23 (03) 1045